|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
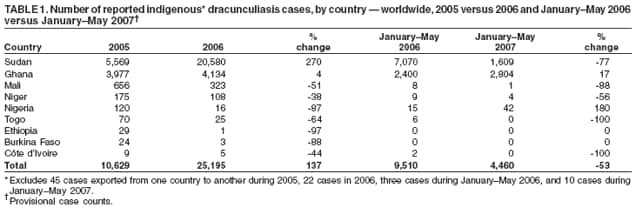
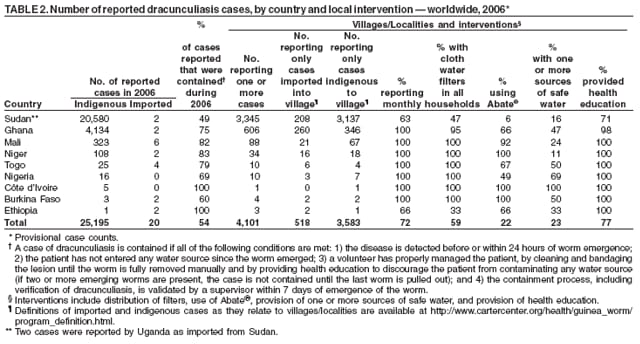
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail. Progress Toward Global Eradication of Dracunculiasis, January 2005--May 2007Please note: An erratum has been published for this article. To view the erratum, please click here. The World Health Assembly first adopted a resolution calling for the eradication of dracunculiasis (Guinea worm disease) in 1986, when an estimated 3.5 million cases were reported in 20 countries, and 120 million persons were at risk for the disease (1,2). This report describes the continued progress of the dracunculiasis eradication program worldwide during July 2005--May 2007 (3,4). As of May 2007, dracunculiasis was still endemic in nine* of the 20 countries cited in 1986; in 2006, approximately 98% of dracunculiasis cases worldwide were reported from Ghana and Sudan, and five other countries reported fewer than 30 cases each (Table 1). The number of dracunculiasis cases increased from 10,674 in 2005 to 25,217 cases in 2006, with nearly all of the increase reported in Sudan, before decreasing from 9,510 during January--May 2006 to 4,460 cases during January--May 2007. Continued intensification of interventions against transmission of dracunculiasis will be necessary to eradicate dracunculiasis in the nine countries where the disease remains endemic. The number of villages worldwide with endemic dracunculiasis decreased from 23,165 in 1993 to 3,583 in 2006 (Table 2). All of the remaining areas where dracunculiasis is endemic are in Africa. Outside of Sudan and Ghana, where the number of dracunculiasis cases increased 159%, from a total of 9,546 in 2005 to 24,714 in 2006, the number of cases reported from the other seven countries where dracunculiasis remains endemic decreased 56%, from 1,083 in 2005 to 481 in 2006. Worldwide, the number of dracunculiasis cases exported from one country to another declined from 114 in 2004, to 45 in 2005, to 22 in 2006. However, a 180% increase was reported from Nigeria during January--May 2007, when the number of cases increased to 42 from 15 during the same period in 2006. Country ReportsSudan. In 2006, the Southern Sudan Guinea Worm Eradication Program was created after political settlement of Sudan's civil war in January 2005. The settlement shifted responsibility for dracunculiasis eradication in remaining areas where the disease was endemic to the ministry of health of the new government of Southern Sudan, composed of 10 southern states. The new eradication program, with the aid of 10,745 trained village volunteers and access to Southern Sudan areas that had been inaccessible during the civil war, provided improved surveillance. The result was a 270% increase in reported cases of dracunculiasis in Sudan, from 5,569 cases in 1,293 villages in 2005 to 20,582 cases in 3,345 villages in 2006, with all but two villages located in Southern Sudan. The last indigenous case of dracunculiasis in northern Sudan occurred in 2001. Three of the 10 southern states reported 92% of all cases in Sudan in 2006; three other southern states reported no indigenous cases. Two cases were imported into Southern Sudan from Ethiopia in 2006, and two in January 2007. During 2006, one case was exported from Southern Sudan to northern Sudan. In addition, Sudan exported two cases of dracunculiasis to Uganda during January--May 2007. In 2006, a total of 63% of 3,137 Sudanese villages with endemic disease filed monthly surveillance reports, compared with 50% of 1,085 villages in 2005. Of the 20,582 cases reported in 2006, 49% were contained,† compared with 4% of 5,565 cases in 2005. The percentage of villages with endemic dracunculiasis receiving health education was 71% in 2006 (compared with 76% in 2005); 47% of the villages had cloth water filters in all households (compared with 30% in 2005), 16% had at least one source of safe drinking water (27% in 2005), and the larvicide Abate® (temephos) (BASF, Ludwigshafen, Germany) was used by 6% (2% in 2005) (Table 2).