|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
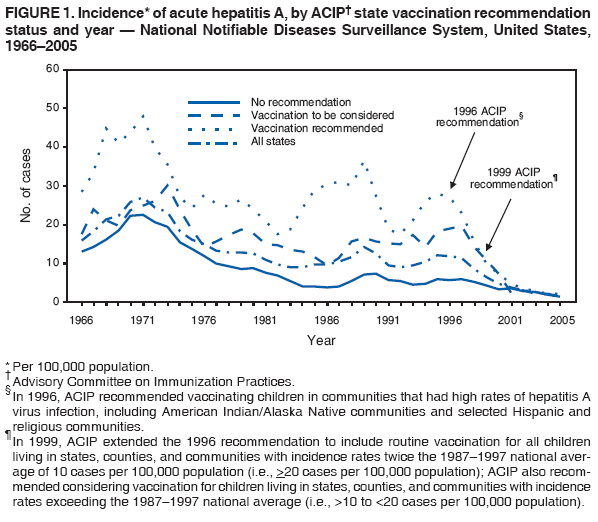
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail. Hepatitis A Vaccination Coverage Among Children Aged 24--35 Months --- United States, 2004--2005After the licensure of hepatitis A vaccine in 1995 for children aged >24 months, the Advisory Committee on Immunization Practices (ACIP) incrementally expanded the proportion of children for whom it recommended the vaccine. In 1996, ACIP recommended vaccinating children in communities that had high rates of hepatitis A virus (HAV) infection, including American Indian/Alaska Native (AI/AN) communities and selected Hispanic and religious communities (1). In 1999, ACIP extended the recommendation to include routine vaccination for all children living in states, counties, and communities with incidence rates twice the 1987--1997 national average of 10 cases per 100,000 population (i.e., >20 cases per 100,000 population); ACIP also recommended considering vaccination for children living in states, counties, and communities with incidence rates exceeding the 1987--1997 national average (i.e., >10 to <20 cases per 100,000 population) (2). National estimates of hepatitis A vaccination coverage were first made available through the 2003 National Immunization Survey (NIS), which indicated an overall national 1-dose coverage level of 16.0% (range: 6.4%--72.7%) among children aged 24--35 months (3). The estimates in this report update those findings by including 2 additional years of data (2004 and 2005). National 1-dose vaccination-coverage levels among children aged 24--35 months increased from 17.6% in 2004 to 21.3% in 2005. Coverage in states where vaccination was recommended (overall in 2005: 56.5%; range: 12.9%--71.0%) was below those for other recommended childhood vaccinations, such as varicella (87.5% in 2004) (4). Despite low hepatitis A vaccination-coverage levels compared with other recommended childhood vaccinations, incidence of acute HAV infections have declined to the lowest level ever recorded (5) (Figure 1). The 2005 licensure of the hepatitis A vaccine for use in younger children (aged >12 months) and the 2006 ACIP guideline for routine hepatitis A vaccination of all children aged >12 months (6) should result in improved vaccination coverage and further reductions in disease incidence. NIS provides vaccination coverage estimates among noninstitutionalized children aged 19--35 months for the 50 states
and selected cities and counties. To obtain vaccination data, NIS conducts a random-digit--dialed telephone survey of
households and a mail survey of the children's vaccination providers. Data are weighted to adjust for households with multiple
telephone lines, household nonresponse, and noninclusion of households without landline telephones
(7). The household survey response rate was 67.4% in 2004 and 65.1% in 2005. Among children aged 19--35 months for whom household
interviews were completed, health-care provider vaccination records were obtained for 21,998 children (71.0%) in 2004 and
17,563 children (63.6%) in 2005. Among the children with vaccination records, age criteria for this assessment (24--35 months)
were met by 14,143 children in 2004 and 12,203 in 2005. Although hepatitis A vaccine is licensed as a 2-dose regimen, data
are presented for 1-dose vaccination coverage, which has been determined to convey serologic protection in 96% of children
