|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
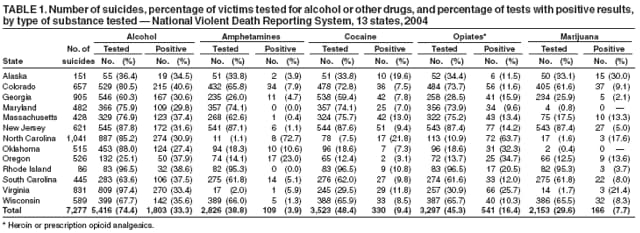
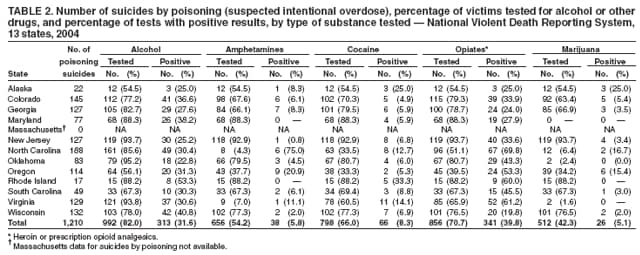
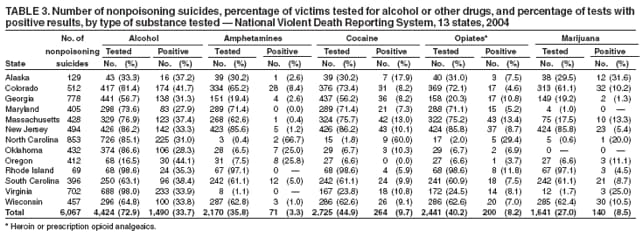
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail. Toxicology Testing and Results for Suicide Victims --- 13 States, 2004In 2003, an estimated 31,484 suicides (10.7 per 100,000 population) occurred in the United States (1). Suicide was the fourth leading cause of death among persons aged 10--64 years and the second and third leading causes of death among persons aged 25--34 and 10--24 years, respectively (2). Few studies have attempted to determine the contribution of substance use to suicide (3,4). To assess toxicology testing practices and to determine the prevalence of positive results for alcohol or other drugs, CDC analyzed test results of suicide victims in the 13 states that collected data for the National Violent Death Reporting System (NVDRS) in 2004. This report summarizes the results of that analysis, which determined that 1) the percentage of suicide victims tested varied among states, ranging from 25.9% to 97.7%; 2) of those victims tested, 33.3% were positive for alcohol, and 16.4% were positive for opiates; and 3) similar percentages of poisoning suicide (i.e., suspected intentional overdose) and nonpoisoning suicide victims tested positive for alcohol or other drugs, with the exception of opiates. These results underscore the need to continue monitoring toxicology test results of suicide victims, which might identify patterns of substance use that can help guide development of effective suicide interventions. Such data can be enhanced by uniform, comprehensive, toxicology testing practices on a state and national basis. NVDRS is a state-based surveillance system that collects information on all violent deaths (i.e., homicides, suicides, legal interventions, unintentional deaths by firearm, or deaths of undetermined intent) in participating states, combining data from death certificates with toxicology results from coroners and medical examiners (5,6). The study described in this report was based on 2004 data collected from 13 states* as of July 2006; these states represented 23.4% of the U.S. population. Suicides were included when listed by coroners or medical examiners as the manner of death; whether a suicide resulted from poisoning or nonpoisoning was determined by the cause of death listed. During 2004, NVDRS received data on 7,277 deaths by suicide. In certain states, toxicology testing was performed routinely on nearly all suicide victims; in other states, testing was performed selectively, an apparent targeting of suicides in which use of alcohol or other drugs was suspected as likely causing or contributing to the deaths. Of the 7,277 victims, testing for at least one substance was performed on 5,550 (76.3%). The percentage of suicide deaths for which at least one test was completed varied among states from 25.9% to 97.7%.† Overall, the percentage of suicide victims tested varied by type of substance tested: alcohol (74.4%), cocaine (48.4%), opiates (i.e., heroin or prescription opioid analgesics) (45.3%), amphetamines (38.8%), and marijuana (29.6%) (Table 1). The percentage of victims tested also varied among states by type of substance tested, ranging from 97.4% to 25.1% for alcohol, 95.3% to 1.1% for amphetamines, 96.5% to 7.5% for cocaine, 96.5% to 10.9% for opiates, and 95.3% to 0.4% for marijuana. Among all suicide victims with positive test results, the greatest percentage tested positive for alcohol (33.3%), followed by opiates (16.4%), cocaine (9.4%), marijuana (7.7%), and amphetamines (3.9%). Among states (excluding those in which fewer than 20 victims were tested), the percentage of positive tests ranged from 27.4% to 40.6% for alcohol, none to 23.0% for amphetamines, 3.1% to 21.8% for cocaine, and 9.6% to 63.7% for opiates. Numbers of positive tests for marijuana in individual states were too small to be considered (Table 1). Greater percentages of victims of suicides caused by poisoning were tested (Table 2) than nonpoisoning suicide victims (Table 3). Tests for alcohol were conducted in 82.0% of poisoning suicides and 72.9% of nonpoisoning suicides. Similar differences were observed for amphetamines (54.2% versus 35.8%), cocaine (66.0% versus 44.9%), opiates (70.7% versus 40.2%), and marijuana (42.3% versus 27.0%). However, despite greater testing in poisoning suicides, with the exception