|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
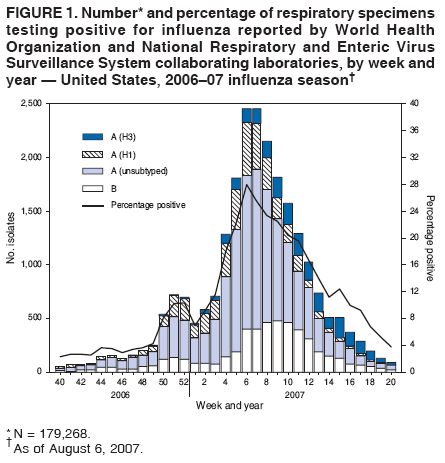
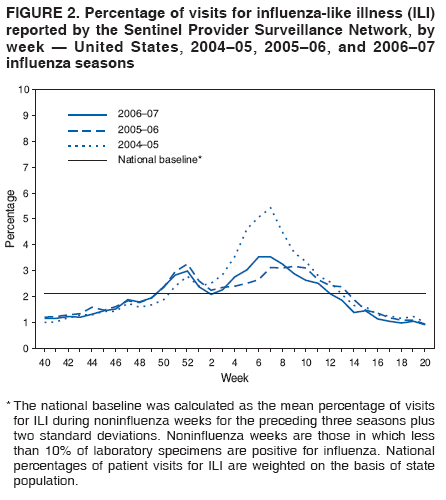
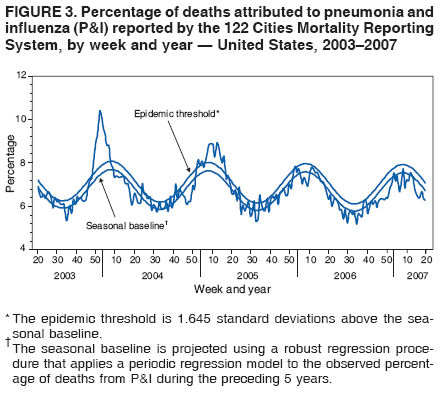
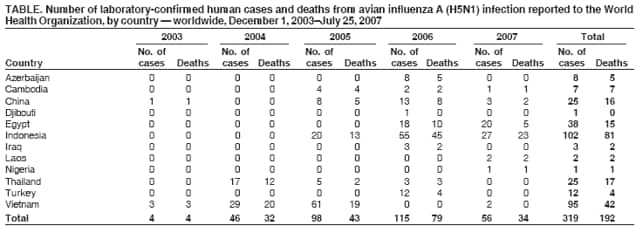
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail. Update: Influenza Activity --- United States and Worldwide, 2006--07 Season, and Composition of the 2007--08 Influenza VaccineDuring the 2006--07 season, influenza activity peaked in mid-February in the United States and was associated with less mortality and lower rates of pediatric hospitalizations than during the previous three seasons. In the United States, influenza A (H1) viruses predominated overall, but influenza A (H3) viruses were isolated more frequently than influenza A (H1) viruses late in the season. Although influenza A (H1), A (H3), and B viruses cocirculated worldwide, influenza A (H3) viruses were the most commonly reported type in Europe and Asia. Sporadic cases of avian influenza A (H5N1) virus infections associated with severe illness or death were reported among humans in Cambodia, China, Egypt, Indonesia, Laos, Nigeria, and Viet Nam. This report summarizes influenza activity in the United States and worldwide during the 2006--07 influenza season (October 1, 2006--May 19, 2007) and describes the composition of the 2007--08 influenza vaccine. United StatesThe national percentage of respiratory specimens testing positive for influenza and the proportion of outpatient visits to sentinel providers for influenza-like illness (ILI)* peaked in mid-February. Although influenza A (H1) viruses were most commonly isolated overall, influenza A (H3) viruses were more frequently identified than influenza A (H1) viruses from early March through May. A small number of influenza B viruses also were identified. Viral SurveillanceDuring October 1, 2006--May 19, 2007, World Health Organization (WHO) and National Respiratory and Enteric Virus Surveillance System (NREVSS) collaborating laboratories in the United States tested 179,268 respiratory specimens for influenza viruses; 23,753 (13.2%) were positive (Figure 1). Of these, 18,817 (79.2%) were influenza A viruses and 4,936 (20.8%) were influenza B viruses. Among the influenza A viruses, 6,280 (33.4%) were subtyped; 3,912 (62.3%) were influenza A (H1) viruses and 2,368 (37.7%) were influenza A (H3) viruses. The proportion of specimens testing positive for influenza first exceeded 10% during the week ending December 23, 2006 (week 51), peaked at 28.0% during the week ending February 10, 2007 (week 6), and declined to less than 10% during the week ending April 28, 2007 (week 17). The proportion was above 10% positive for 14 consecutive weeks. The peak percentage of specimens testing positive for influenza during the previous three seasons ranged from 22.6% to 34.7%, and the peak occurred during early December to early March (1; CDC, unpublished data, 2007). During the previous three influenza seasons, the number of consecutive weeks during which more than 10% of specimens tested positive for influenza ranged from 13 to 17 weeks (1; CDC, unpublished data, 2007). Composition of the Influenza Vaccine for the 2007--08 SeasonThe Food and Drug Administration's Vaccines and Related Biological Products Advisory Committee recommended that the 2007--08 trivalent influenza vaccine for the United States contain A/Solomon Islands/3/2006-like (H1N1), A/Wisconsin/67/2005-like (H3N2), and B/Malaysia/2506/2004-like viruses. This represents a change only in the influenza A (H1N1) component. A/Solomon Islands/3/2006 is a recent antigenic variant of the 2006--07 vaccine strain A/New Caledonia/20/99. The influenza A (H3N2) and influenza B components remain the same. These recommendations were based on antigenic analyses of recently isolated influenza viruses, epidemiologic data, postvaccination serologic studies in humans, and the availability of candidate vaccine strains and