|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
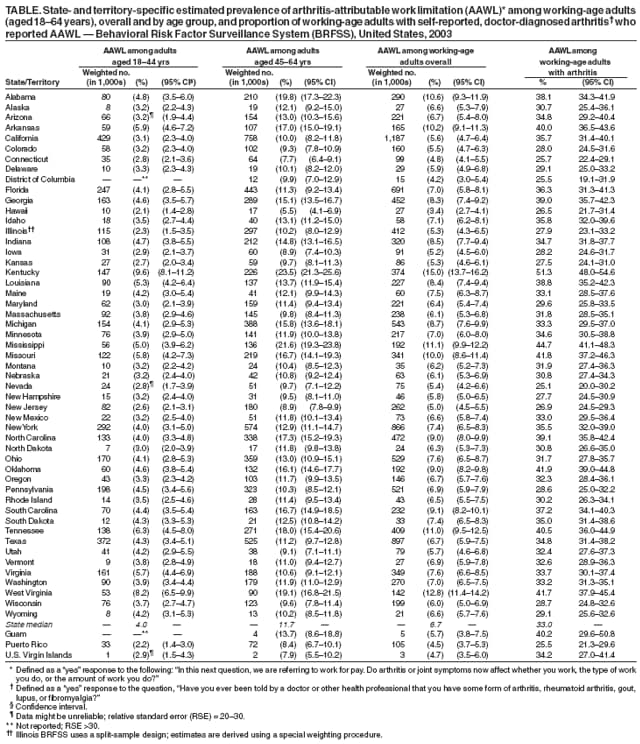
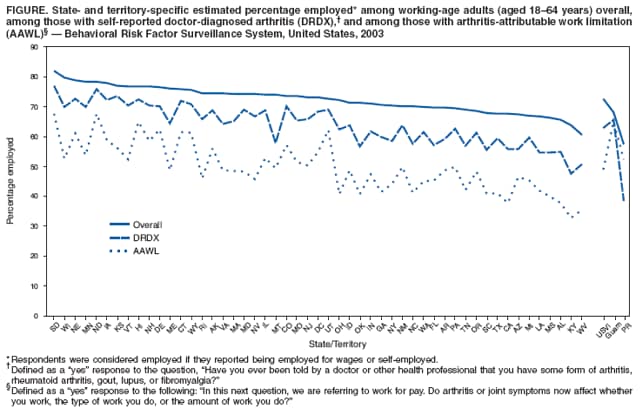
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail. State-Specific Prevalence of Arthritis-Attributable Work Limitation --- United States, 2003One of the Healthy People 2010 objectives calls for a reduction in the proportion of adults with doctor-diagnosed arthritis who are limited in their ability to work for pay because of arthritis (objective 2-5b) (1). Persons who are limited in their work by arthritis are considered to have arthritis-attributable work limitation (AAWL). In the United States, AAWL affects one in 20 working-age adults (aged 18--64 years) and one in three working-age adults with self-reported, doctor-diagnosed arthritis (2). To estimate state-specific prevalence of AAWL and the percentage employed among working-age U.S. adults with AAWL, CDC analyzed data from the 2003 Behavioral Risk Factor Surveillance System (BRFSS) survey. This report describes the results of that analysis, which indicated that the state-specific prevalence of AAWL among all working-age adults ranged from 3.4% (Hawaii) to 15.0% (Kentucky) (median among states: 6.7%) in 2003. Among those with self-reported, doctor-diagnosed arthritis, the prevalence of AAWL ranged from 25.1% (Nevada) to 51.3% (Kentucky) (median among states: 33.0%). In every state, persons with work limitations attributed to arthritis reported being employed less frequently than working-age adults in the state overall and persons with arthritis but not work limitations. Greater use of interventions is needed to help persons with arthritis become and stay employed. The BRFSS survey is a state-based, random-digit--dialed telephone survey of the noninstitutionalized, U.S. civilian population aged >18 years conducted annually in all 50 states, the District of Columbia (DC), Guam, Puerto Rico, and the U.S. Virgin Islands. The 2003 BRFSS survey was the only state-specific survey to assess AAWL among persons with doctor-diagnosed arthritis. Doctor-diagnosed arthritis was defined as a "yes" response to the question, "Have you ever been told by a doctor or other health professional that you have some form of arthritis, rheumatoid arthritis, gout, lupus, or fibromyalgia?" AAWL was defined as a "yes" response to the following: "In this next question, we are referring to work for pay. Do arthritis or joint symptoms now affect whether you work, the type of work you do, or the amount of work you do?" Participants were asked to choose one of the following to determine their employment status: employed for wages, self-employed, out of work for more than 1 year, out of work for less than 1 year, homemaker, student, retired, or unable to work. Respondents were considered employed if they reported being employed for wages or self-employed. Respondents with missing values for doctor-diagnosed arthritis were excluded from the analysis. State-specific prevalence of AAWL was estimated using the population of working-age adults in the state as the denominator. The state population of working-age adults with arthritis was used as the denominator to calculate the proportion of AAWL in this group. The percentage employed* was estimated for three groups in the working-age population: 1) overall, 2) among those reporting doctor-diagnosed arthritis, and 3) among those reporting arthritis and AAWL. Ranges and medians are reported for the 50 states and DC. Weighted point estimates and 95% confidence intervals were derived, accounting for the complex survey design. The Council of American Survey Organizations (CASRO) response rates among the 54 states and territories for the 2003 BRFSS survey ranged from 34.4% (New Jersey) to 80.5% (Puerto Rico) (median: 53.2%), and cooperation rates ranged from 60.1% (California) to 91.9% (Puerto Rico) (median: 74.8%).