|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
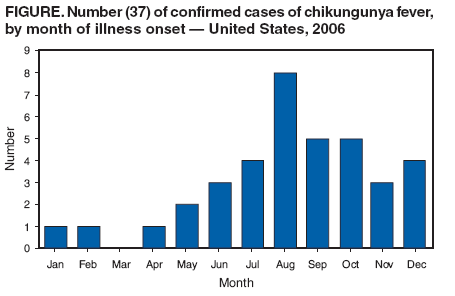
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail. Update: Chikungunya Fever Diagnosed Among International Travelers --- United States, 2006Chikungunya virus (CHIKV) is a mosquitoborne alphavirus indigenous to tropical Africa and Asia, where it causes endemic and epidemic chikungunya (CHIK) fever, an acute illness characterized by fever, arthralgias, and sometimes arthritis, commonly accompanied by conjunctivitis and rash. Although symptoms of CHIKV infection usually last days to weeks, joint symptoms and signs usually last for months and occasionally for 1 year or longer; deaths from CHIKV infection are rare (1). No specific antiviral treatment exists for CHIKV infection; treatment consists of supportive care, including analgesics and anti-inflammatory medication for joint symptoms. During 2005--2006, an epidemic of CHIK fever occurred on islands in the Indian Ocean and in India, resulting in millions of clinically suspected cases, mainly in southern India (2,3). In the United States, CHIK fever has been diagnosed in travelers from abroad. CDC previously reported 12 imported cases of CHIK fever diagnosed in the United States from 2005 through late September 2006, including 11 with illness onset in 2006 (4). This report of 26 additional imported cases with onset in 2006 underscores the importance of recognizing such cases among travelers. Health-care providers are encouraged to suspect CHIKV infection in travelers with fever and arthralgias who have recently returned from areas with CHIKV transmission. Acute- and convalescent-phase serum specimens can be submitted to CDC for testing through state health departments. Public health officials and health-care providers are encouraged to be vigilant for the possibility of indigenous CHIKV transmission in areas of the United States where CHIKV mosquito vectors are prevalent. Surveillance for CHIK fever in the United States is passive and laboratory based; the disease is not nationally reportable. In the United States in 2006, diagnostic testing for CHIKV was available at CDC by arrangement through state health departments. Although clinicians were encouraged to submit paired acute- and convalescent-phase serum specimens (ideally separated by 2 weeks), paired specimens were not uniformly available. All serum samples were tested by immunoglobulin M (IgM)-capture enzyme-linked immunosorbent assay (ELISA) and plaque-reduction neutralization (PRNT). IgM-negative acute-phase samples were tested by virus culture. Positive cultures were confirmed by polymerase chain reaction. Including the previously reported cases (4), CDC confirmed a total of 37 cases of CHIK fever with both positive IgM and PRNT and/or CHIKV isolation among U.S. travelers with onset in 2006; CHIKV was isolated from the blood of five of these patients. Patients were from 17 states (four southern states, four northeastern states, five midwestern states, and four western states) and the District of Columbia. Median age of patients was 49 years (range: 22--78 years), and 54% were female. In 25 (68%) of the 37 cases, onset occurred during June--October 2006 (Figure). The country most commonly visited before traveling to the United States was India, reported by 32 (86%) of the 37 patients; three patients reported visiting Sri Lanka, and one each had visited Zimbabwe and the Indian Ocean island of Réunion. An additional seven travelers returning to the United States in 2006 tested positive for CHIKV antibody by either IgM ELISA or PRNT but not by both. Reported by: Div of Vector-Borne Infectious Diseases, National Center for Zoonotic, Vector-Borne, and Enteric Diseases; Div Global Migration and Quarantine, National Center for Preparedness, Detection, and Control of Infectious Diseases; E Farnon, EIS Officer, CDC. Editorial Note:The 37 imported cases of CHIK fever in 2006 were unprecedented in the United States; during the preceding 15-year period, 1991--2005, only seven patients had both IgM and PRNT antibody to CHIKV detected by tests at CDC, and only three of these were known to be returning U.S. travelers (CDC, unpublished data, 2006). Factors contributing to the increase in the number of confirmed cases likely include an increase in the absolute number of infected travelers and the effects of recent CHIK fever publicity on the frequency of clinical diagnosis and submission of samples for laboratory testing (4). The five patients with positive cultures for CHIKV in 2006 likely represent a small fraction of CHIKV-viremic travelers who entered the United States, including many with subclinical or milder clinical CHIKV infections that were never documented. Human CHIKV infections typically include transient viremia of sufficient concentration to infect feeding vector mosquitoes (1), and approximately one fourth of human CHIKV infections are subclinical (5). Thus, despite the apparent absence of indigenous transmission of CHIKV in the United States or elsewhere in the western hemisphere, the risk for introduction into local vector mosquito populations in 2006 was likely higher than previously observed. In 2007, the risk likely will continue to be higher than usual, especially in tropical and subtropical areas where Aedes aegypti and Aedes albopictus mosquitoes, the main vectors of CHIKV (6), are seasonally abundant. Travelers to tropical areas of Asia and Africa should educate themselves regarding CHIK fever and follow CDC recommendations to prevent mosquito bites.* Febrile illness in persons traveling to the United States from Asia and Africa should be reported promptly to local or state public health authorities, and tests for CHIKV infection should be requested (4). Persons with febrile illness suspected to be caused by CHIKV should avoid mosquito exposure for at least 7 days after illness onset to reduce the likelihood of transmitting CHIKV to local mosquitoes, which might then transmit the virus to other humans. References
* Available at http://www.cdc.gov/ncidod/dvbid/chikungunya and http://www.cdc.gov/travel/other/2006/chikungunya_india.htm.
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to [email protected].Date last reviewed: 3/28/2007 |
|||||||||
|