|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
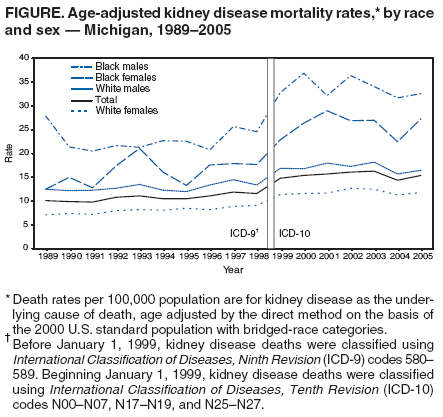
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail. Kidney Disease Mortality --- Michigan, 1989--2005Kidney disease was the ninth leading cause of death in Michigan in 2005 (1) and in the United States in 2004 (2). In 2004, the incidence rate for kidney failure (i.e., end-stage renal disease) was higher in Michigan than in the United States (365 versus 353 per 1 million population) (3). A total of 3,695 Michigan residents started treatment (i.e., dialysis or transplant) for kidney failure in 2004; by the end of that year, 11,002 Michigan residents were receiving dialysis, and 614 had received a transplant (3). Many of these persons had a diagnosis of diabetes (40%) or hypertension (30%) as the primary cause of kidney failure (3). To examine recent trends in kidney disease mortality, the Michigan Department of Community Health (MDCH) analyzed vital statistics data from the period 1989--2005. This report describes the results of that analysis, which indicated that kidney disease mortality is a growing public health problem in Michigan and that blacks were more likely than whites to die from kidney disease. Continued disease-prevention and health-promotion activities, including targeted interventions among populations at greatest risk, are needed by MDCH and other organizations to reduce the burden of kidney disease in Michigan. Vital statistics data from the period 1989--2005 were analyzed to determine the number of deaths in Michigan with kidney disease as the underlying cause. For 1999--2005, kidney disease deaths were classified using International Classification of Diseases, Tenth Revision (ICD-10) codes N00--N07, N17--N19, and N25--N27. For 1989--1998, kidney disease deaths were classified using International Classification of Diseases, Ninth Revision codes 580--589. Kidney disease mortality rates were calculated by selected demographic variables (i.e., age, sex, and race) using annual U.S. Census population estimates for Michigan for 1989--2005 and were age adjusted by the direct method on the basis of the 2000 U.S. standard population with bridged-race categories (4). Standard methodology assuming a Poisson distribution was used to estimate 95% confidence intervals (CIs) (5). From 1989 to 1998, kidney disease mortality rates increased by 14.9%, from 10.1 (CI = 9.4--10.8) per 100,000 population to 11.6 (CI = 10.9--12.3) (Figure). After implementation of ICD-10 coding in 1999, kidney disease mortality rates increased by 4.1%, from 14.8 (CI = 14.0--15.6) in 1999 to 15.4 (CI = 14.7--16.1) in 2005. The kidney disease mortality rate was significantly higher among persons aged >75 years than among younger age groups. In 2005, age-specific mortality rates were 173.6 (CI = 163.5--183.7) per 100,000 population for persons aged >75 years, compared with 19.0 (CI = 17.2--20.8) for those aged 50--74 years and 1.1 (CI = 0.9--1.3) for those aged <50 years. During 1989--2005, the age-adjusted kidney disease mortality rate in Michigan was consistently higher among black males and females than among white males and females (Figure). In 2005, the age-adjusted death rate among males was approximately 2.0 times higher among blacks than whites (32.6 [CI = 27.1--38.1] per 100,000 population versus 16.5 [CI = 15.2--17.8]). Among females, the age-adjusted rate was 2.3 times higher among blacks than whites (27.3 [CI = 23.3--31.3] versus 11.8 [CI = 10.9--12.7]). Reported by: A Andrews, MPH, National Kidney Foundation of Michigan, Ann Arbor; DK El Reda, DrPH, Div of Genomics, Perinatal Health, and Chronic Disease Epidemiology; G Radford, MA, Div for Vital Records and Health Statistics, Michigan Dept of Community Health. NR Burrows, MPH, K Ernst, Div of Diabetes Translation, National Center for Chronic Disease Prevention and Health Promotion, CDC. Editorial Note:Kidney disease mortality is a growing public health problem in Michigan. The findings in this report indicate that kidney disease mortality rates increased during 1989--2005 and that blacks were more likely than whites to die from kidney disease. The increased kidney disease mortality rate might be explained, in part, by the increasing prevalence of kidney failure in Michigan (6). The prevalence of diabetes and hypertension, two risk factors for kidney