reagents. Antigenic CharacterizationSince October 1, 2006, CDC has antigenically characterized 1,107 influenza viruses collected by U.S. laboratories: 486 influenza A (H1) viruses, 289 influenza A (H3) viruses, and 332 influenza B viruses. Of the 486 influenza A (H1) viruses, 439 (90%) were characterized as similar to A/New Caledonia/20/99, the influenza A (H1N1) component recommended for the 2006--07 influenza vaccine. Forty-five (9%) viruses showed reduced titers with antisera produced against A/New Caledonia/20/99 and are similar to A/Solomon Islands/3/2006, which is a recent antigenic variant of A/New Caledonia/20/99 and is the influenza A (H1N1) component recommended for the 2007--08 influenza vaccine. Two influenza A (H1) viruses showed reduced titers with antisera produced against both A/New Caledonia/20/99 and A/Solomon Islands/3/2006. Of the 289 influenza A (H3) viruses, 69 (24%) were characterized as similar to A/Wisconsin/67/2005, the H3N2 component recommended for the 2007--08 vaccine, and 220 (76%) of the 289 viruses showed reduced titers with antisera produced against A/Wisconsin/67/2005. Influenza B viruses currently circulating can be divided into two antigenically distinct lineages represented by B/Yamagata/16/88 and B/Victoria/02/87 viruses. A total of 254 (77%) of the 332 influenza B viruses that have been characterized belong to the B/Victoria lineage: 128 (50%) were similar to B/Ohio/01/2005, and 126 (50%) showed reduced titers with antisera produced against B/Ohio/01/2005. B/Ohio/01/2005 is antigenically equivalent to B/Malaysia/2506/2004, the recommended influenza B component for the 2007--08 influenza vaccine. Seventy-eight (23%) of the 332 influenza B viruses were identified as belonging to the B/Yamagata lineage. Influenza-Like Illness (ILI) SurveillanceThe weekly percentage of patient visits to U.S. sentinel providers for ILI exceeded or was at baseline levels (2.1%)† during the weeks ending December 16, 2006--March 24, 2007 (weeks 50--12) and peaked twice, once at 3.0% for the week ending December 30, 2006 (week 52), and again at 3.5% for the week ending February 17, 2007 (week 7) (Figure 2). The increase in the percentage of patient visits for ILI during the week ending December 30, 2006 (week 52) might have been influenced by a reduction in routine health-care visits during the holiday season, as has occurred in previous seasons. During the previous three influenza seasons, the peak percentage of patient visits for ILI has ranged from 3.3% to 7.6% and the peak occurred during late December to mid-February (1; CDC, unpublished data, 2007). State-Specific Activity LevelsState and territorial epidemiologists report the geographic distribution of influenza in their state through a weekly influenza activity code. The geographic distribution of influenza activity peaked during the week ending February 24, 2007 (week 8), when 25 states reported widespread activity and 19 states reported regional activity.§ Forty-one states reported widespread influenza activity at least once during the 2006--07 season. No states reported widespread influenza activity during the weeks ending April 21--May 19, 2007 (weeks 16--20). The peak number of states reporting widespread or regional activity during the previous three seasons ranged from 41 to 50 states (1; CDC, unpublished data, 2007). Influenza-Associated Pediatric HospitalizationPediatric hospitalizations associated with laboratory-confirmed influenza infections are monitored in two population-based surveillance networks: the Emerging Infections Program (EIP) and the New Vaccine Surveillance Network (NVSN). During October 1, 2006--April 28, 2007, the preliminary influenza-associated hospitalization rate reported by EIP for children aged 0--17 years was 0.81 per 10,000. For children aged 0--4 years and 5--17 years, the rates were 1.62 per 10,000 and 0.23 per 10,000, respectively. During November 5, 2006--May 26, 2007, the