|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
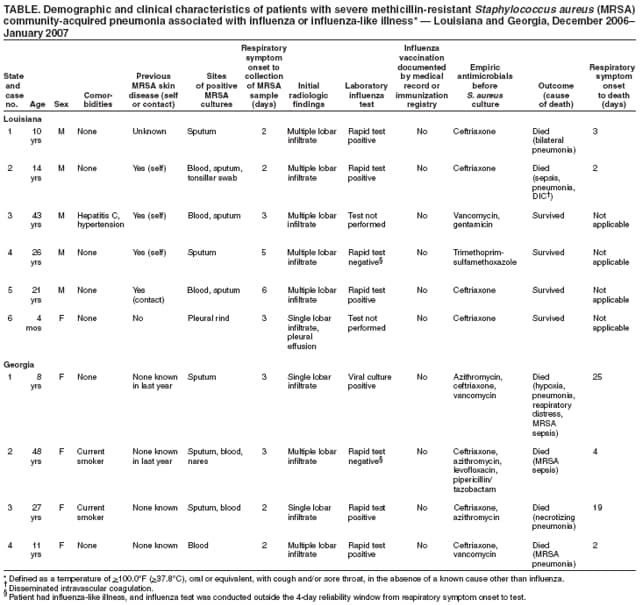
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail. Severe Methicillin-Resistant Staphylococcus aureus Community-Acquired Pneumonia Associated with Influenza --- Louisiana and Georgia, December 2006--January 2007Staphylococcus aureus infection has been reported infrequently as a cause of community-acquired pneumonia (CAP) and typically has been associated with influenza virus infection or influenza-like illness (ILI).* During the 2003--04 influenza season, methicillin-resistant S. aureus (MRSA) gained attention as a cause of 15 cases of influenza-associated CAP† (1). No formal surveillance has been conducted, and few additional cases of MRSA CAP were reported to CDC during the 2004--05 and 2005--06 influenza seasons. However, in January 2007, CDC received reports of 10 cases of severe MRSA CAP, including six deaths, among previously healthy children and adults in Louisiana and Georgia during December 2006--January 2007. These were the first reported cases of severe MRSA CAP during the 2006--07 influenza season in the two states, and 10 was a higher number than expected for the 2-month period. A case of severe MRSA CAP was defined as pneumonia requiring hospitalization or resulting in the death of a patient from whom a specimen (i.e., sterile site or sputum sample) yielded MRSA when collected <48 hours after hospitalization or arrival at an emergency department (ED). Association with influenza was determined by either a positive result on a laboratory test or a diagnosis of ILI. This report describes three of the MRSA CAP cases as examples and summarizes all 10 of the reported cases. These cases underscore the need for health-care providers to be vigilant, especially during the influenza season, for severe cases of CAP that might be caused by MRSA. Case ReportsLouisiana case 1. A previously healthy boy aged 10 years (Table) became ill with fever, cough, sore throat, and bilateral earache on December 6, 2006, and was treated with acetaminophen at home. The next day, his symptoms worsened and he was taken to a local ED in respiratory distress with a fever of 104°F (40°C). A chest radiograph was performed and revealed mutlilobar pneumonia. The patient was transferred to another hospital and admitted to the pediatric intensive care unit (PICU), where he required endotracheal intubation and mechanical ventilation. He was treated initially on December 7 with intravenous (IV) ceftriaxone; vancomycin was started the next day. On December 8, a rapid immunochromatographic assay for the qualitative detection of influenza A or B was performed on nasopharyngeal secretions and was positive for influenza A. A sputum culture obtained the same day grew MRSA; blood cultures were negative. The patient had leukopenia and worsening hypotension and hypoxia. He died on December 9, approximately 42 hours after admission to the PICU. The cause of death was reported as bilateral pneumonia. The patient had no documented history of MRSA; no documentation of influenza vaccination was present in either his medical record or the statewide immunization database, Louisiana Immunization Network for Kids Statewide (LINKS). Louisiana case 2. An adolescent boy aged 14 years (Table) had ILI symptoms on December 26, 2006, and was taken to a local ED, where he was treated with clarithromycin and penicillin for atypical pneumonia and pharyngitis. A rapid test for group A streptococcus was negative. The following day, the patient was taken to his primary-care provider with worsening symptoms and was prescribed oseltamivir for suspected influenza. On December 28, the youth returned to the ED in respiratory distress and was noted to have bloody, frothy sputum; a fever of 104°F (40°C); and hypoxia. In the ED, the patient was intubated, placed on mechanical ventilation, and administered IV ceftriaxone and vancomycin. A chest radiograph revealed diffuse bilateral infiltrates, and a computed tomography scan of his chest revealed extensive bilateral lung consolidation and small anterior mediastinal and posterior pneumothoraces. A rapid immunochromatographic assay performed on nasopharyngeal secretions was positive for influenza A, and a blood culture grew MRSA. The patient died on December 28, approximately 6 hours after arrival in the ED; cause of death was recorded as pneumonia, sepsis, and disseminated intravascular coagulation. At autopsy, the lungs displayed necrotizing pneumonia. Immunohistochemical assay in the lung revealed evidence of S. aureus (positive antigens using monoclonal and polyclonal anti-S. aureus antibodies) in the areas of pneumonia; however, the tissues did not indicate evidence of influenza A or B by immunohistochemistry. MRSA was recovered from a tonsillar swab and lung specimen. Influenza vaccination had not been documented in the patient's medical record or in LINKS. His medical history was unremarkable except for a culture-confirmed axillary MRSA abscess