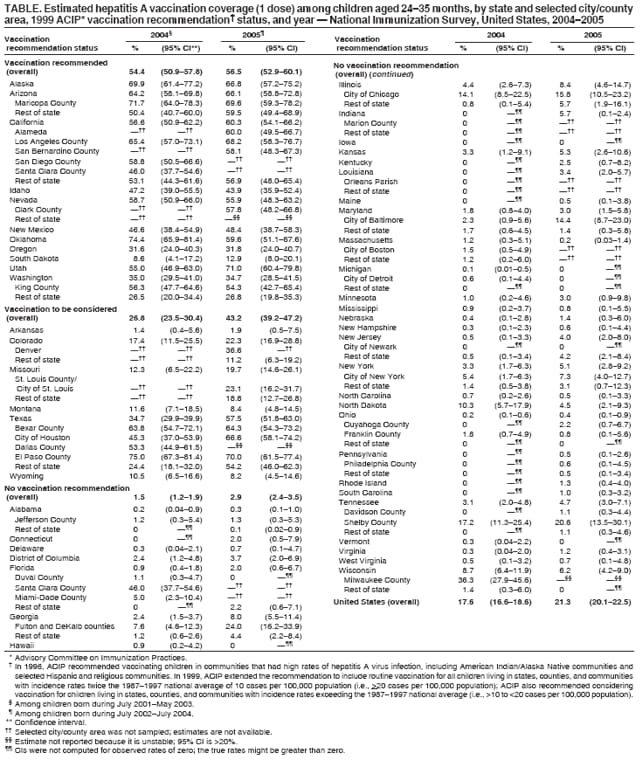
aged <6 years (8). A statistically significant increase was observed in estimated national 1-dose hepatitis A vaccination coverage, from 17.6%
in 2004 to 21.3% in 2005 (Table). Coverage was greater in states where vaccination was recommended by ACIP, compared
with states where vaccination was to be considered or where no specific recommendation was in effect. In the 11 states
where vaccination was recommended, 1-dose coverage was 54.4% (range: 8.6%--74.4%) in 2004 and 56.5% (range:
12.9%--71.0%) in 2005. In the six states where vaccination was to be considered, 1-dose coverage was 26.8% (range: 1.4%--34.7%) in
2004 and 43.2% (range: 1.9%--57.5%) in 2005. In the District of Columbia and the 33 states where no specific
recommendation for vaccination was in effect, coverage was 1.5% (range: 0%--10.3%) in 2004 and 2.9% (range: 0%--8.4%) in
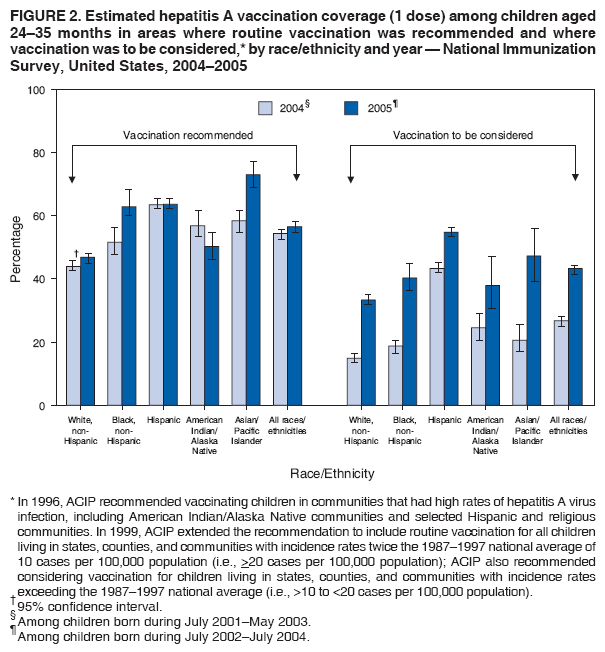
2005. From 2004 to 2005, vaccination coverage increased more in states where ACIP recommended that vaccination be considered (16.4%) than in states where ACIP recommended routine vaccination (2.1%) or where no specific recommendation was in effect (1.4%). The significant increase in states where vaccination was to be considered primarily resulted from increased coverage in Texas (from 34.7% in 2004 to 57.5% in 2005). In states where vaccination was recommended or to be considered, non-Hispanic blacks, Hispanics, AI/ANs, and Asians/Pacific Islanders (A/PIs) had greater vaccination coverage rates than non-Hispanic whites (Figure 2). In 2005, coverage in states where vaccination was recommended ranged from 46.9% among non-Hispanic whites to 72.9% among A/PIs. In states where vaccination was to be considered, coverage in 2005 ranged from 33.3% among non-Hispanic whites to 54.7% among Hispanics. For all racial/ethnic groups, coverage increased from 2004 to 2005 in states where vaccination was to be considered. Reported by: I Williams, PhD, A Wasley, ScD, Div of Viral Hepatitis, National Center for HIV/AIDS, Viral Hepatitis, STD, and TB Prevention; N Darling, MPH, J Singleton, MS, National Center for Immunization and Respiratory Diseases; G Fischer, MD, EIS Officer, CDC. Editorial Note:The NIS findings from 2004 and 2005 are similar to those from 2003; states where routine hepatitis A vaccination was recommended had greater vaccination coverage compared with states where vaccination was to be considered or where no specific recommendation for vaccination was in effect. However, even in states where hepatitis A vaccination was recommended, coverage remained below levels observed for other vaccinations that were recommended during a comparable period. For example, 1-dose vaccination coverage of varicella vaccine, which has been routinely recommended for children aged 12--18 months since 1996, was 76.3% (95% confidence interval [CI] = 75.5%--77.1%) in 2001 and 80.6% (CI = 79.7%--81.5%) in 2002 for children aged 19--35 months. Coverage with 1 dose of measles, mumps, and rubella vaccine, which became available in 1971, was 93.0% (CI = 92.4%--93.6%) in 2004 (4). Despite low levels of 1-dose hepatitis A vaccination coverage compared with other recommended vaccinations, the number of cases and rates of acute hepatitis A in the United States have declined substantially, especially among racial/ethnic groups disproportionately affected by hepatitis A. Before the 1995 introduction of hepatitis A vaccine for children aged >24 months, rates of acute