preliminary laboratory-confirmed influenza-associated hospitalization rate for children aged 0--4 years in NVSN was 3.46 per 10,000. EIP hospitalization data collection ended on April 28, 2007, whereas NVSN hospitalization data collection ended on May 26, 2007. Rate estimates are preliminary and might continue to change as data are finalized. In years 2000--2006, the end-of-season hospitalization rate for NVSN ranged from 3.7 (2002--03) to 12 (2003--04) per 10,000 children aged 0--4 years. During the 2004--05 influenza season, the end-of-season hospitalization rate for EIP was 3.3 per 10,000 children aged 0--4 years and 0.6 per 10,000 children aged 5--17 years; during the 2005--06 season, the rates were 2.8 and 0.4, respectively. Differences in rate estimates between the NVSN and the EIP systems likely result from different case-finding methods, the diagnostic tests used, and the populations monitored.¶ Pneumonia- and Influenza-Related MortalityDuring the 2006--07 influenza season, the percentage of deaths attributed to pneumonia and influenza (P&I) did not exceed the epidemic threshold** in the 122 Cities Mortality Reporting System (Figure 3). The percentage of P&I deaths peaked three times, once at 7.5% during the week ending January 20, 2007 (week 3), once at 7.7% during the week ending February 24, 2007 (week 8), and again at 7.5% during the week ending March 24, 2007 (week 12). During the previous three influenza seasons, the peak percentage of P&I deaths ranged from 7.8% to 10.4%, and the total number of weeks above the epidemic threshold ranged from one to 16 (1; CDC, unpublished data, 2007). Influenza-Associated Pediatric MortalityAs of August 6, 2007, among persons aged <18 years, a total of 68 deaths associated with influenza infection occurring during October 1, 2006--May 19, 2007, were reported to CDC. These deaths were reported from 26 states (Alabama, Alaska, Arizona, California, Colorado, Connecticut, Florida, Georgia, Illinois, Indiana, Kansas, Louisiana, Minnesota, North Carolina, Nebraska, Nevada, New Mexico, New York, Ohio, Oklahoma, South Dakota, Tennessee, Texas, Virginia, Washington, and Wisconsin). All patients had laboratory-confirmed influenza virus infection. Age-specific information was available for all 68 persons; 10 were aged <6 months, 10 were aged 6--23 months, nine were aged 2--4 years, and 39 were aged 5--17 years. Of the 63 patients for whom influenza virus type was known, 47 had influenza A and 16 had influenza B viruses. Of the 53 patients aged >6 months for whom vaccination status was known, 50 (94%) had not been vaccinated against influenza. These data are provisional. WorldwideDuring the 2006--07 influenza season, influenza A (H1), A (H3), and B viruses cocirculated worldwide. In Africa, small numbers of influenza A and B viruses were reported. In Europe and Asia, influenza A (H3) viruses were identified most frequently, but influenza A (H1) viruses circulated at low levels. Influenza B viruses circulated at lower levels overall in Asia and Europe but predominated in some countries. Human Infections with Avian Influenza A (H5N1) VirusesFrom December 1, 2003, through July 25, 2007, a total of 319 human cases of avian influenza A (H5N1) infection were reported to WHO (2). Of these, 192 (60%) were fatal (Table). All cases were reported from Asia (Azerbaijan, Cambodia, China, Indonesia, Iraq, Laos, Thailand, Turkey, and Viet Nam) and Africa (Djibouti, Egypt, and Nigeria). To date, no human case of avian influenza A (H5N1) virus infection has been identified in the United States. Reported by: WHO Collaborating Center for Surveillance, Epidemiology, and Control of Influenza. L Blanton, MPH, L Brammer, MPH, A Budd, MPH, T Wallis, MS, D Shay, MD, J Bresee, MD, A Klimov, PhD, N Cox, PhD, Influenza Div, National Center for Immunization and Respiratory Diseases, CDC. Editorial Note:During the 2006--07 influenza season, influenza activity in the