§ Provisional data from Southern Sudan for January--May 2007 indicated a total of 1,611 reported cases of dracunculiasis, a reduction of 77% from the 7,070 cases reported during the same period in 2006. Ghana. The eradication program in Ghana, which reported an increase of 4% to 4,136 cases (in 606 villages) in 2006 from 3,977 cases in 2005, had a setback resulting from the 2006 breakdown of the municipal water supply in the northern region's capital city of Tamale, which also interrupted the water supply to the nearby city of Savelugu. Commercial vendors in both cities sold contaminated water to residents, who also obtained water from nearby contaminated reservoirs. As a consequence, the number of dracunculiasis cases in Savelugu more than tripled, from 411 cases in 2006 to 1,349 cases during January--May 2007, which accounted for 45% of the cases reported for all of Ghana and resulted in a 17% increase to 2,804 cases nationwide, from 2,400 cases during January--May 2006. The number of villages with endemic dracunculiasis has decreased in Ghana from 673 in 2004, to 422 in 2005, to 346 in 2006. In 2006, the eradication program retrained village volunteers in patient management, increasing the case-containment rate to 90% during January--February 2007, compared with 60% in 2005 and 75% in 2006. Among villages with endemic dracunculiasis, 95% had cloth water filters in all households in 2006 (compared with 89% in 2005), 47% had at least one source of safe drinking water (39% in 2005), and Abate was used in 27% (56% in 2005) (Table 2). In September 2006, the government of Ghana declared dracunculiasis a national emergency in the country's Northern Region, increased funding for the eradication program by approximately 200%, and began an intensive campaign (e.g., via radio, press, television, and billboard messages) to help mobilize villagers to protect themselves and publicize availability of free medical treatment for all persons with the disease. In 2007, program staff members have increased the frequency of supervisory visits to villages with endemic dracunculiasis and have been conducting daily, house-to-house surveillance for cases. Nigeria. In January 2007, 41 cases of dracunculiasis were caused by infected farmers from a tribal group who had migrated in 2005 from a village where dracunculiasis was known to be endemic to a village where the disease had not been endemic previously. Because the affected community is a remote farming village, the outbreak continued undetected for months until one patient sought medical attention at a public health clinic. Staff members from the Nigerian Guinea Worm Eradication Program canvassed the community and others in the area for active cases of dracunculiasis, initiated measures to contain transmission from every person with an open infection, educated the community and its leaders regarding preventive measures, distributed cloth water filters to all households, applied Abate to all stagnant sources of drinking water, and targeted the community for provision of a borehole well. The community is being monitored daily for additional cases, which are seasonal and most likely to appear during October 2007--February 2008. Certification UpdateIn March 2007, the International Commission for the Certification of Dracunculiasis Eradication met for the sixth time in Geneva, Switzerland, and recommended certifying 12 countries (Afghanistan, Algeria, Cameroon, Central African Republic, Djibouti, Gabon, Liberia, Mozambique, Sierra Leone, Swaziland, Tanzania, and Zambia) as free from transmission of dracunculiasis, bringing the total number of certified countries and territories to 180. Five countries where dracunculiasis was previously endemic are in the precertification stage, and six other countries are awaiting certification. Reported by: DR Hopkins, MD, E Ruiz-Tiben, PhD, The Carter Center, Atlanta, Georgia. ML Eberhard, S Roy, Div of Parasitic Diseases, National Center for Zoonotic, Vector-Borne, and Enteric Diseases, CDC. Editorial Note:Dracunculiasis is a parasitic infection caused by Dracunculus medinensis. Persons become infected by drinking water from stagnant sources (e.g., ponds, open wells, or pools) contaminated by copepods (water fleas) that contain immature forms of the parasite. After 1 year of development within the host's body, adult worms approximately 1 meter (39.4 inches) long emerge through skin lesions, usually on the lower limbs, which frequently develop severe secondary bacterial infections. No effective antiparasitic drug or vaccine for dracunculiasis exists, and infected persons do not become immune to future infections by the parasite. The emergent Guinea worm is removed manually by rolling it on a stick or roll of gauze a few centimeters each day. Disabilities caused by dracunculiasis during the emergence of the worm are related to the invasion of pyogenic organisms that invade the skin lesion and aggravate the pain, swelling, and cellulitis along the worm tract, including abscess formation (6). The average period of incapacitation is 8.5 weeks. Inflammation of the joints can lead to arthritis, synovitis, and muscle and tendon contraction with resultant ankylosis of the limbs (7). The duration of disability often can be reduced through proper care of the patient's wounds. Keeping patients under supervised care while their Guinea worms are extracted manually can prevent further contamination of drinking water. Global eradication of dracunculiasis will mark the first worldwide elimination of a parasitic disease and the first time a disease has been eradicated without benefit of a vaccine. The first target year for eradicating dracunculiasis was 1995, set by African ministers of health in 1988 and confirmed by the World Health Assembly in 1991. That target was not met because of slower than expected mobilization of the 20 countries with endemic disease (8). In 2007, however, all nine remaining countries with endemic dracunculiasis are mobilized, and the global program has received support from the Bill & Melinda Gates Foundation and other donors in recent years. In 2004, ministers of health and the World Health Assembly established a new eradication target date of 2009 (9). The current global eradication strategy, when effectively applied, has demonstrated the ability to stop transmission of dracunculiasis, reducing the number of cases worldwide from an estimated 3.5 million in 1986 (1) to 4,460 in the first 5 months of 2007 (Table 1). The parasite cannot survive more than 2--3 weeks outside a human body (10). When all transmission is interrupted, D. medinensis will be eliminated, and no further control measures will be needed. In 2007, the most important factors to ensure global eradication are strong political will, a sense of urgency among political leaders to stop transmission in the remaining countries with endemic dracunculiasis, and continued support from eradication partners. References
* Dracunculiasis remains endemic in Burkina Faso, Côte d'Ivoire, Ethiopia, Ghana, Mali, Niger, Nigeria, Sudan, and Togo. Four of these countries (Burkina Faso, Côte d'Ivoire, Ethiopia, and Togo) reported no indigenous cases during January--May 2007; however, countries must report no indigenous cases for 3 years and meet other requirements to be certified as free from transmission by the International Commission for the Certification of Dracunculiasis Eradication. † A case of dracunculiasis is contained if all of the following conditions are met: 1) the disease is detected before or within 24 hours of worm emergence; 2) the patient has not entered any water source since the worm emerged; 3) a volunteer has managed the patient properly, by cleaning and bandaging the lesion until the worm is fully removed manually and by providing health education to discourage the patient from contaminating any water source (if two or more emerging worms are present, the case is not contained until the last worm is pulled out); and 4) the containment process, including verification of dracunculiasis, is validated by a supervisor within 7 days of emergence of the worm. § Dracunculiasis can be prevented by 1) filtering drinking water through a finely woven cloth, 2) treating contaminated water with Abate, 3) providing clean water from borehole or hand-dug wells, and 4) directing persons to avoid entering water sources when Guinea worms are emerging from their bodies, to prevent contamination of sources of drinking water (5).
Table 1
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to [email protected].Date last reviewed: 8/16/2007 |
|||||||||
|