† In 2003, the state-specific prevalence of AAWL among working-age adults ranged from 3.4% (Hawaii) to 15.0% (Kentucky) (median among states: 6.7%) (Table). In the territories, prevalence of AAWL was 4.5%, 4.7%, and 5.7% for Puerto Rico, the U.S. Virgin Islands, and Guam, respectively. AAWL was higher in all states and territories among adults aged 45--64 years compared with those aged 18--44 years, with the median for the older group (11.7%; range: 5.5% [Hawaii] to 23.5% [Kentucky]) nearly three times that of the younger group (3.9%; range: 2.1% [Hawaii] to 9.6% [Kentucky]). The prevalence of AAWL among adults with doctor-diagnosed arthritis ranged from 25.1% (Nevada) to 51.3% (Kentucky) (median among states: 33.0%). Age adjustment resulted in nearly identical estimates. Among all 50 states and DC, the median percentage employed was 73.2% (range: 60.6% [West Virginia] to 82.0% [South Dakota]) for the overall working-age population (Figure) but was consistently lower for those with doctor-diagnosed arthritis (median among states: 64.3%; range: 47.6% [Kentucky] to 77.1% [South Dakota]) and lower still among those with AAWL (median among states: 48.7%; range: 32.9% [Kentucky] to 67.7% [South Dakota]). This pattern also was observed among all the territories except Puerto Rico. Age adjustment resulted in similar estimates. Reported by: KA Theis, MPH, JM Hootman, PhD, CG Helmick, MD, L Murphy, PhD, J Bolen, PhD, G Langmaid, Div of Adult and Community Health, National Center for Chronic Disease Prevention and Health Promotion; GC Jones, PhD, Div of Human Development and Disability, National Center on Birth Defects and Developmental Disability, CDC. Editorial Note:This report provides the first state-specific prevalence estimates of AAWL among working-age adults. The findings indicate that, in 2003, AAWL varied by state. A recent study demonstrated that, in 2003, the economic costs of low employment among those with arthritis were substantial, with estimated state-specific earnings losses attributed to arthritis and other rheumatic conditions ranging from approximately $79 million (DC) to $4,273 million (California) (3). Both the number of persons affected by arthritis and the prevalence of arthritis are projected to increase (4). Assuming that the 2003 proportion of AAWL among adults with arthritis remains stable, the number of persons experiencing AAWL and its associated consequences will increase. The findings in this report are subject to at least five limitations. First, doctor-diagnosed arthritis was self-reported (i.e., not confirmed by a health-care provider); however, this measure has been validated for surveillance purposes (5). Second, the AAWL question encompassed three work factors (i.e., whether persons are able to work, the type of work they do, and the amount of work they do); the analysis could not examine the independent associations of AAWL and each work factor. Third, work-limiting factors other than AAWL might have contributed to the lower percentage employed among working-age adults with AAWL; however, at least some of the consistently lower employment prevalence among those with AAWL likely is the result of arthritis. Fourth, BRFSS excludes certain populations, including those in the military, residing in institutions, and without landline telephones. Finally, BRFSS has a low median response rate; however, BRFSS weighting procedures partially correct for nonresponse. The effect of low response rates is uncertain. Arthritis is common, affecting nearly 46 million adults nationally, and is associated with numerous functional and activity limitations (4). Physical