that was diagnosed on October 9, 2006, and treated with trimethoprim-sulfamethoxazole for 7 days. Georgia case 1. A previously healthy girl aged 8 years (Table) was taken to her primary-care provider on December 17, 2006, after 3 days of fever (maximum: 103.0°F [39.4°C]), cough, and posttussive emesis. She was treated in the provider's office with azithromycin, dexamethasone, and aerosolized albuterol. Her condition worsened, and she was transported to a local ED, where she received IV ceftriaxone and nebulized albuterol. A chest radiograph revealed a right lower lobe pneumonia. She was transported to a referral hospital, where she was noted to be hypotensive and hypoxemic. She was intubated on arrival and placed on extracorporeal membrane oxygenation. During intubation, she had cardiac arrest and was resuscitated. Also on December 17, viral and sputum cultures were collected that tested positive for influenza A and MRSA, respectively; blood cultures were negative for MRSA. After a long hospital course complicated by renal and hepatic failure and a subpulmonic abscess, the patient died on January 7, 2007, a total of 25 days after onset of symptoms. Cause of death was listed as hypoxia, pneumonia, respiratory distress, and MRSA sepsis. Influenza vaccination was not documented in the medical record or in the Georgia Registry of Immunization Transactions and Services. Summary of 10 CasesTen cases of severe MRSA CAP were reported during December 2006--January 2007 from Louisiana and Georgia (Table). Median age of the 10 patients was 17.5 years (range: 4 months to 48 years), and eight were aged <30 years. Five of the patients were female. One patient had a history of chronic hepatitis C and hypertension, and two were current smokers; none of the other patients had any relevant medical history. Four patients had documentation of either recent MRSA skin and soft tissue infection (SSTI) or living with someone with a history of MRSA SSTI. In all 10 cases, clinicians diagnosed ILI either preceding or concurrent with CAP. Six patients had laboratory-confirmed influenza. Influenza vaccination status for the 2006--07 influenza season was available for six of the patients; none had documentation of vaccination. Radiologic information on the initial evaluation was available for all patients; three had unilobar infiltrates, and seven had multilobar infiltrates. In three patients, MRSA was isolated only from sputum. Respiratory symptoms for the 10 patients began a median of 3 days (range: 2--6 days) before collection of specimens that grew MRSA. Of the six (60%) patients who died, the median period from respiratory symptom onset to death was 3.5 days (range: 2--25 days). Laboratory FindingsAmong the 10 cases, MRSA isolates from five of the six Louisiana cases were available for microbiologic characterization by CDC. All isolates were resistant to beta-lactams and erythromycin, two had inducible resistance to clindamycin, and two were not susceptible to levofloxacin. All isolates were positive for Panton-Valentine leukocidin (PVL) toxin genes by polymerase chain reaction and carried the staphylococcal cassette chromosome mec (SCCmec) type IVa resistance gene cassette. Pulsed-field gel electrophoresis analysis revealed that the five isolates had indistinguishable patterns and were designated USA 300-0114. Reported by: M Pogue, S Burton, MPH, P Kreyling, MPH, J Naponick, MD, J Stefanski, MD, R Ratard, MD, Louisiana Office of Public Health. S Bulens, MPH, J Cope, MPH, J Tuttle, MD, J Ladson, MPH, M Tobin-D'Angelo, MD, K Arnold, MD, Georgia Div of Public Health. J Hageman, MHS, R Gorwitz, MD, G Fosheim, MPH, S McAllister, K Anderson, J Patel, PhD, B Limbago, PhD, Div of Healthcare Quality Promotion, National Center for Preparedness, Detection, and Control of Infectious Diseases; A Fry, MD, L Brammer, MPH, R Dhara, MPH, D Shay, MD, Influenza Div, National Center for Immunization and Respiratory Diseases; J Guarner, MD, S Zaki, MD, PhD, Infectious Disease Pathology Activity, National Center for Zoonotic, Vector-Borne, and Enteric Diseases; J Brunkard, PhD, A Kallen, MD, EIS officers, CDC. Editorial Note:As demonstrated by the cases in this report, secondary S. aureus pneumonia is a potentially catastrophic complication of influenza. S. aureus respiratory coinfections often develop into severe, necrotizing pneumonia with a relatively high case-fatality rate (33% during the influenza epidemic of 1968--1969) and rapid clinical progression (e.g., death within 24 hours after admission) (2). S. aureus pneumonia has been complicated further by the emergence of MRSA as a cause of infection among persons in the community without traditionally recognized MRSA risk factors (3). During the 2003--04 influenza season, 15 cases of influenza-associated CAP caused by MRSA and four deaths (fatality rate: 26.7%) were reported to CDC, generally in persons with no medical problems (1,4). Reports of pediatric mortality associated with bacterial coinfections with influenza virus