|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
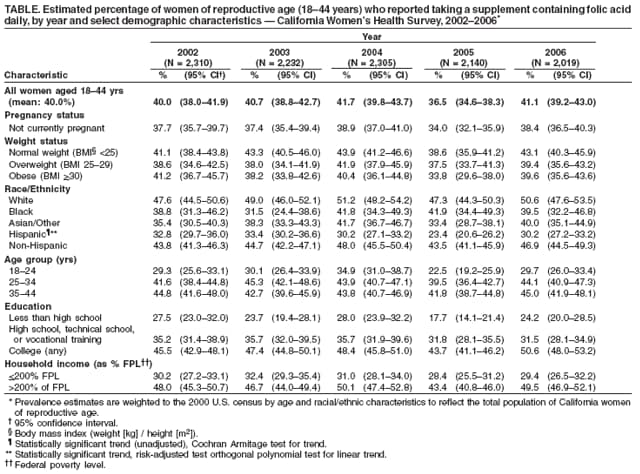
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail. Trends in Folic Acid Supplement Intake Among Women of Reproductive Age --- California, 2002--2006Daily intake of 400 µg of folic acid before conception can reduce by approximately 80% the risk for having an infant with a neural tube defect (NTD) such as spina bifida or anencephaly (1). Although other risk factors for NTDs exist, such as diabetes, obesity, and family history of NTDs, prevention measures have focused predominantly on promoting folic acid consumption. Women can ensure they are consuming the recommended amount of folic acid by eating one serving of breakfast cereal fortified with 100% of the recommended daily value of folic acid or by taking a supplement with 400 µg folic acid daily (2). Annual surveys conducted for the March of Dimes (MOD) Birth Defects Foundation indicate that 40% of all U.S. women of reproductive age (i.e., aged 15--45 years) took supplements containing folic acid in 2007 (MOD, unpublished data, 2007), up from 28% in 1995 (3). To analyze trends in folic acid--containing supplement intake among California women aged 18--44 years during 2002--2006, the California Department of Public Health conducted trend analyses of data from the California Women's Health Survey (CWHS). This report summarizes the results of those analyses, which indicated that although the overall prevalence of intake of folic acid--containing supplements remained stable from 2002 (40%) to 2006 (41%) in California, use of such supplements decreased among Hispanic women and women with less education. Downward trends among Hispanic women are of particular concern because 1) Hispanic women are at increased risk for having a fetus or an infant with an NTD compared with women of other races/ethnicities (4,5), 2) the number of births to Hispanics in California increased during 1993--2003 (6), and 3) Hispanics accounted for nearly 52% of all births in California in 2005 (California Department of Public Health, unpublished data, 2005). Development of additional targeted and evidence-based public health interventions for increasing folic acid intake among these populations is needed. CWHS is a statewide, random-digit--dialed telephone survey of women aged >18 years. Data from approximately 4,000 interviews are collected annually, half of which are from respondents aged 18--44 years. Survey cooperation rates (the proportion of eligible households contacted that resulted in a completed interview) for 2002--2006 ranged from 72% to 74%; Council of American Survey Research Organizations (CASRO) response rates ranged from 37% to 42%. The survey is conducted in English and Spanish and contains questions on various women's health topics (e.g., domestic violence, mammography use, body mass index, and physical activity). Questions on the daily use of supplements containing folic acid were first included in the 2002 survey. In each year since 2002, respondents have been asked, "Are you currently taking a prenatal or multivitamin pill or a pill containing the B vitamin folate or folic acid?" and "Do you take any of these on a daily basis?" Respondents who answered yes to both questions were identified as persons who used folic acid daily. Data were stratified by pregnancy status, race/ethnicity, age, educational attainment, and income. Income was measured as the percentage of household income above or below the federal poverty level in a given year. Prevalence estimates, temporal trends, and risk-adjusted linear trends for daily folic acid intake among respondents aged 18--44 years were examined for each year from 2002 to 2006. Using the 2000 U.S. census, all results were weighted by age and race/ethnicity to reflect the total population of women aged 18--44 years in California and to allow for comparisons of survey years. The Cochran Armitage test for trend was used to determine significance in unadjusted models, and the orthogonal polynomial test for linear trend in logistic regression was used in risk-adjusted models. The overall prevalence of daily intake of supplements containing folic acid among California women aged 18--44 years did not change significantly from 2002 (40.0%) to 2006 (41.1%), although a decrease occurred in 2005 (36.5%) (2002 versus 2005, p=0.01; 2003 versus 2005, p=0.002; 2004 versus 2005, p<0.001, by chi-square test) (Table). Among Hispanic women, the prevalence of daily intake of supplements containing folic acid declined significantly from 32.8% in 2002 to 30.2% in 2006 (p=0.002, Cochran Armitage two-tailed test for trend). This decrease also was significant in risk-adjusted models controlling for the effects of 1) age and income and 2) age and educational attainment (p<0.001 for both). Reported by: AM Herrndorf, MPH, SC Haydu, MPH, ER Takahashi, PhD, Maternal, Child, and Adolescent Health Program, California Dept of Public Health. Editorial Note:To reduce the risk for NTDs, the Institute of Medicine (IOM) recommends that all women of reproductive age consume at least 400 µg of synthetic folic acid daily through dietary supplements, fortified foods, or a combination of the two. In addition, IOM recommends that women eat foods rich in naturally occurring folate from a varied diet* (7). These recommendations are for all women of reproductive age because 50% of U.S. pregnancies are unplanned (8). Since the mid-1990s, the California Department of Health Services (CDHS)† has partnered with the California MOD to promote folic acid intake by women of reproductive age and participated in the National Folic Acid campaign that occurred during 1999--2001. In 2002, folic acid pamphlets and posters in English and Spanish were