|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
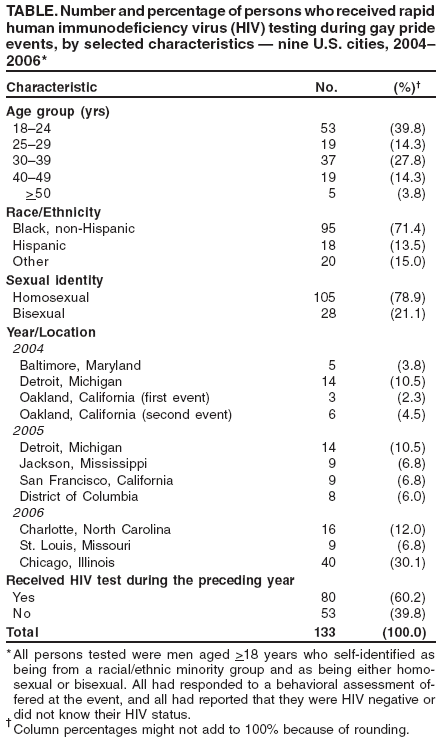
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail. Rapid HIV Testing Among Racial/Ethnic Minority Men at Gay Pride Events --- Nine U.S. Cities, 2004--2006In the United States, human immunodeficiency virus (HIV) and acquired immunodeficiency syndrome (AIDS) disproportionately affect men from racial/ethnic minority groups (1). Approximately half of the HIV/AIDS cases among non-Hispanic black and Hispanic males reported by 33 states using name-based HIV surveillance during 2001--2005 were among men who have sex with men (MSM) (1). Each year, approximately 100 gay pride events are held in cities across the United States to celebrate diversity, demonstrate solidarity of the gay community, and heighten awareness of topics of importance to the gay community. These events are attended by several hundred to several hundred thousand MSM. Certain gay pride events are focused on celebrating solidarity in the minority gay community and are attended primarily by MSM from racial/ethnic minority groups. These events offer an opportunity for community-based organizations (CBOs) and health departments to provide HIV-prevention education and outreach. In 2004, CBOs and health departments, with technical assistance from CDC, began conducting rapid behavioral assessments at gay pride events and at minority gay pride events (2). This report describes the results of assessments and rapid HIV testing conducted at 11 events in nine U.S. cities during 2004--2006; most of these events were attended primarily by MSM from racial/ethnic minority groups. A total of 543 attendees who participated in the assessments reported at the time of the event that they had not had HIV infection diagnosed previously. Of these, 133 (24%) were tested for HIV during the event, and eight (6%) of those tested during the event had a positive rapid test result. All eight were subsequently confirmed to be HIV positive by Western blot testing. Testing at gay pride events provides an opportunity to identify new HIV infections among MSM outside of health-care settings, particularly those from racial/ethnic minority groups. As part of an initiative to reduce racial/ethnic disparities in HIV infection, the U.S. Conference of Mayors, through a cooperative agreement with CDC, provided funding to CBOs and health departments to conduct behavioral assessments at gay pride events attended primarily by MSM from racial/ethnic minority groups. CDC provided on-site technical assistance to the CBO and health department staff, including developing assessment questionnaires, training interviewers, and coordinating HIV testing and questionnaire administration. During 2004--2006, CBOs and health departments were funded to conduct assessments and HIV testing at 1) black gay pride events in Detroit, Michigan (2004 and 2005), Baltimore, Maryland (2004), Jackson, Mississippi (2005), Charlotte, North Carolina (2006), St. Louis, Missouri (2006), and the District of Columbia (2005); 2) Hispanic gay pride events in Oakland (2004) and San Francisco, California (2005); and 3) gay pride events in Oakland, California (2004), and Chicago, Illinois (2006). Both volunteer and paid interviewers were stationed in multiple places at event sites. Interviewers approached and invited adult attendees to participate in a behavioral assessment. At some events, attendees were offered nonmonetary incentives (typically valued at <$10) to increase participation. Assessments were conducted using a two-page, self-administered questionnaire in 2004 and a more comprehensive questionnaire administered by local staff using hand-held personal computers during 2005--2006. The assessment questionnaires included questions about demographic characteristics, sexual behavior, illicit drug use, HIV status, history of testing for HIV and other sexually transmitted diseases (STDs), and access to HIV and STD prevention services. After completing the questionnaire, respondents who said they were HIV negative or did not know their HIV status were offered rapid HIV testing using the OraQuick® Advance™ Rapid HIV-1/2 Antibody Test (OraSure Technologies, Inc., Bethlehem, Pennsylvania). Because a positive rapid HIV test is considered to be a preliminary result, persons with preliminary positive results were asked to provide an oral fluid or blood specimen for confirmatory Western blot testing. Rapid HIV testing at the 11 events was performed in diverse settings, including tents, mobile testing units, community centers, churches, bars, and hotel rooms. Of 627 male respondents aged >18 years who self-identified as being from a racial/ethnic minority group and as being either gay or bisexual, 543 reported that they were HIV negative or did not know their HIV status. Of these, 133 (24%) were tested for HIV at an event (Table). Of the 133 respondents who were tested, eight (6%) had preliminary positive test results. All eight were subsequently confirmed to be HIV positive by Western blot testing. The median age of the eight HIV-positive respondents was 36 years (range: 21--43 years), and seven were non-Hispanic blacks. Four of the eight newly identified HIV-positive respondents reported having had a negative HIV test result during the preceding year, one had never been tested for HIV, and the testing histories of three were unknown. Of the 169 persons who were willing to be tested at a 2005 or 2006 event, 105 (62%) were tested; data for 2004 were unavailable. Although the reasons willing respondents were not tested were not collected systematically, anecdotal reports from staff at events suggest that the primary reasons were that respondents did not report to testing locations after completing the behavioral assessment or, if they did report to testing locations, they chose not to wait until staff were available to administer a test. Data on health-care--seeking behaviors were available from the 