failure, also has increased among adults in Michigan, and self-reported diabetes and hypertension are more prevalent among blacks than whites (7). The results described in this report identify population groups in Michigan that need targeted interventions to reduce the prevalence of kidney disease risk factors and ultimately reduce morbidity and mortality from kidney disease. The findings in this report are subject to at least three limitations. First, the change in ICD classification in 1999 resulted in a new coding structure that classified more deaths with kidney disease as the underlying cause of death (8). During 1998--1999, an apparent increase occurred in age-adjusted kidney disease mortality rates; part of this increase likely can be attributed to changes in ICD coding. Second, mortality rates were estimated using only kidney disease as the underlying cause of death (i.e., not including deaths with kidney disease listed as a contributing cause), which underestimates the overall burden of mortality associated with kidney disease. Finally, kidney disease mortality among Hispanics was not analyzed; however, less than 4% of the population in Michigan in 2005 was Hispanic (9). The number of persons living with chronic kidney disease (CKD) in Michigan is expected to increase with the increasing prevalence of diabetes and hypertension, major risk factors for kidney disease (7). In 2002, MDCH and the National Kidney Foundation of Michigan (NKFM) developed a plan for key health-care and community interventions to promote early identification and appropriate management of Michigan residents with CKD. Interventions in health-care settings include educating physicians regarding CKD management, developing a common CKD guideline for health plans across Michigan, and implementing mandatory reporting of the estimated glomerular filtration rate (GFR) by laboratories.* Estimated GFR (eGFR) is calculated using serum creatinine levels and is accepted as the best overall measure of kidney function (10). Substantial kidney dysfunction can be present despite a normal serum creatinine level, and an estimate of GFR detects more cases of CKD than does the serum creatinine level alone (10). In 2002, guidelines for the diagnosis and management of CKD were established to provide a definition and a classification scheme for staging kidney disease patients according to levels of GFR (10). In 2006, legislation was passed in Michigan mandating eGFR reporting by laboratories when an outpatient serum creatinine test is performed for adults covered by Medicaid, alerting health-care providers of early loss of kidney function and prompting action to reduce disease progression. Five other states have mandated eGFR reporting (Connecticut, Louisiana, New Jersey, Pennsylvania, and Tennessee), and eGFR legislation has been proposed in four more states (Alabama, Mississippi, North Carolina, and South Carolina). Because blacks in Michigan are affected disproportionately by kidney disease, interventions have focused on reaching blacks in community-based settings, such as beauty salons, barber shops, schools, preschools, and Head Start programs. These interventions include lay health education programs about kidney disease and its risk factors. In one program, Healthy Hair Starts with a Healthy Body™, 20,433 beauty salon clients have received educational materials since 1999; 47% have reported taking a prevention step related to diet or exercise (e.g., limiting salt intake or increasing number of days they exercise >30 minutes), and 38% have visited a doctor or planned to do so. In another program, Dodge the Punch: Live Right™, 2,853 barber shop clients have received educational materials since 2005, and 37% have tried to eat more fruits and vegetables. In addition, MDCH and NKFM are working with CDC grantees at the University of Michigan and John Hopkins University to develop and test a national surveillance system for kidney disease in the United States. References
* Mandate covers patients on Medicaid only. However, a survey of Michigan laboratories conducted by the MDCH Bureau of Laboratories in August 2006 indicated that 67% of laboratories are routinely providing estimated GFR results, compared with 22% in 2004.
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to [email protected].Date last reviewed: 3/15/2007 |
|||||||||
|