|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
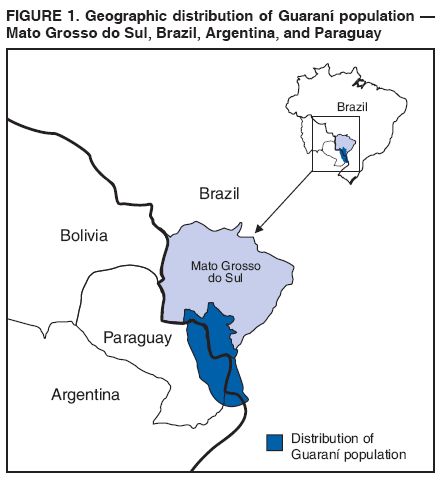
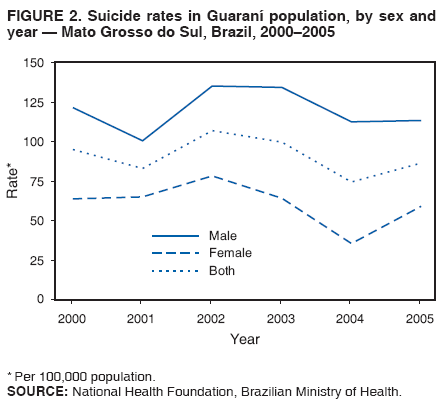
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail. Suicide Trends and Characteristics Among Persons in the Guaraní Kaiowá and Ñandeva Communities --- Mato Grosso do Sul, Brazil, 2000--2005Suicide rates among indigenous communities around the world vary substantially; in many nations these groups have the highest suicide risk of any identifiable cultural or ethnic group (1). Mato Grosso do Sul is a state in the southwest corner of Brazil that borders Bolivia and Paraguay. In 2004, the Guaraní, an indigenous ethnic group in the region (Figure 1), accounted for 2.6% of Mato Grosso do Sul's population (approximately 2,230,702).* During 1975--2000, the infant mortality rate decreased, and overall life expectancy increased in Mato Grosso do Sul; however, suicide increased as a proportion of overall mortality among the Kaiowá and Ñandeva communities of the Guaraní population (2). In 2000, the National Health Foundation (FUNASA) of the Brazilian Ministry of Health (BMH) initiated a study of suicide trends and characteristics in these two Guaraní communities; data were collected during 2000--2005, and epidemiologic assistance was provided by CDC. This report summarizes the results of that study, which suggested that the suicide rate among Guaraní was 19 times higher than the national rate in Brazil and 10 times higher than the rate in Mato Grosso do Sul and that suicides disproportionately affected Guaraní adolescents and young adults. To decrease suicide rates, BMH initiated research and prevention programs among the Guaraní, and the Guaraní initiated measures to increase their economic self-sufficiency. Participants in the study were from the Kaiowá and Ñandeva communities of the Guaraní population, collectively referred to as Guaraní in this report. FUNASA medical teams determined cause of death using categories from the International Classification of Diseases and Related Health Problems, Tenth Revision (ICD-10) (3). Suicide was defined as a death resulting from purposely self-inflicted poisoning or injury corresponding to ICD-10 codes X60--X84 and Y87. Demographic data on Guaraní were drawn from routinely updated census information such as name, sex, date of birth, ethnicity, address, village, Special Indigenous Sanitary District (DSEI), and municipality. As part of an ongoing ethnographic study, an anthropologist obtained qualitative information on each death through interviews with persons who included political and spiritual leaders of the communities. Participants were asked questions about the decedent (e.g., observations of decedent's behavior) and the community (e.g., social or environmental conditions that might have been associated with the suicide). Among the Guaraní in 2000, information on age was available for all but seven cases of suicide, and information on sex was available for all but one case. Demographic data for deaths in other years were complete. Crude rates and age- and sex-specific rates were calculated per 100,000 population. During 2000--2005, a total of 3,004 deaths were recorded in the Guaraní population in Mato Grasso do Sul, including 286 (9.5%) suicides; 190 (66.7%) of the suicide victims were male. All but three suicides were caused by suffocation (hanging); three were caused by pesticide ingestion. Annual suicide rates in the Guaraní ranged from 121.5 per 100,000 population for males in 2000 to 113.2 in 2005 and from 63.7 per 100,000 population for females in 2000 to 59.1 in 2005 (Figure 2). The ratio of male to female suicide rates was approximately 2 to 1. In 2005, the overall Guaraní suicide rate was 86.3 per 100,000 population. By comparison, in 2004, the most recent year for which national and state data were available, suicides represented 1.5% of deaths in Mato Grosso do Sul and 0.8% of deaths in Brazil (4). Therefore, the proportion of deaths caused by suicide in the Guaraní population during 2000--2005 was approximately six times the proportion in Mato Grosso do Sul and 12 times the proportion overall in Brazil in 2004. The suicide rate overall in Mato Grosso do Sul was 8.6 per 100,000 population, and the national rate was 4.5. The Guaraní suicide rate in 2005 was approximately 10 times the rate in Mato Grosso do Sul and 19 times the national rate in 2004. Persons aged <30 years accounted for 70% of the Guaraní population and 85% of the suicides. Among persons aged 20--29 years in 2005, the suicide rate was 159.9 per 100,000 population; among persons aged <20 years, suicide accounted for 28.0% of the deaths, and the suicide rate was 90.3 per 100,000 population. Reported by: C Coloma, MD, PhD, United Nations Educational, Scientific, and Cultural Organization, FUNASA, Ministry of Health; JS Hoffman, PhD, VP Gawryszewski, PhD, Disease Control Coordination, State Health Dept of São Paulo, Brazil. MD Bennett, PhD, AE Crosby, MD, Div of Violence Prevention, National Center for Injury