|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
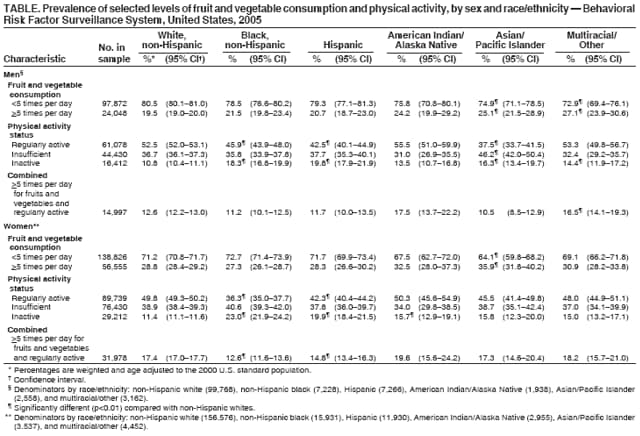
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail. Prevalence of Fruit and Vegetable Consumption and Physical Activity by Race/Ethnicity --- United States, 2005Diets high in fruits and vegetables and participation in regular physical activity are associated with a lower risk for several chronic diseases and conditions (1). The National Cholesterol Education Program and the American Cancer Society both emphasize lifestyle modifications that include diet and physical activity to reduce disease risk.* These are also two of the strategies implemented by states participating in CDC's Nutrition and Physical Activity Program to Prevent Obesity and Other Chronic Diseases. To examine the combined prevalence of 1) consumption of fruits and vegetables five or more times per day and 2) regular physical activity among U.S. adults by race/ethnicity, CDC analyzed self-reported data from the 2005 Behavioral Risk Factor Surveillance System (BRFSS). This report describes the results of that analysis, which indicated that the combined prevalence of these two behavioral strategies was higher among men of multiple/other races (16.5%) compared with non-Hispanic white men (12.6%). In addition, only 12.6% of non-Hispanic black women and 14.8% of Hispanic women, compared with 17.4% of non-Hispanic white women, engaged in these two behavioral strategies. These results underscore the need to promote diets high in fruits and vegetables and regular physical activity among all populations in the United States and among racial and ethnic minority communities in particular. BRFSS is a state-based, random-digit--dialed telephone survey of the noninstitutionalized U.S. civilian population aged >18 years. In 2005, the survey, which used a stratified, multistage probability sampling design, was administered to a nationally representative sample of adults from the 50 states and the District of Columbia, Puerto Rico, and the U.S. Virgin Islands (N = 356,112). The median state response rate† was 51.1%, and the median cooperation rate§ was 75.1%, when calculated using Council of American Survey and Research Organizations guidelines.¶ Data were weighted to the respondents' probabilities of being selected and to the age-, race-, and sex-specific populations from the states' annually adjusted census results to provide national estimates for the combined prevalence of the two behavioral strategies. Respondents were asked to report their race and ethnicity; six categories are included in this report: non-Hispanic white, non-Hispanic black, Hispanic, American Indian/Alaska Native (AI/AN), Asian/Pacific Islander (A/PI), and multiracial/other. Any respondent who reported being of Hispanic ethnicity was categorized as Hispanic regardless of race. After excluding 1) respondents who were from Puerto Rico or the U.S. Virgin Islands (n = 6,211), 2) respondents for whom information on race or ethnicity was missing or who replied "don't know" regarding race or ethnicity (n = 3,349), and 3) respondents who were missing information on physical activity (n = 24,136) or consumption of fruits and vegetables (n = 5,115), a total of 317,301 participants remained to constitute the final study sample. To measure consumption of fruits and vegetables, respondents were asked, "How often do you drink fruit juices such as orange, grapefruit, or tomato?" "Not counting juice, how often do you eat fruit?" "How often do you eat green salad?" "How often do you eat potatoes, not including French fries, fried potatoes, or potato chips?" "How often do you eat carrots?" and "Not counting carrots, potatoes, or salad, how many servings of vegetables do you usually eat?" After the responses were summarized, respondents were classified as eating or not eating fruits and vegetables five or more times per day. To measure physical activity, respondents were asked how often they engaged in physical activities of moderate intensity (i.e., brisk walking, bicycling, vacuuming, gardening, or anything else that causes small increases in breathing or heart rate) and vigorous intensity (i.e., running, aerobics, heavy yard work, or anything else that causes large increases in breathing or heart rate) for at least 10 minutes at a time in a usual week. Respondents were classified as being regularly active if they reported engaging in moderate-intensity activity at least 30 minutes per day, 5 or more days per week, or vigorous-intensity