United States peaked in mid-February, and the percentage of deaths resulting from pneumonia and influenza remained below baseline levels for the entire influenza season. In the United States, influenza A (H1) viruses predominated during most of the season, but influenza A (H3) viruses were more frequently identified than influenza A (H1) viruses since early March. Worldwide, influenza A (H3) viruses predominated in many European and Asian countries. In the United States, the majority of influenza A (H1) viruses were characterized as A/New Caledonia/20/99, the recommended influenza A (H1N1) component of the 2006--07 influenza vaccine. Fifty percent of the influenza B viruses characterized as belonging to the B/Victoria lineage were further characterized as B/Ohio/01/2005, the antigenic equivalent of B/Malaysia/2506/2004, the recommended influenza B component for the 2006--07 influenza vaccine. In the early months of the season, the majority of influenza A (H3) isolates matched the A/Wisconsin/67/2005 strain, the recommended influenza A (H3N2) component for the 2006--07 vaccine. Beginning in late February 2007, the majority of the influenza A (H3) isolates indicated reduced titers with antisera produced against A/Wisconsin/67/2005. States are requested to submit a subset of their summer influenza isolates and any samples that cannot be subtyped by standard methods or are unusual to CDC for further antigenic characterization. In May 2007, a Health Alert Network advisory was issued by CDC regarding an increase in the number of influenza-associated pediatric deaths and coinfections with Staphylococcus aureus during the 2006--07 season (3). Only one pediatric death with influenza and S. aureus coinfection had been reported during 2004--05, and three had been reported during the 2005--06 season (3). Of the 68 reported deaths among children associated with influenza infections during October 1, 2006--May 19, 2007, a total of 21 had coinfections with influenza and either methicillin-resistant or sensitive S. aureus. State health departments have been asked to ensure that all influenza-associated pediatric deaths from the 2006--07 influenza season are reported to CDC. At the June 2007 Annual Meeting of the Council of State and Territorial Epidemiologists (CSTE), members voted to ratify a position statement adopted by the CSTE Executive Committee in January 2007 that adds human infections with novel influenza A viruses to the list of nationally notifiable diseases and conditions reportable to the National Notifiable Disease Surveillance System. Novel influenza A viruses are defined as those isolated from a human but subtyped as nonhuman, or those that cannot be subtyped by standard methods. Human infections with novel influenza A viruses that can be transmitted from person-to-person might signal the beginning of an influenza pandemic. Rapid reporting of human infections with novel influenza A viruses will facilitate prompt detection and characterization of influenza A viruses with pandemic potential and accelerate implementation of effective public health responses. In addition, influenza-associated pediatric deaths were maintained as a nationally notifiable disease reportable to the National Notifiable Disease Surveillance System. In May 2007, health authorities in the United Kingdom identified four persons, two in Wales and two in northwest England, who were infected with a low pathogenic avian influenza A (H7N2) virus (4). All four persons had been exposed to infected poultry at a farm in Wales; limited evidence of human-to-human transmission has been associated with low pathogenic avian influenza viruses such as influenza A (H7N2) virus (4). The United Kingdom incident underscores the importance of submission and identification of unusual influenza isolates. In collaboration with local and state health departments, CDC continues to recommend enhanced surveillance for possible avian influenza