|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
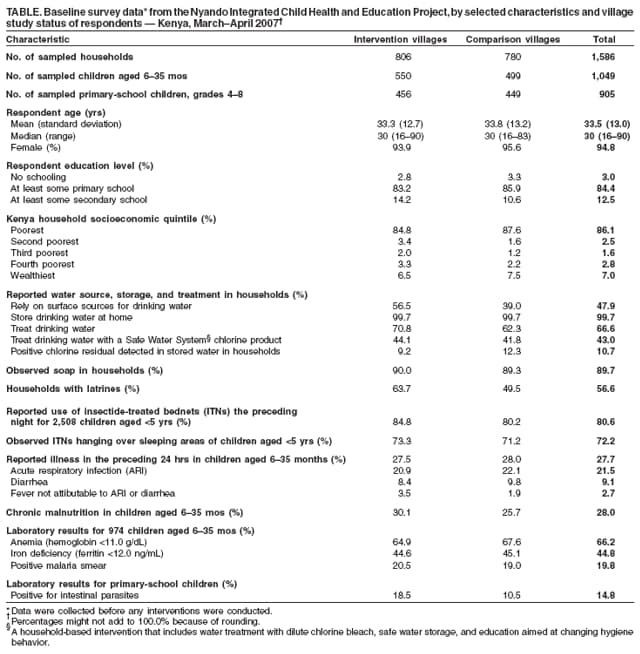
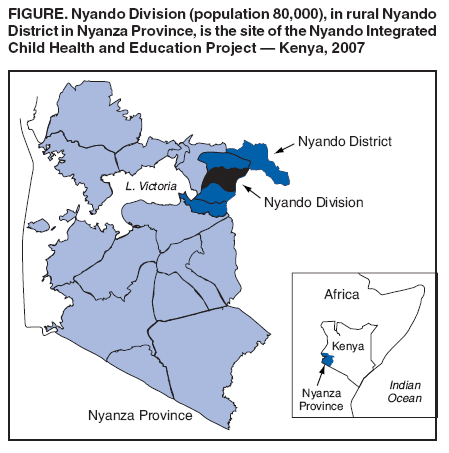
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail. Baseline Data from the Nyando Integrated Child Health and Education Project --- Kenya, 2007This report is presented in conjunction with the Council of Science Editors 2007 Global Theme Issue on Poverty and Human Development, an international collaboration of 235 publications, all releasing reports on poverty and human development on October 22, 2007. Additional information is available at http://www.councilscienceeditors.org/globalthemeissue.cfm. On October 22, this report was posted as an MMWR Early Release on the MMWR website (http://www.cdc.gov/mmwr). Approximately 10 million children aged <5 years die each year in developing countries (1). The leading infectious causes of these deaths include acute respiratory infections, diarrhea, measles, and malaria; malnutrition contributes to approximately 50% of these deaths (2). To address multiple conditions that contribute to mortality, child-survival programs require effective interventions and implementation strategies (3). To assess the effectiveness of multiple interventions, CDC has joined with partners to create the Nyando Integrated Child Health and Education (NICHE) project to combine several proven approaches to child survival in an impoverished rural district of western Kenya. During March--April 2007, CDC began the NICHE project with a baseline survey. This report summarizes preliminary data from that survey, which determined that 1) 86.1% of surveyed households were in the poorest Kenya socioeconomic quintile and 2) among children aged 6--35 months, 21.5% had experienced an acute respiratory infection and 9.1% had experienced diarrhea in the preceding 24 hours, 28.0% had chronic malnutrition, 66.2% had anemia, and 19.8% had a positive malaria smear. Comprehensive interventions will be needed to improve living conditions and reduce the risk for death before age 5 years among children in this population. NICHE Project MethodologyIn the NICHE project, two groups of villages, an intervention group and a comparison group, were selected to compare the effects of child-survival interventions targeted at leading causes of mortality (i.e., respiratory infections, diarrhea, and malaria). Intervention activities were begun initially in the intervention group, and will be expanded to include the comparison group in 2008. A two-stage, modified cluster-sampling strategy was used to select 30 intervention villages and 30 comparison villages from Nyando Division (population 80,000), an impoverished area with poor sanitary facilities located in Nyanza Province in rural western Kenya (Figure). The two clusters of villages were chosen from separate political jurisdictions (i.e., sublocations) to inhibit interventions in one cluster from influencing conditions in the other. Households and children were numbered in each village. Random samples of children aged 6--35 months, and primary-school children (from grades 4--8; generally aged 9--13 years) in the villages were selected by using random number tables. During March--April 2007, a baseline survey was conducted in enrolled households in all 60 villages to determine the 1) demographic, socioeconomic, and health characteristics and 2) health behaviors of the two populations. Information was collected regarding household drinking water, sanitation, hygiene, dietary practices, and child health. A principal component analysis developed by the World Bank was used to categorize the study households into Kenya socioeconomic quintiles (4). NICHE project field workers tested water stored in households for the presence of water chlorination products. Laboratory technicians obtained blood samples from children aged 6--35 months to measure hemoglobin, iron stores, and malaria status. Field workers measured heights and weights of these children, and z-scores were calculated to assess nutritional status; stool samples were collected from primary-school children to test for intestinal parasites. Baseline Survey ResultsThe baseline survey collected data on samples of 1,049 children aged <3 years and 905 primary-school children from 1,586 sampled households (Table); 86.1% of households were in the poorest Kenya socioeconomic quintile, and 94.8% of respondents were women. Respondent ages ranged from 16 to 90 