|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
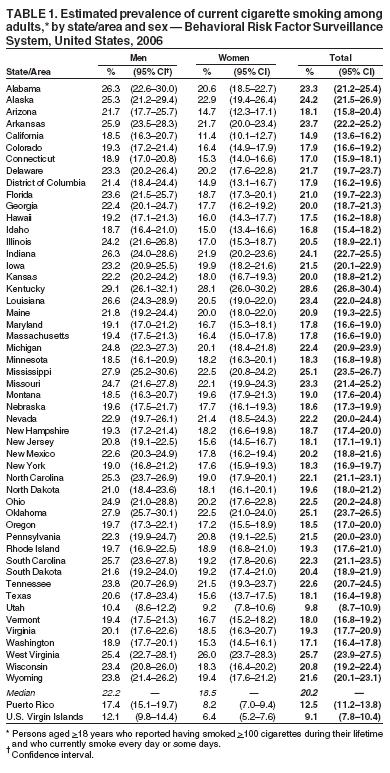
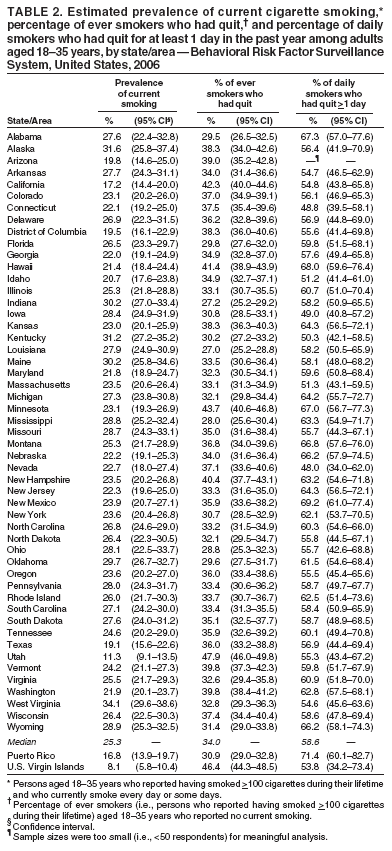
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail. State-Specific Prevalence of Cigarette Smoking Among Adults and Quitting Among Persons Aged 18--35 Years --- United States, 2006Each year, cigarette smoking in the United States causes approximately 438,000 deaths and results in an estimated $167 billion in health-care costs plus lost productivity attributed to premature deaths (1). Although smoking cessation has major and immediate health benefits for persons of all ages (2), the benefit is greater the earlier in life a person quits. Persons who quit before the age of 35 years have a life expectancy similar to that of those who never smoked (3). To assess the prevalence of current smoking among all adults and among those aged 18--35 years, and to assess the proportion of smokers aged 18--35 years who have quit or attempted to quit, CDC analyzed state and area data from the 2006 Behavioral Risk Factor Surveillance System (BRFSS) survey. This report summarizes the results of that analysis, which indicated substantial variation in current cigarette smoking prevalence among the 50 states, the District of Columbia (DC), Puerto Rico (PR), and the U.S. Virgin Islands (USVI) (range: 9.1%--28.6%). The majority of current smokers aged 18--35 years reported that they had attempted to quit smoking during the past year (median: 58.6%; range: 48.0% [Nevada] to 69.2% [New Mexico]), and the median proportion of ever smokers aged 18--35 years who had quit smoking was 34.0% (range: 27.0% [Louisiana] to 47.9% [Utah]). Effective, comprehensive tobacco-use prevention and control programs should be continued and expanded to further reduce smoking initiation by young persons and to encourage cessation as early in life as possible (4,5). BRFSS is a state-based, random-digit--dialed telephone survey of the noninstitutionalized, U.S. civilian population aged >18 years. Estimates were weighted by age and sex distributions of each state or area population. Because BRFSS data are state-specific, national median prevalences are reported instead of national averages. The median response rate for the 50 states and DC was 51.4% (range: 35.1% [New Jersey] to 66.0% [Nebraska]). Respondents were asked, "Have you smoked at least 100 cigarettes in your entire life?" and "Do you now smoke cigarettes every day, some days, or not at all?" Ever smokers were defined as those who reported having smoked >100 cigarettes during their lifetime. Current smokers were defined as those who reported having smoked >100 cigarettes during their lifetime and who currently smoked every day or some days. Former smokers were defined as those who reported having smoked >100 cigarettes during their lifetime and who currently did not smoke at all. Attempted smoking cessation was assessed by asking those who smoked every day, "During the past 12 months, have you stopped smoking for 1 day or longer because you were trying to quit?" The percentage of ever smokers who had quit smoking was calculated by dividing the number of former smokers by the number of ever smokers. Current Cigarette Smoking PrevalenceIn 2006, the median prevalence of current cigarette smoking among adults in the 50 states and DC was 20.2%, with a nearly threefold difference among states with the lowest and highest prevalences (Table 1). Current smoking prevalence was highest in Kentucky (28.6%), West Virginia (25.7%), Oklahoma (25.1%), and Mississippi (25.1%) and was lowest in Utah (9.8%). Smoking prevalence was 12.5% in PR and 9.1% in USVI. The median smoking prevalence for the 50 states and DC was 22.2% (range: 10.4%--29.1%) for men and 18.5% (range: 9.2%--28.1%) for women. Similar variation among the states also was observed in the prevalence of current smoking among persons aged 18--35 years (median for the 50 states and DC: 25.3% [range: 11.3%--34.1%]) (Table 2). Current smoking prevalence for this age group was 16.8% in PR and 8.1% in USVI. Quitting and Quit Attempts Among Persons Aged 18--35 YearsIn 2006, the median percentage of ever smokers aged 18--35 years who had quit was 34.0% for the 50 states and DC (Table 2). The states with the highest percentages of ever smokers who had quit in this age group were Utah (47.9%) and Minnesota (43.7%). The median prevalence of current daily smokers aged 18--35 years who had quit for at least 1 day during the past year was 58.6% for the 50 states and DC (range: 48.0% [Nevada] to 69.2% [New Mexico]) (Table 2). The proportion of current daily smokers who had quit for at least 1 day during the past year was 71.4% in PR and 53.8% in USVI. Reported by: J Kahende, PhD, A Teplinskaya, MPH, A Malarcher, PhD, C Husten, MD, E Maurice, MS, Office on Smoking and Health, National Center for Chronic Disease Prevention and Health Promotion, CDC. Editorial Note:Substantial variations among states and territories were observed in smoking prevalence among adults overall and smoking prevalence and quitting among adults aged 18--35 years. These variations likely are