2005 assessments only. Of the 229 respondents in 2005 who reported that they were HIV negative or did not know their HIV status, 23 (10%) had received a referral for HIV testing from a health-care provider or outreach worker during the preceding year, and 169 (74%) respondents had visited a health-care provider during the preceding year. Of these 169 respondents, 70 (41%) had been offered an HIV test by their health-care provider. Reported by: T Dowling, MA, MPH, O Macias, D Sebesta, PhD, San Francisco Dept of Public Health, E Antonio, Mission Neighborhood Health Center, C Emerson, Tenderloin Health, San Francisco; L Hinojosa, Alameda County Office of AIDS Admin, Oakland, California. P LaKosky, MA, Chicago Dept of Public Health, Chicago, Illinois. C Bolden Calhoun, Community Health Awareness Group, Detroit; L Randall, PhD, Michigan Dept of Community Health. B Tucker, Women Accepting Responsibility, Inc., Baltimore; C Flynn, ScM, Maryland Dept of Health and Mental Hygiene. M Robinson, Pride of Mississippi, Inc., H Mangum, MSSW, Grace House Inc., Jackson; C Thompson, Mississippi Dept of Health. D Wrigley, St. Louis City Health Dept, St. Louis, Missouri. M Buie, MA, D Bost, North Carolina Dept of Health and Human Svcs. A Smith, MA, Whitman-Walker Clinic, District of Columbia. E Begley, MPH, B Boyett, MS, H Clark, MPH, J Heffelfinger, MD, K Jafa-Bhushan, MBBS, J Schulden, MD, B Song, MS, P Thomas, PhD, P Sullivan, DVM, PhD, Div of HIV/AIDS Prevention, National Center for HIV/AIDS, Viral Hepatitis, STD, and TB Prevention; A Voetsch, PhD, EIS Officer, CDC. Editorial Note:Of the estimated 1 million persons living with HIV infection in the United States, approximately 25% do not know their HIV status (3). In 2003, the CDC initiative Advancing HIV Prevention: New Strategies for a Changing Epidemic called for implementation of new models for diagnosing HIV infections (4). Rapid HIV testing can increase the number of persons who are willing to be tested and the proportion of persons tested who receive their results (5). The findings in this report suggest that rapid HIV testing of MSM in racial/ethnic minority groups at gay pride events is a useful way to enable HIV-infected persons to learn their HIV status. Overall, of the persons who reported that they were HIV negative or who did not know their HIV status during the assessment and who were tested at gay pride events, 6% had positive HIV test results. This result is comparable to the 7% of minority MSM with a positive HIV test result in 2004 at CDC-supported testing sites, which included hospitals, public health and STD clinics, prisons and jails, drug treatment centers, and outreach settings (6). Four of the eight men who were newly identified as infected with HIV had received negative HIV test results during the preceding year. Men who mistakenly believe that they are HIV negative, even those who have this belief based on a recent negative HIV test, represent an important risk group for HIV transmission. For example, 47 (7%) of the 723 MSM in the Young Men's Survey who had received negative HIV test results during the preceding year and disclosed that they were HIV negative to their sex partners were unaware that they were HIV positive (7). Knowledge of being infected with HIV has been associated with reduction of high-risk behaviors (8). CBOs and health departments face several challenges when conducting rapid HIV testing at gay pride events. The effectiveness of testing depends, in part, on the amount of resources that CBOs and health departments can dedicate to such events. The demand for rapid HIV testing at several of the events described in this report exceeded the capacity of CBO and health department staff to provide testing. Persons who could not be tested during the event were referred for testing at a later date. Effectiveness also depends on proper follow up of persons with newly diagnosed HIV. Two of the eight MSM with newly diagnosed and confirmed HIV infection were not referred to medical care because they could not be located after the event. HIV testing at gay pride events is only one part of a greater strategy to encourage HIV testing among MSM. HIV testing provided by CBOs and health departments outside of the health-care setting, such as at gay pride events, is an important strategy to reach MSM who might not regularly access health care. Among persons for whom health-care--seeking behavior information was available, 74% had visited a health-care provider during the preceding year; however, only 41% had been offered HIV testing by a provider during the preceding year. To decrease the number of missed opportunities for HIV testing, in 2006, CDC recommended that HIV testing for patients aged 13--64 years become a routine part of medical services using a voluntary, opt-out approach. CDC further recommended that persons likely to be at high risk for HIV infection, including sexually active MSM, be tested at least annually (9). Future analyses of outreach activities such as the ones described in this report can be used to understand barriers to HIV testing among MSM and help determine the cost-effectiveness of such activities for health departments and CBOs. Expansion of HIV testing opportunities for racial/ethnic minorities outside of health-care settings, combined with culturally appropriate behavioral interventions, are important components of ongoing CDC activities to reduce HIV transmission and eliminate disparities in the rates of HIV infection by race and ethnicity. References
|
Use of trade names and commercial sources is for identification only and does not imply endorsement by the U.S. Department of
Health and Human Services. |
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices.
**Questions or messages regarding errors in formatting should be addressed to [email protected].Date last reviewed: 6/21/2007
|
|
|||||
|
HOME |
ABOUT MMWR |
MMWR SEARCH |
DOWNLOADS |
RSS
|
CONTACT
|
|||||
|
|
|||||
|