years (median: 30 years), and 84.4% had a primary-school education or less. Among households, 47.9% relied on surface sources (e.g., rivers or ponds) for drinking water, and 99.7% of respondents reported storing drinking water in the home. Respondents in 66.6% of households reported treating their drinking water, and 43.0% reported treating water with a Safe Water System (SWS)*chlorine product; however, investigators detected chlorine residuals in 10.7% of stored water samples. Among households, 89.7% were observed to have soap present, and 56.6% had a latrine. Respondents reported that 80.6% of 2,508 children aged <5 years had slept under an insecticide-treated bednet (ITN) the preceding night; ITNs were observed hanging over the sleeping areas of 72.2% of children aged <5 years. The prevalence of chronic malnutrition† in children aged 6--35 months was 28.0%. Of 974 children aged 6--35 months who were tested, 66.2% were anemic (hemoglobin <11.0 g/dL), and 44.8% were iron deficient (ferritin <12.0 ng/mL); 19.8% had a positive malaria smear. Stool samples from 14.8% of primary-school children exhibited parasites (e.g., schistosomes, trichuris, ascaris, and hookworms). Baseline survey data indicated that 27.7% of children aged 6--35 months were reported to have been ill in the preceding 24 hours; 21.5% had acute respiratory infection, and 9.1% had diarrhea. Fewer than 1% had been hospitalized. NICHE ImplementationImplementation activities began in the 30 intervention villages after baseline data collection was completed in April 2007 and will continue through October 2007. Interventions include 1) SWS (5); 2) distribution of ITNs (6); 3) promotion of handwashing with soap (7); 4) distribution of Sprinkles®, single-serve packets of dry powder, containing iron and other micronutrients intended for home fortification of foods consumed by young children who are no longer exclusively breastfeeding (8); and 5) deworming of primary-school children (i.e., of geohelminths) with albendazole; this was the only activity that also was extended to children in the 30 comparison villages. To promote these interventions, project partners have combined several approaches. Population Services International, a social-marketing nongovernmental organization, has an ongoing program to promote purchase and use of SWS bleach solution, ITNs, and reproductive-health products through mass media, peer educators, murals, and billboards. The Safe Water and AIDS Project (SWAP) trains HIV self-help groups in rural villages and urban low-income settings to provide health education and sell health products to their neighbors as an income-generating activity. SWAP trains clinic nurses, school teachers, and religious leaders to teach their clients, students, and congregations about these interventions and installs drinking water and handwashing stations in these settings. Finally, NICHE project staff members enlist the support of local political leaders and the ministries of health and education. As of May 30, 2007, primary-school children in all 60 villages had been dewormed with albendazole. In June, active surveillance to collect data on all household members through biweekly visits to all study households was initiated to assess product use and health status. In addition, ongoing qualitative research is being conducted in intervention villages to supplement surveillance data. A follow-up evaluation of the NICHE project is planned in March 2008. In April 2008, project staff members will expand implementation of all interventions to the 30 comparison villages, and active surveillance will resume in enrolled households in all 60 study villages for another year. To motivate village populations to participate more actively in the NICHE project, staff members are analyzing baseline data and will present summary and village-specific findings to each participating village. Study personnel also will analyze surveillance data regarding specific intervention use and health indicators. In November 2007 and again in March 2008, NICHE staff members will present surveillance findings to each participating intervention village so that residents can see how well they are doing in comparison with the entire study population. Reported by: A Obure, MA, C Mbakaya, PhD, S Kariuki, PhD, D Karanja, PhD, Kenya Medical Research Institute. PC Juliao, PhD, RE Quick, MD, K Teates, MPH, Div of Foodborne, Bacterial and Mycotic Diseases; S