|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
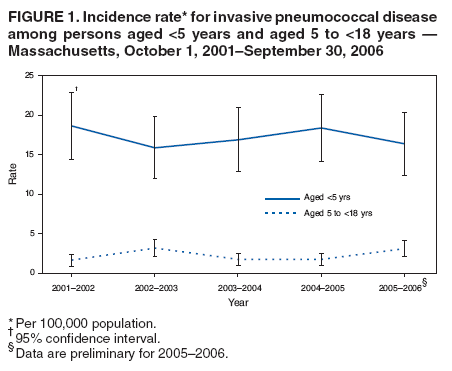
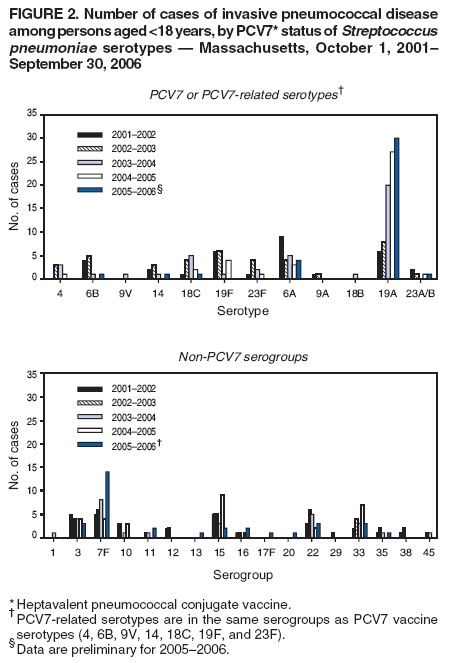
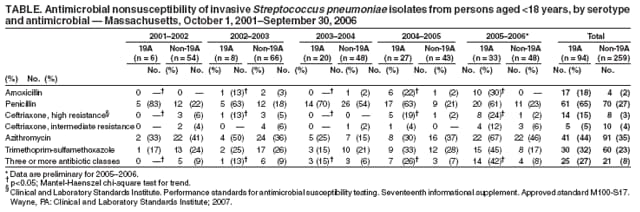
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail. Emergence of Antimicrobial-Resistant Serotype 19A Streptococcus pneumoniae --- Massachusetts, 2001--2006Streptococcus pneumoniae (pneumococcus) is a leading cause of otitis, sinusitis, pneumonia, and meningitis worldwide. Treatment of the most serious type of pneumococcal infection, invasive pneumococcal disease (IPD),* is complicated by antimicrobial resistance. Widespread introduction in 2000 of heptavalent pneumococcal conjugate vaccine (PCV7) against serotypes 4, 6B, 9V, 14, 18C, 19F, and 23F resulted in a decline in antimicrobial-nonsusceptible IPD in the United States (1,2), including in Massachusetts (3). However, development of antimicrobial resistance in serotypes not covered by PCV7 is a growing concern (1,4). In Massachusetts during 2001--2006, IPD surveillance identified an increased number of cases in children caused by pneumococcal serotypes (most notably 19A) not covered by PCV7 and an associated increase in antimicrobial resistance among these isolates. This report examines these trends and clinical characteristics of Massachusetts patients with antimicrobial-nonsusceptible, non--PCV7-type IPD. The findings indicated that, despite increases in incidence of antimicrobial-nonsusceptible IPD, overall rates of IPD remained stable during 2001--2006. In addition, persons with IPD caused by antimicrobial-nonsusceptible S. pneumoniae had clinical outcomes comparable to persons with IPD caused by antimicrobial-susceptible serotypes. Although PCV7 is effective in preventing IPD, these results confirm that antimicrobial resistance among serotypes not covered by PCV7 remains a concern. On October 1, 2001, the Massachusetts Department of Public Health and the Section of Pediatric Infectious Diseases at Boston University Medical Center initiated statewide laboratory- and population-based surveillance for IPD among children.† For this report, cases of IPD were defined by isolation of pneumococcus from a normally sterile body site (e.g., blood or cerebrospinal, pleural, or joint fluid) in a Massachusetts resident aged <18 years during October 1, 2001--September 30, 2006. Demographic and clinical data were obtained from telephone interviews with primary-care providers or adult caregivers. PCV7 vaccination rates were estimated using CDC's National Immunization Survey.§ Serotyping was performed at Boston University Medical Center, using the Quellung reaction with pneumococcal antisera. Susceptibility to five antimicrobials often used in pediatric patients (i.e., amoxicillin, penicillin, ceftriaxone, azithromycin, and trimethoprim-sulfamethoxazole) was determined by E-test (epsilometer test, an agar diffusion method), and interpretations were based on Clinical and Laboratory Standards Institute 2007 guidelines (5). For each antimicrobial agent tested, isolates with either intermediate-level or high-level antimicrobial resistance were considered nonsusceptible to the antimicrobial agent unless otherwise indicated. Population denominators were obtained from 2000--2005 census figures. Mantel-Haenszel chi-square test for trend was used to identify changes in serotype distribution or antimicrobial resistance over time. Chi-square or Fisher's exact tests of proportions were used to compare risk factors and clinical characteristics of disease. Because IPD surveillance did not begin until after introduction of PCV7, no data on pre-PCV7 susceptibility were available for comparison. PCV7 was administered widely to Massachusetts children beginning in 2000. Although PCV7 shortages occurred nationwide, shortages were