hepatitis A were five times greater than the national average among AI/ANs and three times greater among Hispanics (1). In 2005, acute hepatitis A rates among AI/ANs were comparable to other populations but remained greater for Hispanics compared with non-Hispanics (9). This trend demonstrates progress toward eliminating racial/ethnic disparities previously observed in rates of acute hepatitis A. The overall number of cases and rates of acute hepatitis A in the United States have declined to historic lows since the last peak in 1995. In 1995, a total of 31,582 cases were reported (12 per 100,000 population), compared with 4,488 cases (1.5 per 100,000) in 2005, which was the lowest annual number ever recorded (5). In 2005, similar rates of acute hepatitis A were reported by states where vaccination was recommended (2.1 per 100,000), states where vaccination was to be considered (1.5 per 100,000), and states where no specific recommendation for vaccination was in effect (1.3 per 100,000) (CDC, unpublished data, 2005). Even limited vaccination coverage might reduce disease incidence through herd effects because young children are thought to be a major reservoir of infection. In one communitywide outbreak, approximately 40% of adults with hepatitis A without an identifiable source lived with a child aged <6 years who had evidence of recent HAV infection (10). Declines also might be the result of cyclic increases and decreases in HAV infections (9). The findings in this report are subject to at least four limitations. First, NIS is a telephone survey, and statistical adjustments might not fully compensate for nonresponse and households without telephones. Second, NIS relies on provider-verified vaccination histories; vaccination coverage might be underestimated if providers have incomplete records or if incomplete reporting of hepatitis A vaccination has occurred. Third, children who are older than the 24--35 months age group described in this report might have greater hepatitis A vaccination coverage because ACIP recommendations state that community disease patterns should determine which age groups to vaccinate (2). Finally, changes in vaccination coverage levels from 2004 to 2005 might be underestimated because the sampled birth cohorts overlap. The data in this report do not explain differences in coverage levels among states; however, variations in state mandates for vaccination might provide one explanation for these differences. Statewide day care or school-entry mandates were in effect in six of the 11 states where vaccination was recommended. Intrastate regional mandates were in effect in one of six states where vaccination was to be considered and in one of 33 states where no specific recommendation for vaccination was in effect.* In August 2005, hepatitis A vaccine was licensed by the Food and Drug Administration for use in younger children (aged >12 months). In 2006, ACIP recommended routine vaccination of all children aged >12 months regardless of risk category or geographic location (6). This recommendation should decrease hepatitis A incidence in states where vaccination was not recommended previously and should sustain reductions in places where hepatitis A vaccination has been recommended since 1999. References
* Additional information available at http://www.immunize.org/laws/hepa.htm.
Figure 1
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to [email protected].Date last reviewed: 7/11/2007 |
|||||||||
|