Montgomery, DVM, W Secor, PhD, L Slutsker, MD, M Hamel, MD; Div of Parasitic Diseases, National Center for Zoonotic, Vector-Borne, and Enteric Diseases; PS Suchdev, MD, L Ruth, MPH, ME Jefferds, PhD, B Woodruff, MD, Div of Nutrition, Physical Activity and Obesity, National Center for Chronic Disease Prevention and Health Promotion; CDC. Editorial Note:The families in the NICHE project face problems associated with poverty that are common in the developing world. The majority of respondents in the 60 villages are poor; 86.1% fall into the poorest socioeconomic quintile in a country that ranked 152nd out of 177 countries in the 2006 United Nation's Human Development Index.§ These families have poor access to basic sanitary facilities, and young children have high rates of acute respiratory infection, diarrhea, and malaria, compared with populations in more developed countries. High rates of chronic malnutrition are of particular concern, because malnutrition contributes to approximately half the deaths in children aged <5 years (2). Previous programs in Kenya aimed at increasing child survival and improving public health in this study population have had some success. Free distribution of ITNs has resulted in high observed baseline use rates, and ongoing promotion of water-treatment products has resulted in reported use of SWS products at baseline by 43.0% of households and confirmed use by 10.7% of households. In recent years, a trend has been observed toward increased funding for high-profile, disease-specific, child-health programs that have had an impact on child survival. Recognition of the need for multiple interventions to address child survival has led to recent initiatives to bundle interventions (9). Greater use of interventions available today might make possible the achievement of the United Nations millennium development goal to reduce child mortality by two thirds by the year 2015 (3). By integrating services, combining interventions, and engaging local leadership, the NICHE project is attempting to create a model for improved child health. The findings in this report are subject to at least three limitations. First, results are specific to the study population and geographic area and are not generalizable to the entire population of Kenya. Second, socioeconomic quintiles for Kenya households were derived from 1998 data; recent changes (e.g., more widespread use of cellular telephones) might affect socioeconomic indicators. Finally, illness data were based on unverified reports; therefore, the 21.5% of children reported with acute respiratory infection and other illness data might be subject to recall bias. The NICHE project will enable CDC and partners to assess the extent to which combining proven child-survival interventions and employing multiple community-based implementation techniques can improve health in impoverished populations. The use of inexpensive, locally available interventions will control program costs and increase the prospects for sustaining the program. If the simultaneous engagement of local populations and institutions, the private sector, and government in program implementation proves successful, this implementation approach might serve as a blueprint for child-survival programs in other regions of Kenya and elsewhere in Africa. Acknowledgments This report is based, in part, on contributions by the Kenya Ministry of Health; Safe Water and AIDS Project; Kenya Medical Research Institute; Sprinkles Global Health Initiative; CDC Coordinating Office of Global Health; Bur of Global Health of the U.S. Agency for International Development; Bur of Oceans, Environment, and Science of the U.S. Dept of State; and A Eleveld, C Jalang'o, V Were, C Ochieng, SH Faith, S Kola, I Sadumah, W Abok, R Otieno, L Ogange, M Owuor, B Ondego, P Odonde, T Malachi, U Mandava, I Parvanta, D Feikin, J Vulule, J Kioko, F Diemo, and R Abayo. References
* A household-based intervention that includes water treatment with dilute chlorine bleach, safe water storage, and education aimed at changing hygiene behavior. † Defined as a z-score of less than -2 for height-for-age, according to the 2005 World Health Organization Child Growth Standards. Available at http://www.who.int/childgrowth/en. § Available at http://hdr.undp.org/hdr2006/statistics. Table
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to [email protected].Date last reviewed: 10/25/2007 |
|||||||||
|