|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
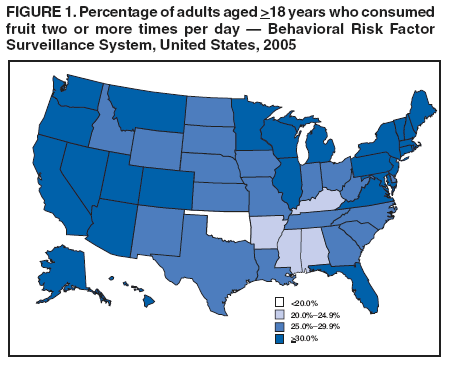
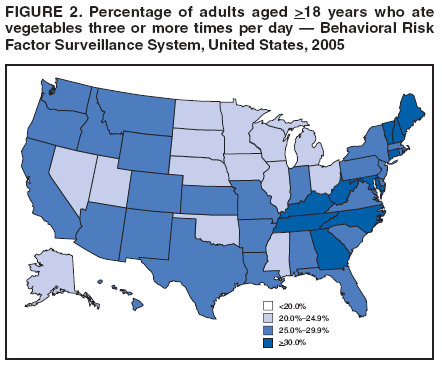
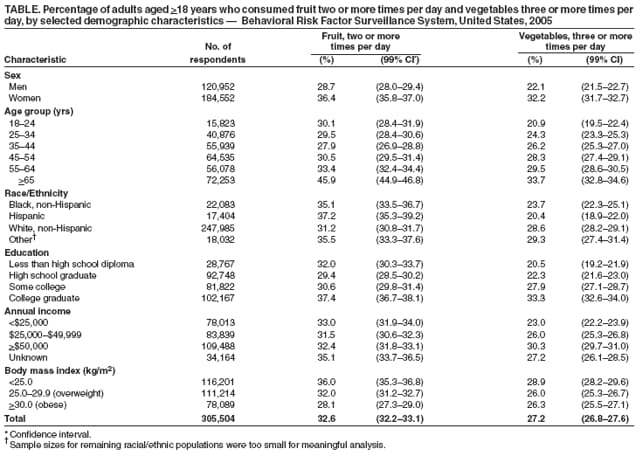
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail. Fruit and Vegetable Consumption Among Adults --- United States, 2005Please note: An erratum has been published for this article. To view the erratum, please click here. A diet high in fruits and vegetables is associated with decreased risk for chronic diseases (1). In addition, because fruits and vegetables have low energy density (i.e., few calories relative to volume), eating them as part of a reduced-calorie diet can be beneficial for weight management (2). Healthy People 2010 health objectives include increasing to 75% the percentage of persons aged >2 years who eat at least two daily servings* of fruit (objective 19-5) and increasing to 50% the proportion of persons aged >2 years who eat at least three daily servings of vegetables, with at least one third being dark green or orange vegetables (objective 19-6) (3). To assess the level of fruit and vegetable consumption among adults by state and demographic characteristics, data from the 2005 Behavioral Risk Factor Surveillance System (BRFSS) were analyzed. This report describes the results of that analysis, which indicated that 32.6% of adults consumed fruit two or more times per day and 27.2% ate vegetables three or more times per day. The results underscore the need for continued interventions that encourage greater fruit and vegetable consumption among U.S. adults. BRFSS is an ongoing, state-based, random-digit--dialed telephone survey of the noninstitutionalized, U.S. civilian population aged >18 years. BRFSS data are used to provide information regarding health behaviors that relate to the leading causes of death among U.S. adults and to monitor state progress toward health objectives. BRFSS data are weighted to the respondents' probabilities of being selected and to the age-, race/ethnicity-, and sex-specific populations from annually adjusted census reports in the state. In 2005, response rates† among the states ranged from 34.6% to 67.4% (median: 51.1%) when calculated by the guidelines of the Council of American Survey and Research Organizations. Cooperation rates§ ranged from 58.7% to 85.3% (median: 75.1%). City- and county-level 2005 data on health behaviors, including consumption of fruits and vegetables, for more than 153 cities are available as part of the BRFSS Selected Metropolitan/Micropolitan Area Risk Trends project.¶ The BRFSS module on fruits and vegetables included six questions that were preceded by the following statement: "These next questions are about the foods you usually eat or drink. Please tell me how often you eat or drink each one, for example, twice a week, three times a month, and so forth." The six questions were as follows: 1) "How often do you drink fruit juices such as orange, grapefruit, or tomato?" 2) "Not counting juice, how often do you eat fruit?" 3) "How often do you eat green salad?" 4) "How often do you eat potatoes, not including French fries, fried potatoes, or potato chips?" 5) "How often do you eat carrots?" 6) "Not counting carrots, potatoes, or salad, how many servings of vegetables do you usually eat? (Example: a serving of vegetables at both lunch and dinner would be two servings.)" Participants were not given a definition of serving size. Total daily fruit consumption was calculated based on responses to questions 1 and 2, and total daily vegetable consumption was based on responses to questions 3--6. The percentage of adults who consumed fruit two or more times per day and vegetables three or more times per day was calculated for the overall population and by selected characteristics. To calculate consumption in times per day, weekly frequencies were divided by seven, monthly frequencies were divided by 30, and yearly frequencies were divided by 365. To be consistent with past analyses, the answer to question 6 was treated as times per day. Data from all 50 states and the District of Columbia (DC) were included. A total of 347,278 persons completed the interview. After excluding persons who did not report selected demographic or behavioral risk-factor information (n = 38,317), persons who did not answer all six questions in the fruit and vegetable module (n = 14,179), and persons who reported consumption of fruits and vegetables >25 times per day (an unlikely frequency of consumption) (n = 61), 305,504 persons were included in the final sample. In 2005, approximately 32.6% of the U.S. adult population surveyed consumed fruit two or