infection have been uncommon. During the 2003--04 influenza season, 153 influenza-associated pediatric deaths were reported through state health departments to CDC; 102 of these had bacterial cultures obtained, and 11 were positive for S. aureus, primarily CAP infections (5). Pediatric influenza deaths were made nationally notifiable in 2004. During October 1, 2004--January 19, 2007, a total of 99 pediatric deaths associated with influenza were reported to CDC. Of these, 13 were tested for concomitant invasive bacterial infections, and only four had invasive S. aureus coinfection; two of those four deaths are reported here. Particularly notable in the 10 cases described in this report is the short period between any respiratory symptom onset and either death or recovery of MRSA from the patient. Respiratory symptoms began a median of 3 days before recovery of MRSA, and four (67%) of six patients who died did so within 4 days of respiratory symptom onset. These short durations suggest that, in these cases, the influenza virus and MRSA infections likely occurred concomitantly rather than in the more classically described biphasic clinical course of CAP symptoms after influenza illness (6). In the United States, the majority of community-associated MRSA infections have been SSTIs caused by a single pulsed-field type, termed USA300. USA300 isolates typically are resistant only to beta-lactam and macrolide antimicrobial agents and contain genes for the PVL toxin, which lyses white blood cells; these genes typically are not present in strains of health-care--associated MRSA (7). A recent study with an acute pneumonia animal model determined that PVL was associated with the development of necrotizing pneumonia (8). In general, diagnostic testing for CAP is encouraged if the results might affect clinical decisions (e.g., antimicrobial management). In 30% of the cases in this report, MRSA was recovered only from sputum. The recently released Infectious Disease Society of America/American Thoracic Society CAP guidelines for adults recommend sputum cultures along with blood cultures and other diagnostic tests for certain patients (e.g., those with severe disease). Other indications for sputum culture include pleural effusion, cavitary infiltrates, and failure of outpatient therapy; all of these indications were observed among the MRSA patients described in this report. The guidelines also note that sputum Gram stain is useful for quickly identifying pathogens such as S. aureus that are not the most common causes of CAP and might not be covered by routine empiric therapy (9). Beginning optimal therapy quickly can reduce mortality (9). Four patients in this report had a documented history of MRSA skin infection in themselves or in a close contact before contracting pneumonia. The presence of preceding staphylococcal skin disease among persons with staphylococcal pneumonia has been described previously during an influenza pandemic (10). The index of suspicion for MRSA CAP, therefore, should be increased in patients with a history of MRSA infection or close contact with an MRSA-infected person or in communities where MRSA infections have been identified. If MRSA CAP is suspected, clinicians should add vancomycin or linezolid to the empiric regimen (9). These cases serve to remind health-care providers that CAP can be caused by MRSA. Although uncommon, MRSA CAP has few obvious characteristics that differentiate it from other bacterial infections or from influenza virus infection alone; MRSA CAP often affects young, otherwise healthy persons and can be rapidly fatal. MRSA should be suspected in persons with severe pneumonia, especially during the influenza season, in those with cavitary infiltrates, and in those with a history of MRSA infection. Fatal cases of MRSA CAP or cases requiring hospitalization or ICU admission should be reported through state health departments to CDC's Division of Healthcare Quality Promotion by telephone (800-893-0485) or e-mail ([email protected]). Acknowledgments This report is based, in part, on contributions by C Jones-Nazar, MD, D Robertson, J Eavey, MPH, Louisiana Office of Public Health; L Kravet, Louisiana State Public Health Laboratory; F Brian, MD, Rapides Parish Coroner's Office; LJ Mayeux, MD, Avoyelles Parish Coroner's Office; and C Trant, MD, Lafayette Parish Coroner's Office, Louisiana. References
* Defined as a temperature of >100.0°F (>37.8°C), oral or equivalent, with cough and/or sore throat, in the absence of a known cause other than influenza. † Defined as pneumonia occurring during the 2003--04 influenza season in a person with either laboratory-confirmed influenza virus infection, clinician-determined ILI (e.g., fever plus sore throat or cough), or both, from whom a specimen (i.e., blood, sputum, or pleural fluid) that was collected within 48 hours after hospitalization yielded S. aureus.
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to [email protected].Date last reviewed: 4/12/2007 |
|||||||||
|