activity at least 20 minutes per day, 3 or more days per week. Respondents were classified as insufficiently active if they reported engaging in physical activity for at least 10 minutes per week, but did not meet the requirements for regular activity. Respondents who reported no instances of physical activity of >10 minutes' duration during a usual week were classified as inactive. A combined variable was created to classify 1) respondents who ate fruits and vegetables five or more times per day and were regularly active and 2) respondents who did not engage in either behavior. Age-adjusted prevalence was stratified by sex and racial/ethnic population. The chi-square test was used to compare non-Hispanic whites with all other racial/ethnic populations. Because of the multiple comparisons, the Bonferroni correction was used to detect statistically significant differences (p<0.01). During 2005, the estimated prevalence of eating fruits and vegetables five or more times per day was lower for men than women (Table). Compared with non-Hispanic white men (19.5%), the prevalence of eating fruits and vegetables five or more times per day was significantly higher among A/PI men (25.1%) and men of multiple/other races (27.1%). Compared with non-Hispanic white women (28.8%), the prevalence of eating fruits and vegetables five or more times per day was significantly higher among A/PI women (35.9%). Among men, engaging in regular physical activity was significantly less common for non-Hispanic blacks (45.9%), Hispanics (42.5%), and A/PIs (37.5%) than for non-Hispanic whites (52.5%). Among women, regular physical activity was significantly lower among non-Hispanic blacks (36.3%) and Hispanics (42.3%) than among non-Hispanic whites (49.8%). Compared with non-Hispanic white men (12.6%), the combined prevalence for eating fruits and vegetables five or more times per day and engaging in regular physical activity was significantly higher for men of multiple/other races (16.5%). Among women, the combined prevalence of eating fruits and vegetables five or more times per day and engaging in regular physical activity was significantly lower for non-Hispanic blacks (12.6%) and Hispanics (14.8%) than for non-Hispanic whites (17.4%). Reported by: J Kruger, MM Yore, M Solera, R Moeti, Div of Nutrition and Physical Activity, National Center for Chronic Disease Prevention and Health Promotion, CDC. Editorial Note:This report describes racial/ethnic differences in the combined prevalence of engaging in two behavioral strategies for reducing the risk for chronic disease: consuming fruits and vegetables five or more times per day and engaging in regular physical activity. The findings indicate that 14.6% of U.S. adults surveyed engage in both of these behavioral strategies. A previously published report examined the combined prevalence of these two behaviors among black and Hispanic survey populations in the United States, the state of Michigan, and the Racial and Ethnic Approaches to Community Health (REACH) 2010 program communities in Detroit, Michigan, during 2001--2003; the results indicated that 7%--11% of respondents consumed five or more daily servings of fruits and vegetables and were regularly active (2). Although this finding applies to black and Hispanic populations alone and is not directly comparable with the data described in this report, both reports indicate that few adults combine consuming fruits and vegetables frequently and engaging in regular physical activity, thus missing an opportunity to help reduce their risk for chronic disease. The findings in this report indicate racial/ethnic differences in combining these two behavioral strategies. Men of multiple/other races had a significantly higher prevalence of combining the two strategies than did non-Hispanic whites. In addition, compared with non-Hispanic white women, non-Hispanic black women and Hispanic women had significantly lower prevalences of combining the two strategies. In part, these differences among women are attributed to the lower prevalence of physical activity among non-Hispanic blacks and Hispanics, a finding that is consistent with previous reports (3). This difference might be attributed to lack of access; previous studies have demonstrated that lower-income, nonwhite communities often lack facilities for physical activity and environments that are supportive of physical activity (4). Despite the specific racial/ethnic differences observed in this report, the prevalence