attributed to differences in the distribution of socioeconomic determinants of smoking (e.g., race/ethnicity, age, and socioeconomic status), cultural norms, and the strength of tobacco-control programs and policies (5). In 2006, Utah and USVI were the only areas to achieve the Healthy People 2010 objective to reduce overall adult smoking prevalence to <12% (objective 27-1a) (6); California achieved this objective among women only. Utah and USVI also were the only areas to achieve this objective among persons aged 18--35 years. The low prevalences in Utah and USVI might be a result of stronger social and cultural norms against tobacco use compared with other parts of the United States. Since 2003, Utah and USVI have met the <12% target for overall adult smoking prevalence, and California, Utah, PR, and USVI have achieved this objective among women since 2004. In 2006, Utah met the <12% target among men, as it had in 2004 but not in 2005. The findings in this report indicate that in the 53 areas surveyed, the majority of current daily smokers aged 18--35 years had tried to quit during the past year. On average, approximately one third of persons aged 18--35 years who had ever smoked reported that they did not currently smoke. The rates differed between adults in the 18--35 years age group and the total adult population (CDC, unpublished data, 2007). Early cessation should be encouraged because persons who quit before the age of 35 years have a life expectancy similar to that of never smokers (3). The longer young adults smoke, the more likely they are to develop adverse health effects that are not reversible. Young adults who smoke include persons who are just beginning to smoke, those who do not smoke daily, persons who are transitioning to daily smoking, and daily smokers who might or might not have tried to quit. Diverse strategies are needed to motivate these different groups to quit smoking, such as conducting sustained mass media campaigns, increasing the price of tobacco products, providing brief counseling by health-care professionals at every clinic visit, reducing out-of-pocket costs of smoking-cessation treatments, and offering telephone quitlines (4). Similar to older adults, young adults usually try to quit on their own (7). Among adolescent and young adult smokers aged 16--24 years who reported ever trying to quit, only 20% reported talking with a nurse, doctor, or dentist for assistance with their quit attempts, and even smaller proportions had used counseling (e.g., individual, group, or telephone counseling) or medications approved by the Food and Drug Administration (7). Therefore, strategies also are needed to increase the use of effective cessation treatments among these smokers. The findings in this report are subject to at least five limitations. First, BRFSS does not survey persons in households without landline telephones or those with wireless-only telephones, populations that might more likely include smokers (8,9). Wireless telephone use is highest among young adults and decreases with age (9). Preliminary findings from the National Health Interview Survey indicate that approximately one in four adults aged 18--24 years and nearly one in three adults aged 25--29 years lived in households with only wireless telephones in 2006 (9). The exclusion of persons with wireless-only telephone service might have led to the underestimation of smoking prevalence, particularly among those aged 18--35 years. Second, estimates for cigarette smoking are based on self-report and are not validated by biochemical tests. However, self-reported data on current smoking status have high validity (8). Third, the median response rate was 51.4% (range: 35.1%--66.0%). Lower response rates indicate a potential for response bias; however, BRFSS estimates for current cigarette smoking are comparable to smoking estimates from other surveys with higher response rates (8). Fourth, the survey did not include information on the length of time between the quit attempt and the interview. Finally, the number of young adults who quit smoking was low; thus, certain estimates derived from state-level data are unstable. Effective interventions have been identified for preventing smoking initiation and increasing cessation rates (4), but they have not been implemented adequately by most states. Fully implementing comprehensive state tobacco-control programs as recommended by CDC (5) would accelerate progress in reducing rates of smoking and other tobacco use. Moreover, because persons who quit smoking before the age of 35 years have a life expectancy similar to that of never smokers (3), these programs should target young adults. References
|
Use of trade names and commercial sources is for identification only and does not imply endorsement by the U.S. Department of
Health and Human Services. |
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices.
**Questions or messages regarding errors in formatting should be addressed to [email protected].Date last reviewed: 9/26/2007
|
|
|||||
|
HOME |
ABOUT MMWR |
MMWR SEARCH |
DOWNLOADS |
RSS
|
CONTACT
|
|||||
|
|
|||||
|