impairments, such as pain and activity limitations, might underlie AAWL by interfering with the ability of a person to perform work-related tasks and therefore constitute substantial disability. These state-level data on disability attributed to AAWL are critical for program planning and policy development at the local level. Several interventions have the potential to decrease the impact of arthritis on work. First, CDC funds 36 state health departments to expand the reach of evidence-based programs and interventions§ for persons with arthritis. Although the content of these programs is not work-specific, they have been demonstrated to be effective in reducing physical and functional limitations, decreasing pain, and delaying disability attributed to arthritis (6), which might contribute to AAWL. Also, because these programs are designed for community-based implementation, they are feasible for worksite health-promotion programs. Second, federal/state partnership programs to increase employment among persons with disabilities exist in every state, including vocational rehabilitation.¶ A recent randomized controlled trial demonstrated that vocational rehabilitation delivered to employed persons at risk for job loss because of arthritis can decrease or delay job loss (7). The U.S. Social Security Administration's Ticket to Work Program, a nationwide employment program aimed at providing services for persons with various impairments, is another option for eligible persons.** Finally, reasonable worksite accommodations can help keep persons with arthritis and AAWL employed and independent. The Job Accommodation Network, a service of the U.S. Department of Labor's Office of Disability Employment Policy, offers examples of such accommodations for workers with arthritis (e.g., ergonomic work stations and accessible parking) (8). An increasing proportion of U.S. adults are remaining in the workforce after age 64 years (9). At the same time, the number of persons affected by arthritis and its consequences, including activity limitations, are projected to increase with the aging of the U.S. population (4), suggesting a corresponding increase in AAWL and effects on employment. State-based estimates of arthritis impact, such as AAWL, help define the consequences of arthritis, raise awareness, and provide state programs and policy-makers with data for planning. Anticipating and accommodating employment barriers caused by arthritis can prevent disability and maintain a healthy workforce. Acknowledgment The findings in this report for the state of Illinois were provided by B. Steiner, state BRFSS coordinator, Center for Health Statistics, Illinois Dept of Public Health. References
* The measure "percentage employed" is distinct from "employment rate" as defined by the Bureau of Labor Statistics (definition available at http://www.bls.gov/bls/glossary.htm), which calculates employment and unemployment among those who "have made specific efforts to find employment." No data on efforts to find employment are available through the BRFSS survey. † Additional information available at http://www.cdc.gov/brfss/technical_infodata/pdf/2003summarydataqualityreport.pdf. § Including the Arthritis Foundation Exercise Program, Arthritis Foundation Aquatics Program, Arthritis Foundation Self-Help Course, the Chronic Disease Self-Management Program, and EnhanceFitness®. Additional information available at http://www.cdc.gov/arthritis/intervention/index.htm. ¶ Additional information available at http://www.jan.wvu.edu/sbses/vocrehab.htm. ** Additional information available at http://www.yourtickettowork.com/index.
Table
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to [email protected].Date last reviewed: 10/11/2007 |
|||||||||
|