moderate in Massachusetts. By 2005, approximately 95% of Massachusetts children aged 19--35 months had received >3 PCV7 doses. During October 2001--September 2006, surveillance identified 467 cases of IPD in Massachusetts residents aged <18 years. Throughout this period, annual IPD incidence rates were stable, ranging from 15.9 to 18.6 per 100,000 children aged <5 years (Figure 1); rates were approximately 70% lower than the pre-PCV7 annual IPD incidence of 56.9 per 100,000 children aged <5 years documented in surveillance during 1990--1991 (6). A total of 353 isolates (76%) from 467 cases were available for serotyping. During 2001--2006, a total of 94 (27%) isolates were serotype 19A. During that period, the number and percentage of IPD cases caused by serotype 19A increased from six (10% of all cases) during 2001-- 2002 to 33 (41%) during 2005--2006 (p<0.01) (Figure 2). No significant changes were noted in the proportions of IPD caused by other PCV7 or PCV7-related serotypes or by non-PCV7 serogroups (Figure 2). Because 19A was the most common serotype isolated during 2005--2006, the antimicrobial susceptibility of 19A isolates was examined further (Table). The majority of 19A isolates were nonsusceptible to penicillin. During 2001--2006, significant increases were noted in the proportion of 19A isolates that were nonsusceptible to amoxicillin (minimum inhibitory concentration [MIC] >2 µg/mL), ceftriaxone (MIC >0.5 µg/mL), or three or more classes of antimicrobials (Table). Fourteen (15%) of 94 isolates of 19A were highly resistant to ceftriaxone (MIC >2 µg/ml), a first-line antimicrobial used for empiric bacterial meningitis treatment. No significant trends in the antimicrobial resistance of non-19A isolates were noted. To describe the clinical features of and identify risk factors for infection with ceftriaxone-nonsusceptible serotype 19A, demographic and clinical characteristics of the 14 patients with highly ceftriaxone-resistant 19A IPD were compared with those of 73 patients with ceftriaxone-susceptible 19A IPD and 237 patients with ceftriaxone-susceptible non-19A IPD. The results indicated that patients with highly ceftriaxone-resistant 19A disease did not differ from the other groups with regard to established risk factors for antimicrobial-nonsusceptible pneumococcal disease, including age, sex, race/ethnicity, geographic region, degree of household crowding, or day care exposure. Underlying medical conditions that might predispose to IPD (e.g., sickle cell disease or congenital or acquired immune deficiencies) were not significantly more common among patients with highly ceftriaxone-resistant 19A IPD (three of 14 [21%]) than among patients in the ceftriaxone-susceptible 19A group (nine of 73 [12%]) or the non-19A group (33 of 237 [14%]). In addition, no significant differences among the three groups were detected in the proportion of patients with meningitis, pneumonia, or bacteremia without focus, case-fatality ratios, rates of hospitalization (79% versus 68% and 59%, respectively), or longer hospital stay (64% with >4 days versus 40% and 51%, respectively). Reported by: KK Hsu, MD, JE Kellenberg, MPH, SI Pelton, MD, Boston Univ Medical Center; DS Friedman, PhD, Massachusetts Dept of Public Health. MR Moore, MD, Div of Bacterial Diseases, National Center for Immunization and Respiratory Diseases; HT Jordan, MD, EIS Officer, CDC. Editorial Note:During 2001--2006, Massachusetts surveillance identified an increase in the proportion of childhood IPD cases caused by serotype 19A and increasing resistance of 19A isolates to commonly used antimicrobials. Increases in the proportion of IPD caused by pneumococcal serotypes not covered by PCV7 have been reported previously (1,4,7,8). In Massachusetts and in other states, serotype 19A has