|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
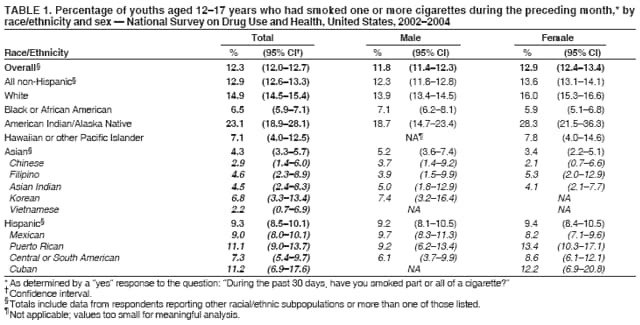
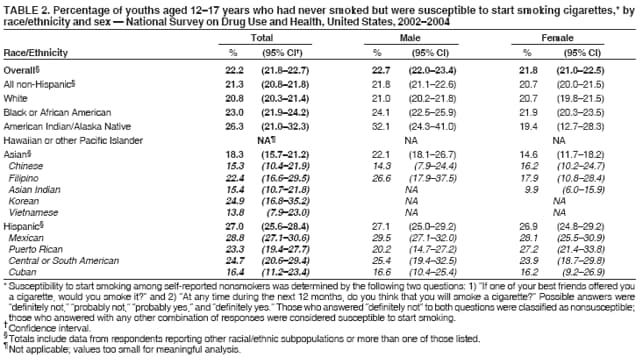
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail. Racial/Ethnic Differences Among Youths in Cigarette Smoking and Susceptibility to Start Smoking --- United States, 2002--2004Limited information on cigarette smoking in racial/ethnic subpopulations hinders development and implementation of targeted interventions for smoking prevention and cessation. Because of small sample sizes or inadequate study formats, cigarette smoking among youths has been studied mostly in major racial/ethnic populations (e.g., Asian or Hispanic) instead of subsets of these populations (e.g., Vietnamese or Cuban). Data on major population categories might mask differences in tobacco-use prevalence among subpopulations. To assess the prevalence of cigarette smoking among youths aged 12--17 years in six major racial/ethnic populations* and nine Asian or Hispanic subpopulations† in the United States, the Substance Abuse and Mental Health Services Administration and CDC analyzed self-reported data collected during 2002--2004 from the National Survey on Drug Use and Health (NSDUH). This report summarizes the results of that analysis, which indicated that the estimated prevalence of cigarette smoking in this age group ranged from 23.1% for American Indians/Alaska Natives (AI/ANs) to 2.2% for Vietnamese. Implementing tobacco-control programs that include culturally appropriate interventions might help reduce cigarette smoking in racial/ethnic subpopulations. NSDUH is an annual, in-person household survey that collects information on drug use and abuse from a nationally representative sample of the U.S. civilian, noninstitutionalized population aged >12 years. The average, weighted, overall response rate for the 2002--2004 surveys was 81% for youths aged 12--17 years, based on a household screening response rate of 91% and an interview response rate of 89%; the final sample size was 68,611. Racial/ethnic classifications by NSDUH were based on standards for classification of federal data (1). Prevalences and 95% confidence intervals (CIs) were calculated; data were weighted to account for different probabilities of selection within strata. Differences in prevalences were considered statistically significant if CIs did not overlap; no other test for statistical significance was performed. Current cigarette smoking was assessed by asking respondents aged 12--17 years, "During the past 30 days, have you smoked part or all of a cigarette?" Youths who answered "yes" were classified as current smokers. Susceptibility to start smoking among self-reported nonsmokers was determined by the following two questions: 1) "If one of your best friends offered you a cigarette, would you smoke it?" and 2) "At any time during the next 12 months, do you think that you will smoke a cigarette?" Possible answers were "definitely not," "probably not," "probably yes," and "definitely yes." Those who answered "definitely not" to both questions were classified as nonsusceptible; those who answered with any other combination of responses were considered susceptible to start smoking. Among youths, AI/ANs had the greatest cigarette smoking prevalence (23.1%), followed by non-Hispanic whites (14.9%), Hispanics (9.3%), non-Hispanic blacks (6.5%), and Asians (4.3%) (Table 1). Among Asian subpopulations, smoking prevalence ranged from 2.2% for Vietnamese to 6.8% for Koreans; among Hispanic populations, prevalence ranged from 7.3% for Central and South Americans to 11.2% for Cubans. However, none of the differences among Asian subpopulations and Hispanic subpopulations were statistically significant. No significant differences were observed between male and female youths in any of the major populations or subpopulations, except for non-Hispanic white youths, among whom females had a greater prevalence of cigarette smoking (16.0%) than males (13.4%). A wide range in susceptibility to start smoking was observed among youths who had never smoked (Table 2). Overall, 22.2% were susceptible to start smoking. Youths in the Mexican subpopulation were significantly more susceptible (28.8%) to start smoking than non-Hispanic white (20.8%), non-Hispanic black (23.0%), Cuban (16.4%), Asian Indian (15.4%), Chinese (15.3%), and Vietnamese (13.8%) youths. No significant differences in susceptibility to start smoking were observed between male and female youths in any of the major populations or subpopulations. Reported