|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
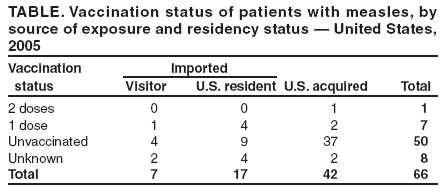
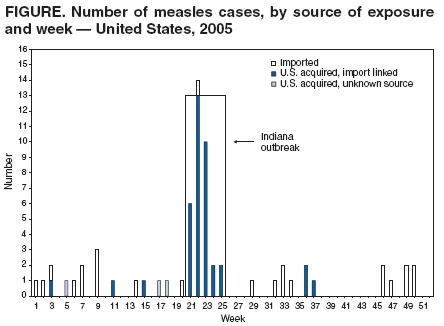
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail. Measles --- United States, 2005Measles is a highly infectious, acute viral illness that can be complicated by severe pneumonia, diarrhea, and encephalitis and can result in death. In the prevaccine era, approximately 500,000 cases of measles occurred annually in the United States (1). During 2005, local and state health departments reported to CDC 66 confirmed cases of measles (incidence rate: less than one case per 1 million population), 34 of which were from a single outbreak in Indiana associated with infection in a traveler returning to the United States. This report describes the epidemiology of U.S. measles cases in 2005 and documents the absence of endemic measles and the continued risk for imported measles infections that can result in transmission within the United States. The findings underscore the need to maintain the highest possible measles vaccination coverage in the United States and to adhere to recommendations regarding measles vaccination. Case ClassificationIn accordance with state laws and regulations, health-care providers, laboratories, and other health-care workers report measles cases to state and public health departments; this information is forwarded to CDC. Data on variables such as vaccination status, age, complications, transmission setting, and serologic confirmation of cases also are collected. In 2005, of the 66 cases reported, 44 (66%) were confirmed by laboratory testing, including 19 with detection of both IgM antibodies and virus (by polymerase chain reaction, culture, or both) and 25 with only measles IgM detected. The remaining 22 (33%) were confirmed by meeting the clinical case definition* and by being linked epidemiologically to a laboratory-confirmed case. Twenty-four (36%) of the 66 infections were imported,† including 17 (71%) in U.S. residents who acquired measles while traveling abroad and seven (29%) in non-U.S. residents who acquired the disease abroad and traveled to the United States. Measles was imported from 16 countries on four continents.§ Of the 24 patients with imported measles, eight (33%) were infectious during airline flights (i.e., rash onset occurred some time during the period 4 days before through 4 days after date of U.S. arrival). No secondary transmission was identified among flight crew members or passengers seated in the same row or the row in front of or behind the infectious person. The other 42 (64%) cases were U.S. acquired,¶ of which 38 (90%) were import linked and four (10%) had unknown sources of exposure. Thirty-three (87%) of the 38 import-linked cases were part of a single outbreak in Indiana, traced to exposure in Romania. Of the remaining five import-linked cases, two patients were linked to measles imported from Nigeria, and three were linked to only one other case. Overall, 62 (94%) of the 66 cases in 2005 were determined to be import associated (i.e., either imported or U.S. acquired but import linked). Age and Sex DistributionDistribution of the 66 measles patients by age group was as follows: seven (10.6%) measles patients were aged <1 year, four (6.1%) 1--4 years, 33 (50%) 5--19 years, seven (10.6%) 20--34 years, and 15 (22.7%) >35 years. Thirty-one (47%) patients were male, and 34 (52%) were female; the sex of one patient was not recorded. Geographic and Temporal DistributionThe 66 cases were reported from 16 states. Five states reported more than two cases: Indiana (33 cases), New York (seven cases, including six from New York City), California (four cases), and Texas and Ohio (three cases each). Cases were reported during 28 of the 52 reporting weeks (Figure). The longest period during which no cases were reported was 8 weeks, from week 38 through week 45. The median number of cases reported per week was one (range: zero to 14 cases). The maximum number of cases reported during a single week was 14 (week 22). Vaccination StatusOf the 66 persons with measles, one had been vaccinated with 2 doses of a measles-containing vaccine and seven (11%) with 1 dose; 50 (76%) were unvaccinated, and eight (12%) had unknown vaccination status (Table). Fifteen of the 17 U.S. residents who acquired infection while traveling abroad had been eligible for vaccination with 2 doses of measles-containing vaccine, according to recommendations from the Advisory Committee on Immunization Practices (ACIP) (4). However, four (27%) had been vaccinated with only 1 dose; eight (53%) had not been vaccinated (including three infants aged 11--12 months), and three (20%) had unknown vaccination status. Two of the 17 U.S. residents were ineligible because they were born before 1957 (one had not been vaccinated; the other had unknown vaccination status). Of the seven visitors (non-U.S. residents) with imported measles, one (14%) had been vaccinated with 1 dose; four (57%) had not been vaccinated (including one infant aged 8 months), and two (29%) had unknown vaccination status. Among the 42 U.S.