more times per day, and 27.2% ate vegetables three or more times per day. The prevalence of consuming fruit two or more times per day was 28.7% among women and 36.4% among men. By age, prevalence of consuming fruit two or more times per day ranged from 27.9% among persons aged 35--44 years to 45.9% among persons aged >65 years. Among racial/ethnic populations, Hispanics had the highest prevalence (37.2%) of consuming fruit two or more times per day, and non-Hispanic whites had the lowest prevalence (31.2%). College graduates had the highest level of fruit consumption (37.4%) compared with lower levels of education, as did persons who earned >$50,000 per year (32.4%) compared with those who earned less. Persons who were not overweight or obese (i.e., body mass index [BMI] <25) had the highest prevalence of consuming fruit two or more times per day (36.0%), and obese persons (BMI >30) had the lowest prevalence (28.1%) (Table). The prevalence of eating vegetables three or more times per day was 22.1% among men and 32.2% among women and ranged from 20.9% among persons aged 18--24 years to 33.7% among persons aged >65 years. Among racial/ethnic populations, whites had the highest prevalence (28.6%) of eating vegetables three or more times per day, and Hispanics had the lowest prevalence (20.4%). College graduates had the highest level of vegetable consumption (33.3%) compared with lower education levels, as did persons earning >$50,000 per year (30.3%) compared with those earning less. Persons who were not overweight or obese had the highest prevalence of eating vegetables three or more times per day (28.9%), and overweight persons had the lowest prevalence (26.0%). Twenty-six states reported that >30% of the adults consumed fruit two or more times per day (Figure 1), and 10 states reported that >30% of adults ate vegetables three or more times per day (Figure 2). By state, the prevalence of eating fruit two or more times per day ranged from 19.2% to 37.8%, and the prevalence of eating vegetables three or more times per day ranged from 20.9% to 39.0%. No state reached the Healthy People 2010 national objectives for fruit and vegetable consumption. Reported by: HM Blanck, PhD, DA Galuska, PhD, C Gillespie, MS, L Kettel Khan, PhD, MK Serdula, MD, MK Solera, MS, Div of Nutrition and Physical Activity; AH Mokdad, PhD, Div of Adult and Community Health, National Center for Chronic Disease Prevention and Health Promotion; LP Cohen, MD, EIS Officer, CDC. Editorial Note:The findings in this report indicate that adults in the 50 states and DC have not achieved national objectives for fruit and vegetable consumption. A separate midcourse review of Healthy People 2010 determined that data were not yet available to update estimates toward meeting fruit and vegetable consumption goals; however, existing data were used to make interim analyses, which indicated that the average fruit intake among persons aged >2 years remained the same from 1994--1996 to 1999--2002 (1.6 servings) and that average vegetable consumption declined from 3.4 to 3.2 servings during the same period, with no noted change in the daily consumption of dark green or orange vegetables (0.3 servings).** To meet the 2010 national objectives, a more sustained and effective public health response is needed, including continued surveillance, identification of barriers to eating more fruits and vegetables, and environmental changes (e.g., increasing the proportion of fruits and vegetables in vending machines and promoting healthful food advertising and the availability of healthful foods). Interventions that increase fruit and vegetable consumption by changing behaviors should be promoted, as should those that increase public awareness of the overall benefits of fruits and vegetables in the diet (4). The 2005 U.S. Dietary Guidelines suggest eating more fruits and vegetables than have been recommended in the past (1). The most recently recommended numbers of daily servings of fruits and vegetables are related to sex, age, and physical activity level; for adults, recommended levels are three to five servings of fruit and four to eight servings of vegetables per day†† (1). In 1991, Produce for Better Health (a nonprofit organization that promotes the consumption of fruits and vegetables) and the National Cancer Institute initiated the 5 A Day for Better Health program to promote healthy eating through fruit and vegetable consumption. In 2005, CDC became the lead federal agency for the program, which is a partnership of government, nonprofit, business, and community organizations. The program has encouraged behaviors that increase