by: J Gfroerer, Office of Applied Studies, Substance Abuse and Mental Health Services Admin. R Caraballo, PhD, Office on Smoking and Health, National Center for Chronic Disease Prevention and Health Promotion, CDC. Editorial Note:The findings in this report indicate that cigarette smoking varied among racial/ethnic subpopulations in addition to major populations of youths aged 12--17 years and that AI/AN youths had the highest prevalence of cigarette smoking in the United States. Differences in smoking prevalence might be attributable to multiple factors, including cigarette prices and discount offers, exposure to antismoking campaigns, and ability to buy cigarettes, all of which can vary by racial/ethnic population (2). This study also suggests that, overall, approximately one in five nonsmokers aged 12--17 years is susceptible to start smoking. Among the six major populations and nine Asian or Hispanic subpopulations studied, Mexican youths who had never smoked appeared most susceptible to start smoking. Youths in this subpopulation might need specialized prevention interventions to lower their susceptibility. Two major public health objectives are 1) to prevent the initiation of cigarette smoking among children, adolescents, and young adults and 2) to help those who already smoke, including children and adolescents, to quit. The overall prevalence of cigarette smoking among high school students declined from 36.4% in 1997 to 23.0% in 2005 (3); however, recent evidence suggests that the reduction in smoking rates over time might have stalled (4). Children and teens constitute the majority of all new smokers (5). In 2003, cigarette companies spent approximately $15.2 billion to promote their products, nearly triple their spending in 1996 (6). Conversely, spending by state tobacco-control programs declined from $749.7 million in 2002 to $551.0 million in 2006, an amount still less than 3% of the $21.3 billion that the states received in 2005 from tobacco excise taxes and the 1998 Tobacco Master Settlement Agreement (7). The decline in spending on tobacco-control programs might have been a factor in slowing the progress made in reducing smoking among adolescents (3,8). The findings in this report are subject to at least four limitations. First, NSDUH surveys are conducted only in English or Spanish, which might have limited participation by some persons (e.g., Asians). Second, the precision of smoking prevalence estimates for certain racial/ethnic subpopulations is low, especially when reported by sex; therefore, differences in prevalence among these subpopulations might not have been detected, and estimates should be interpreted with caution. Third, the data in this report were self-reported in participant households and subject to social-desirability bias (2). However, to reduce this bias, the tobacco-use section in the NSDUH survey was administered using computer-assisted self-interviewing, in which participants read the questions on a computer screen or listened to them through headphones and then entered their responses into the computer. Finally, because of changes in the NSDUH survey methodology in 2002, comparison of the estimates in this report with pre-2002 NSDUH data is not recommended (9). Sustained, culturally appropriate interventions to prevent youths from starting to smoke or help them to quit might be effective in racial/ethnic populations and subpopulations with high prevalences of cigarette smoking. Effective tobacco-control initiatives might result from comprehensive behavior-based approaches enhanced by 1) using culturally targeted media and education campaigns (10) and 2) increasing the capacities (e.g., for program development) of specific populations to address tobacco use within their communities. To aid these populations in developing programs, systematic reviews of the effectiveness of interventions to reduce or prevent tobacco use are offered by the Guide to Community Preventive Services at http://www.thecommunityguide.org/tobacco. References
* Major racial/ethnic populations include: Hispanics and the following non-Hispanic populations: white, black or African American, American Indian/Alaska Native, Hawaiian or other Pacific Islander, and Asian. † Asian subpopulations: Chinese, Filipino, Asian Indian, Korean, and Vietnamese. Hispanic subpopulations: Mexican, Puerto Rican, Central or South American, and Cuban. Table 1
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to [email protected].Date last reviewed: 11/29/2006 |
|||||||||
|