of engaging in both behaviors is low among all racial/ethnic populations. Thus, all populations should be targeted by interventions to increase consumption of fruits and vegetables and to increase regular physical activity. However, interventions are likely to be most effective if they are tailored to the needs of specific populations (e.g., Hispanics and non-Hispanic blacks) through strategies such as establishing programs in culturally relevant settings, promoting culturally appropriate foods and activities, and engaging members of the groups in development of interventions (5). Interventions to promote the two behavioral strategies described in this report might be accomplished simultaneously or individually. Interventions should be comprehensive, combining both consumer education and environmental factors, such as the availability of fresh fruits and vegetables and access to these foods (6). New approaches, such as improving availability by developing alternative sources for fruits and vegetables (e.g., food cooperatives, farmers' markets, and community gardens) and providing alternative transportation options (e.g., car pools and ride-sharing programs) should be considered. The Community Guide to Preventive Services has identified nine evidence-based strategies to increase physical activity at the community level, including increasing access combined with informational approaches, interventions providing behavioral and social support, and environmental and policy approaches (7). The findings in this report are subject to at least three limitations. First, prevalence estimates are based on self-reports and therefore are subject to reporting errors. Estimates of the intake of fruits and vegetables from short food-frequency questionnaires, such as the BRFSS module on fruits and vegetables, are lower than those made from other more extensive methods of dietary assessment used in research settings (8). Although the BRFSS fruit and vegetable module has been determined to have moderate validity and reliability in multiple population groups, its reliability has been determined to be lowest among AI/AN populations, and validity studies have not been conducted among AI/AN or A/PI populations (9). Similar questions on physical activity have been found to be reliable (10) but have not been validated by studies among subpopulations. Second, the BRFSS sample does not include persons who are institutionalized or who do not have landline telephones. To the extent that these groups have different behavioral patterns, the estimates of prevalence might be biased. Finally, because of the low response rate (51.1%) and because respondents from Puerto Rico and the U.S. Virgin Islands were excluded, results might not be representative of the U.S. population. Increasing consumption of fruits and vegetables and levels of physical activity are two key strategies implemented by states in CDC's Nutrition and Physical Activity Program to Prevent Obesity and Other Chronic Diseases.** In these states, interventions to address these behaviors are implemented at individual, group, and community levels and include education, access to fruits and vegetables, and opportunities for physical activity in settings such as day care centers, work sites, and communities. State coordinators work with statewide coalitions and community partners to develop statewide action plans and interventions to promote fruit and vegetable consumption and physical activity. In addition, CDC's REACH 2010 communities have demonstrated improvements in the consumption of fruits and vegetables and in physical activity in their target populations as a result of community interventions.†† References
* Additional information available at http://www.nhlbi.nih.gov/guidelines/cholesterol/atp3xsum.pdf and http://caonline.amcancersoc.org/cgi/content/full/56/5/254. † The percentage of persons who completed interviews among all eligible persons, including those who were not successfully contacted. Rates available at http://www.cdc.gov/brfss/technical_infodata/2005qualityreport.htm. § The percentage of persons who completed interviews among all eligible persons who were contacted. ¶ Available at http://www.cdc.gov/brfss/technical_infodata/quality.htm. ** Additional information available at http://www.cdc.gov/nccdphp/dnpa. †† Additional information available at http://www.cdc.gov/reach2010.
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to [email protected].Date last reviewed: 4/5/2007 |
|||||||||
|