fruit and vegetable intake (5). In addition to the 5 A Day for Better Health program, CDC's Steps to a HealthierUS Cooperative Agreement Program and the Nutrition and Physical Activity Program to Prevent Obesity and Other Chronic Diseases support various state and local programs that have effectively increased fruit and vegetable consumption. These programs include school-based interventions such as the Fresh Fruit and Vegetable Program; during an evaluation of this program, parents reported that their children were requesting more fruits and vegetables at home, and many children described positive changes in their eating habits and a greater willingness to try fruits and vegetables (6). A healthy-eating program for preschoolers, Color Me Healthy, resulted in 79% of child-care providers reporting that children were more willing to try new foods, and 82% reporting that the program had improved fruit and vegetable recognition (7). Participants in Body & Soul, a health program for churches serving the black community, had greater fruit and vegetable intake when compared with controls (8).§§ CDC programs also support state initiatives that provide nutritional education and increase access to fruits and vegetables through community gardens, farmers' markets, and restaurants (5). The findings in this report are subject to at least five limitations. First, although the retest consistency of participant responses has been validated in multiple populations, estimates of fruit and vegetable intake from abbreviated food questionnaires such as the BRFSS fruit and vegetable module are lower than other methods of dietary assessment (9,10). Second, BRFSS does not include persons without landline telephones or those residing in institutions, so the results might not be representative of certain U.S. populations. Third, the BRFSS survey has low response rates, which might result in an overestimation or underestimation of fruit and vegetable consumption. Fourth, BMI data are based on self-reported measures, which might lead to an underestimation of BMI. Finally, this analysis reports fruit and vegetable consumption according to number of times per day the foods were eaten, whereas Healthy People 2010 objectives are based on number of servings per day. This difference in intake measurement might lead to misclassification of participants, resulting in an overestimation or underestimation of persons meeting national fruit and vegetable consumption objectives. The lack of success in meeting national goals for fruit and vegetable consumption indicates a need for additional measures to educate and motivate persons to make healthier dietary choices. Nutritional interventions should go beyond increasing individual awareness and target the family, local community, and overall society to eliminate barriers to healthy eating, provide support for persons who are making healthy changes, increase resources for populations with greater need, and emphasize nutritional policies that have an impact on society. Acknowledgment The findings in this report are based, in part, on data provided by BRFSS state coordinators.
References
* Information regarding recommended serving sizes based on U.S. Dietary Guidelines for Americans is available at http://www.health.gov/dietaryguidelines/dga2005/document/html/appendixa.htm. † The percentage of persons who completed interviews among all eligible persons, including those who were not successfully contacted. Rates available at http://www.cdc.gov/brfss/technical_infodata/2005qualityreport.htm. § The percentage of persons who completed interviews among all eligible persons who were contacted. ¶ Additional information available at http://www.cdc.gov/brfss/smart. ** US Department of Health and Human Services. Healthy People 2010 midcourse review. Available at http://www.healthypeople.gov/data/midcourse/default.htm. †† Additional information regarding recommendations, which vary based on caloric level of the diet, are available at http://www.health.gov/dietaryguidelines/dga2005/document/html/chapter5.htm. §§ Additional information regarding these programs is available at the following websites: 5 A Day: http://www.5aday.gov, Steps to a HealthierUS Cooperative Agreement Program: http://www.cdc.gov/steps, the Nutrition and Physical Activity Program to Prevent Obesity and Other Chronic Diseases: http://www.cdc.gov/nccdphp/dnpa/obesity/state_programs/index.htm, Color Me Healthy: http://www.colormehealthy.com, and Body & Soul: http://www.bodyandsoul.nih.gov.
Figure 1
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to [email protected].Date last reviewed: 3/15/2007 |
|||||||||
|