revised by CDHS to focus on two options for obtaining 400 µg of folic acid daily: fortified cereals or vitamin supplements. CDHS and MOD have developed and distributed folic acid education guidelines and materials, including a booklet given to couples who are obtaining a marriage license. During 2000--2004, the California Folic Acid Council developed targeted interventions, including informational slides in English and Spanish that were shown in movie theaters. Although folic acid supplements have been available as a benefit of Medi-Cal (California's Medicaid program) for decades, use of 400-µg folic acid supplements among nonpregnant women of reproductive age has been considerably lower than anticipated (Medi-Cal, unpublished data, 2006--2007). Data from the 2001--2002 National Health and Nutrition Examination Survey indicate that only 8% of nonpregnant women aged 15--49 years consumed >400 µg folic acid by eating fortified foods, suggesting that more women need to take a supplement containing folic acid to achieve recommended intake levels (9). Since 1995, the Gallup Organization, commissioned by MOD, has conducted surveillance on self-reported intake of folic acid supplements among U.S. women of reproductive age. Findings from the MOD survey indicate that the proportion of U.S. women who use supplements containing folic acid increased from 28% in 1995 to 40% in 2007 (MOD, unpublished data, 2007). The estimated use of daily supplements containing folic acid might be slightly higher in California than in the United States overall, with approximately 37% of California women reporting intake of supplements containing folic acid in 2005 compared with 33% of women nationally.§ According to these estimates, California and all other states likely are far from meeting the Healthy People 2010 objective for folic acid intake (objective 16-16a), which is to increase to 80% the proportion of all nonpregnant women aged 15--44 years who consume at least 400 µg of folic acid daily. Hispanic respondents to CWHS were less likely than respondents of other racial/ethnic groups to report daily use of supplements containing folic acid. The decline in daily supplement use likely indicates a lower total intake of folic acid among Hispanic women and is of particular concern because NTD rates are nearly two times higher among Hispanic women (0.60 per 1,000 live births during 1999--2003) than among white women (0.36 per 1,000 live births) in California (5). The findings in this report are subject to at least three limitations. First, although the sample size was large, cell sizes were not adequate to include all relevant covariates in the risk-adjusted trend models. Second, the weighting methodology used in CWHS adjusts for age and racial/ethnic discrepancies between the CWHS sample and California's general population but does not adjust for education or income discrepancies. Because U.S. women with higher levels of education are more likely to report vitamin use (3), and overall, respondents to CWHS have higher levels of education than California's general population, the results of this study might overestimate folic acid supplement use among California women. Third, CWHS data on folic acid use are derived from self-reported supplement use; questions regarding additional sources of folic acid, such as fortified breakfast cereal or grain products, were not included in CWHS, which might have resulted in an underestimation of the number of women consuming folic acid. Educational materials and provider guidelines on folic acid use have been widely distributed to women participating in CDHS programs and receiving CDHS services. However, not all California women of reproductive age have benefited from or participated in these programs. Evidence-based strategies such as social marketing (10) and providing better access to supplements containing folic acid might be needed, especially among certain subgroups of women (e.g., those with less education and Hispanic women). To reduce disparities in NTD rates between Hispanics and non-Hispanics, Hispanic women of reproductive age should consume 400 µg of folic acid daily through fully fortified sources: either breakfast cereal or vitamin supplements. Supporting evidence-based behavior-change initiatives, such as social marketing campaigns, is an important step toward ensuring that all women of childbearing age consume 400 µg of folic acid every day to prevent serious birth defects. Acknowledgments This report is based, in part, on contributions by the Survey Research Group (Sacramento, California), which administers the California Women's Health Survey; A Ratnasiri, MSc, JL Troyan, MPH, KC Ramstrom, DO, L Llewelyn, MPP, Maternal, Child, and Adolescent Health Program, California Dept of Public Health; and CE Prue, PhD, and J Mulinare, MD, Div of Birth Defects and Developmental Disabilities, National Center on Birth Defects and Developmental Disabilities, CDC. References
* A well-balanced, varied diet includes foods naturally rich in folate, such as orange juice, strawberries, cantaloupe, asparagus, broccoli, cooked dry peas and beans, and dark green, leafy vegetables. † On July 1, 2007, CDHS was divided into the California Department of Public Health and the California Department of Health Care Services. § The MOD-commissioned Gallup Survey asks women of reproductive age "Do you currently take any vitamin or mineral supplement on a daily basis?" and "What type of vitamin or mineral supplement do you take?" The survey questions are similar to, but not the same as, those asked in CWHS. Response rates from the MOD Gallup Survey range from 24% to 53%.
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to [email protected].Date last reviewed: 10/25/2007 |
|||||||||
|