A (H5N1) infection among travelers who have severe unexplained respiratory illness and are returning from influenza A (H5N1)-affected countries. Additional information regarding influenza, including avian influenza, is available at http://www.cdc.gov/flu. Updates on the worldwide avian influenza situation are available from WHO at http://www.who.int/csr/disease/avian_influenza/en. Acknowledgments This report is based, in part, on data contributed by participating state and territorial health departments and state public health laboratories, WHO collaborating laboratories, National Respiratory and Enteric Virus Surveillance System collaborating laboratories, the U.S. Influenza Sentinel Provider Surveillance System, the New Vaccine Surveillance Network, the Emerging Infections Program, and the 122 Cities Mortality Reporting System; WHO National Influenza Centers, WHO Global Influenza Programme, Geneva, Switzerland; I Gust, MD, A Hampson, WHO Collaborating Center for Reference and Research on Influenza, Parkville, Australia; A Hay, PhD, WHO Collaborating Center for Reference and Research on Influenza, National Institute of Medical Research, London, England; M Tashiro, MD, WHO Collaborating Center for Reference and Research on Influenza, National Institute of Infectious Diseases, Tokyo, Japan. References
* Defined as a temperature of >100.0°F (>37.8°C), oral or equivalent, and cough and/or sore throat, in the absence of a known cause other than influenza. † The national baseline is the mean percentage of visits for ILI during noninfluenza weeks for the previous three seasons plus two standard deviations. Noninfluenza weeks are those in which less than 10% of laboratory specimens are positive for influenza. National percentages of patient visits for ILI are weighted on the basis of state population. § Levels of activity are 1) no activity; 2) sporadic: isolated laboratory-confirmed influenza cases or a laboratory-confirmed outbreak in one institution, with no increase in ILI activity; 3) local: increased ILI , or at least two institutional outbreaks (ILI or laboratory-confirmed influenza) in one region with recent laboratory evidence of influenza in that region; virus activity no greater than sporadic in other regions; 4) regional: increased ILI activity or institutional outbreaks (ILI or laboratory-confirmed influenza) in at least two but less than half of the regions in the state with recent laboratory evidence of influenza in those regions; and 5) widespread: increased ILI activity or institutional outbreaks (ILI or laboratory-confirmed influenza) in at least half the regions in the state with recent laboratory evidence of influenza in the state. ¶ NVSN provides population-based estimates of laboratory-confirmed influenza hospitalization rates in children aged <5 years admitted to NVSN hospitals with fever or respiratory symptoms. Children are prospectively enrolled, and respiratory samples are collected and tested by viral culture and reverse transcription--polymerase chain reaction (RT-PCR). EIP conducts surveillance for laboratory-confirmed, influenza-related hospitalizations in persons aged <18 years. Hospital laboratory and admission databases and infection-control logs are reviewed to identify children with a positive influenza test (i.e., viral culture, direct fluorescent antibody assays, RT-PCR, or a commercial rapid antigen test) from testing conducted as a part of their routine care. ** The expected seasonal baseline proportion of P&I deaths reported by the 122 Cities Mortality Reporting System is projected using a robust regression procedure in which a periodic regression model is applied to the observed percentage of deaths from P&I during the preceding 5 years. The epidemic threshold is 1.645 standard deviations above the seasonal baseline.
Figure 1
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to [email protected].Date last reviewed: 8/8/2007 |
|||||||||
|