emerged as the most common cause of IPD, and the proportion of 19A isolates that are nonsusceptible to commonly used antimicrobials is greater than the proportion for other serotypes (1,4). As a member of the same serogroup as the PCV7-type 19F, serotype 19A is considered a PCV7-related serotype. However, PCV7-induced antibodies to 19F are not active against serotype 19A (9). Concern exists that emergence of antimicrobial-nonsusceptible non--PCV7-type IPD could erode the success of PCV7 against pneumococcal infections. The limited number of 19A cases restricted the ability of this study to identify risk factors or characteristic clinical features of antimicrobial-nonsusceptible 19A disease. However, the study found no evidence that infections caused by antimicrobial-nonsusceptible serotype 19A had different clinical syndromes or outcomes than infections caused by antimicrobial-susceptible 19A. Despite the lack of continuous surveillance data before PCV7 introduction, the overall stability of IPD incidence in Massachusetts during the study period indicates that the decline in IPD resulting from PCV7 introduction is being maintained (3,6). Furthermore, antimicrobial-nonsusceptible infections have not negated the positive impact of PCV7. Accordingly, vaccination with PCV7 remains a priority in Massachusetts. Nonetheless, the emergence of antimicrobial-nonsusceptible non--PCV7-type IPD is of concern. Continued surveillance for IPD in Massachusetts will provide data on the clinical impact of antimicrobial-nonsusceptible 19A infection and will be useful in development and monitoring of new pneumococcal vaccines. The findings in this report support the continued empiric use of combination therapy with vancomycin and cefotaxime or ceftriaxone (the antimicrobials of choice to treat nonsusceptible pneumococci) for children with bacterial meningitis caused by, or possibly caused by, S. pneumoniae, and for critically ill children with nonmeningeal IPD (10). Antimicrobial-resistance data obtained through surveillance will continue to guide empiric treatment regimens for IPD in Massachusetts and provide data that can be used to tailor treatment recommendations to state-specific resistance patterns. State-based surveillance also will help detect trends in the emergence of nonsusceptible non-PCV7 IPD. The recent development of polymerase chain reaction (PCR)-based serotyping provides the opportunity for state public health laboratories and academic partners to identify IPD isolates by serotype. Serotyping based on the Quellung reaction requires expensive reagents and substantial training and experience to perform reliably. In contrast, PCR-based serotyping can be performed using commercially available reagents and equipment and technical expertise already available in most state public health laboratories.¶ If applied in other states, these techniques might increase understanding of IPD trends that have occurred nationally since introduction of PCV7. Acknowledgments This report is based, in part, on contributions by SM Lett, MD, A DeMaria, Jr, MD, Massachusetts Dept of Public Health; H Huot, J Wesson, S Karumuri, L Truong, B Ma, Boston Univ Medical Center; and BE Mahon MD, Boston Univ School of Public Health. References
* IPD is defined by isolation of S. pneumoniae from a normally sterile body site (e.g., blood or cerebrospinal, pleural, or joint fluid). † Partial support for the IPD surveillance was provided by Wyeth as part of the investigator-initiated proposal. § Information available at http://www.cdc.gov/vaccines/stats-surv/imz-coverage.htm#nis. ¶ Information available at http://www.cdc.gov/ncidod/biotech/strep/prc.htm.
Figure 1
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to [email protected].Date last reviewed: 10/18/2007 |
|||||||||
|