-acquired cases, one patient had been vaccinated with 2 doses; two (5%) patients had been vaccinated with 1 dose, and 37 (88%) had not been vaccinated (including 29 [69%] persons aged 1--19 years). The vaccination status of two patients (5%) was not known. OutbreaksDuring 2005, three measles outbreaks (i.e., with three or more epidemiologically linked cases) were reported to CDC. These outbreaks affected three states and accounted for 40 (61%) of the 66 reported cases. An outbreak in Indiana with 34 cases (including one Illinois resident) resulted from an unvaccinated U.S. resident aged 17 years who returned home after acquiring measles infection in Romania. Of the 34 patients in this outbreak, 32 (94%) were eligible for vaccination. Of these, one patient aged 16 years had been vaccinated with 2 doses, a health-care worker aged 34 years had been vaccinated with only 1 dose, and 28 (88%) patients aged 1--19 years had not been vaccinated, primarily because their parents were concerned about potential adverse events associated with vaccination. Vaccination status for two patients, aged 43 and 45 years, was unknown. Two other patients were ineligible because of their ages: one was aged <12 months, and the other was born before 1957 and presumed immune to measles. Among the school-age patients (aged 5--19 years), 20 (71%) were schooled at home. Three persons were hospitalized during this outbreak, including the health-care worker, who was treated in the intensive care unit and recovered (5,6). A second outbreak was traced to a visitor aged 6 years from Nigeria, who was hospitalized in Ohio. Cases of measles in two U.S. residents, an unvaccinated health-care worker and an unvaccinated person aged 89 years, were linked to the hospital setting. A third outbreak involved three U.S residents, two adults and a child aged 20 months, who had traveled together to a family reunion in Mexico and might have been exposed during air travel before returning to Texas. The adults had been vaccinated; the child had not been vaccinated. Viral GenotypesFive genotypes of measles virus were identified in specimens from 19 patients representing 11 importations. Genotype D4 was identified in two travelers to France and Germany, two visitors from Romania and Yemen, and eight patients with U.S.-acquired measles linked to an imported case from Romania (the Indiana outbreak). Genotype B3 was identified in a refugee from Kenya and two of the three U.S. travelers to Mexico (7). Genotype D8 was identified in two U.S. residents returning from India. Genotypes D6 and D9 were isolated from a foreign visitor from Armenia and a child returning from Indonesia, respectively. Measles viruses in the four U.S.-acquired cases with unknown sources were not genotyped. Reported by: G Dayan, MD, S Redd, P Rota, PhD, J Rota, MPH, W Bellini, PhD, Viral Diseases Div, National Center for Immunization and Respiratory Diseases (proposed); P Gould, MD, EIS Officer, CDC. Editorial Note:The epidemiology of measles in 2005 supports previous conclusions that endemic transmission of measles has been eliminated in the United States (8,9). Measles incidence was low (less than one case per million population), measles cases were geographically isolated, and 95% of cases were linked to importations (i.e., internationally imported or U.S-acquired, import-linked cases). In addition, no predominant and recurring viral genotype was detected, and the measles genotypes detected, in most circumstances, had been circulating within the country of presumed exposure (10). Half of all the cases in 2005 are traceable to one unvaccinated U.S. resident, who was infected during a visit to Romania of less than 2 weeks. This outbreak was the largest documented in the United States since 1996. All but two of the 34 patients in this outbreak were unvaccinated. The outbreak occurred because measles was imported into a population of children whose parents had chosen not to vaccinate their children because of safety concerns, despite evidence that that measles-containing vaccine is safe and effective (4). A major epidemic was averted because of high vaccination levels and a low rate of vaccine failure in the surrounding community. The cost of containing this outbreak was estimated at $167,685 (5). This outbreak and other cases reported during 2005 likely could have been prevented had existing ACIP vaccination recommendations been followed (4). The index case traveler should have been vaccinated with 2 doses of measles-containing vaccine before departure; exposed school-age children and personnel working in health-care facilities also should have had the recommended 2 doses before exposure. The epidemiology of measles in 2005 highlights the need to maintain the highest possible measles vaccination coverage in the United States and to continue to address the concerns of those who choose not to be vaccinated or who choose not to vaccinate their children. Because 100% coverage in U.S. residents might never be achieved and because communities of unvaccinated persons continue to exist, accurate surveillance and rapid response to outbreaks are essential to preventing widespread transmission of imported measles. Moreover, providing assistance to other countries to control measles globally can limit the risk for imported measles in the United States. References
* Generalized maculopapular rash lasting >3 days with fever >101.0ºF (>38.3ºC) and one of the following: cough, coryza, or conjunctivitis (2). † Cases among persons who were exposed and infected outside the United States (3). § Asia, 13 cases: India and Saudi Arabia had two each; Armenia, Bangladesh, China, Indonesia, Pakistan, Thailand, and Yemen had one each; and two persons traveled to more than one country in Southeast Asia. Europe, six cases: Germany and Romania, two each; Belgium and France, one each. North America, three cases: Mexico, three. Africa, two cases: Kenya and Nigeria, one each. ¶ U.S.-acquired cases are those in persons infected in the United States. These cases are subclassified into four groups: import linked (i.e., epidemiologically linked to an imported case); imported virus (i.e., cases that cannot be linked epidemiologically to an imported case but for which viral genetic evidence indicates an imported measles genotype); endemic (i.e., cases for which epidemiologic or virologic evidence indicates a chain of measles virus transmission that is continuous for >12 months within the United States); and unknown source (i.e., all other cases acquired in the United States for which an epidemiologic or virologic link to importation or to endemic transmission within the United States cannot be established after a thorough investigation) (3).
Table
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to [email protected].Date last reviewed: 12/20/2006 |
|||||||||
|