Prevention and Control, CDC. Editorial Note:The findings in this report indicate that youths and young adults in Guaraní communities had higher suicide rates than older members of their population and that the Guaraní suicide rate overall was higher than the rates in Mato Grosso do Sul and Brazil overall. In the United States, suicide rates among some American Indian and Alaska Native (AI/AN) indigenous populations have been similar to those of the overall U.S. population, whereas in certain other AI/AN populations, rates have been seven times higher than the U.S. rate overall (5). Historically, the highest suicide rate nationally in Brazil has been among those aged >65 years (6). However, among the Guaraní, the highest rates were among adolescents and young adults. Among Guaraní aged 20--29 years, the 2005 suicide rate was 159.9 per 100,000 population, compared with 6.1 for the same age group nationwide in 2004 (4). Previous studies have identified multiple factors that might be associated with suicidal behaviors among the Guaraní. These factors, some resulting from colonization, include rapid sociocultural change, disturbances in traditional social life, progressive dismantling of extended family structure, and forced relocation to reservations (7). Exposure to different and conflicting cultures, perspectives, and belief systems exacerbates challenges faced by these communities and contributes to intergenerational conflict. Studies conducted among other indigenous communities indicate that youths often perceive themselves as marginalized from mainstream society and their own communities (7), resulting in a sense of social isolation that might contribute to an increased rate of suicide. The findings in this report are subject to at least four limitations. First, counting the number of suicides based on death certificates might underestimate the true number because of misclassification of cause of death (8). Many decedents were buried privately by their families; in 2000, 16.5% of deaths among the Guaraní occurred without medical attention or certification by a coroner or medical examiner, so the cause of death could not be established. In 2001, DSEI began providing financial support for burials, thereby increasing death registrations, and by 2003, cause of death could not be established for only 5.7% of deaths. Second, because data were not specifically collected at the municipal or national level, suicide rates of indigenous and nonindigenous populations could not be compared. Third, temporal data were limited and insufficient for comprehensive analysis. Finally, the small absolute number of suicides in the Guaraní limited the detail of this analysis. Suicide is a complex, multifaceted problem influenced by risk factors among persons, families, communities, and societies. Studies on indigenous populations in other nations have found that community-based, comprehensive suicide-prevention programs are the most promising (9). Such programs vary, but strategies typically include counseling, support groups, crisis response, recreational activities, volunteer support systems, and cultural-heritage education. For example, a suicide-prevention program for an American Indian community in the United States included a comprehensive strategy involving schools, community outreach to persons at risk for suicide and their families, improved infrastructure of local mental health services, and interventions addressing common suicide risk factors in the community (e.g., alcohol abuse, family violence, and unemployment) (10). To better address health disparities among indigenous communities, BMH established DSEI and placed multidisciplinary indigenous health-care teams in municipal governments. These teams periodically visit area villages and, with the support of trained local residents, provide health care. In 2000, FUNASA began a mental health initiative to address alcohol abuse and suicidal behaviors in indigenous ethnic communities. This initiative involved developing the Monitoring Center for Indigenous Mental Health, which includes physicians, behavioral scientists, social workers, and linguists. The center supports research and encourages a multidisciplinary approach to assessing and preventing suicidal behavior. Its projects are developed with community participation and designed so that they can be sustained by the local community. In addition, the Guaraní have been organizing to recover, through court challenges and legislation, most of their former territories; this is expected to increase their economic self-sufficiency and reduce poverty and unemployment, improvements associated with decreased risk for suicide and suicidal behaviors (9). References
* Instituto Brasileiro de Geografia e Estatística. Population estimates for Brazilian municipalities; 2004. Available at http://www.ibge.gov.br/english/estatistica/populacao/estimativa2004/default.shtm.
Figure 1
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to [email protected].Date last reviewed: 1/11/2007 |
|||||||||
|