of opiates, the proportions of tests with positive results were similar for poisoning and nonpoisoning suicides, respectively: 31.6% versus 33.7% for alcohol, 5.8% versus 3.3% for amphetamines, and 8.3% versus 9.7% for cocaine. For opiates, 39.8% of poisoning victims tested positive, compared with 8.2% of nonpoisoning victims (Tables 2 and 3). Reported by: D Karch, PhD, A Crosby, MD, T Simon, PhD, Div of Violence Prevention, National Center for Injury Prevention and Control, CDC. Editorial Note:In this study, substantial percentages of suicide victims tested positive for alcohol or other drugs. The most frequently identified substance was alcohol, found in one third of those tested; four other substances were identified in approximately 10% of tested victims. These test results are consistent with previous studies demonstrating use of alcohol or other drugs by suicide victims (7,8). Among states, substantial variation was observed in both the percentage of suicide victims tested for alcohol or other drugs and the specific substances included in testing. In addition, states were more likely to test victims of suspected poisoning suicide than nonpoisoning suicide. However, the similarities in positive test results involving four of the five substance types in poisoning and nonpoisoning suicides suggest that use of alcohol or other drugs might contribute substantially to suicides overall, regardless of cause of death. The finding that opiates (the fifth substance type) were nearly five times more prevalent among poisoning suicide victims is consistent with evidence that prescription opioid analgesics cause more intentional overdose deaths than illegal non-opioid drugs (CDC, unpublished data, 2006). The relationship between substance use and other suicide risk factors is complex; the chronology and causal pathway of events leading to suicide are difficult to determine. To better understand the results of this study, CDC is funding a survey of coroner and medical examiner toxicology laboratories to examine practices and protocols regarding testing of suicide victims. The findings in this report are subject to at least three limitations. First, high percentages of positive results in a state might reflect targeted testing rather than greater drug use in that state. Second, manner of death for certain suspected suicides might have been listed as undetermined, excluding those cases from the study; the scope of this limitation has been documented previously (9). Finally, the alcohol or other drugs in the bodies of victims were only recorded as present or absent; no evaluations were conducted to determine whether the concentrations present were lethal or intoxicating. Despite evidence of substance use among substantial numbers of suicide victims, none of the 13 states reporting to NVDRS in 2004 conducted comprehensive alcohol and drug screenings on all suicide victims. Previous studies of subpopulations by specific substance, geographic area, race/ethnicity, and age have documented the limited toxicology screening performed in certain states. Descriptions of cases selected for toxicology screening suggest subjective determinations for testing on the basis of local policy and individual coroner or medical examiner preference (10). More comprehensive toxicology testing for suicide victims might provide greater insight into trends and geographic variations in the role of substance use in suicides. Comprehensive toxicology data also could be linked with demographic data already collected by coroners and medical examiners at the state and local levels. These combined data could enable studies of the relationship of substance use to suicides in specific populations at greatest risk. Such studies remain critical to better understanding of suicidal behavior and development of effective interventions. References
* Alaska, Colorado, Georgia, Maryland, Massachusetts, New Jersey, North Carolina, Oklahoma, Oregon, Rhode Island, South Carolina, Virginia, and Wisconsin. † Alaska, 62 (41.1%) suicide victims tested; Colorado, 578 (88.0%); Georgia, 563 (62.2%); Maryland, 366 (75.9%); Massachusetts, 337 (78.7%); New Jersey, 554 (89.2%); North Carolina, 906 (87.0%); Oklahoma, 455 (88.3%); Oregon, 136 (25.9%); Rhode Island, 83 (96.5%); South Carolina, 286 (64.3%); Virginia, 812 (97.7%); and Wisconsin, 412 (69.9%).
Table 1
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to [email protected].Date last reviewed: 11/21/2006 |
|||||||||
|