|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
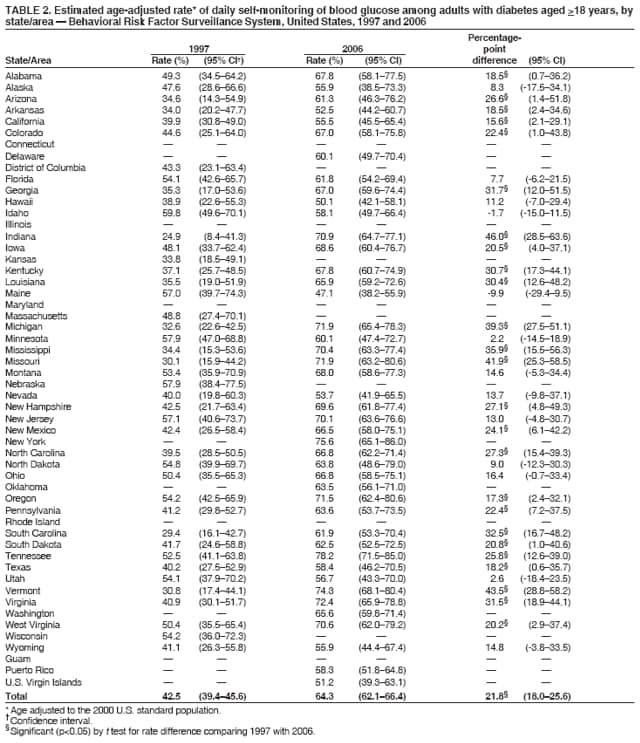
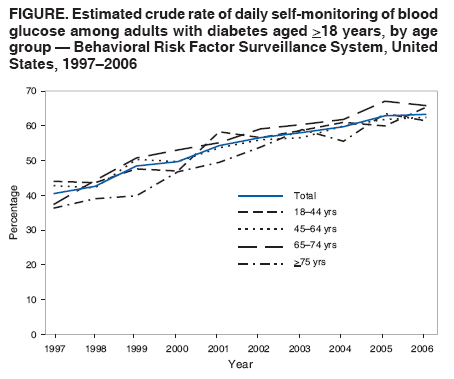
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail. Self-Monitoring of Blood Glucose Among Adults with Diabetes --- United States, 1997--2006Blood-glucose control is critical for managing diabetes and preventing diabetes-related complications such as cardiovascular disease, retinopathy, nephropathy, and neuropathy (1). In addition to recommending that patients with diabetes have a glycated hemoglobin (HbA1c) measurement at least two times a year, the American Diabetes Association recommends self-monitoring of blood glucose (SMBG) as an integral part of diabetes management for patients who are treated with insulin and as a useful component for achieving glycemic goals for patients who use oral medications or medical nutrition therapy (2). One of the Healthy People 2010 national objectives is to increase to 61% the proportion of persons with diabetes who perform SMBG at least once a day (objective 5--17) (3). To estimate the rates of SMBG and to track the progress of states during 1997--2006, CDC analyzed data from the Behavioral Risk Factor Surveillance System (BRFSS) for that period. This report summarizes the findings of that analysis, which indicated that the proportion of adults with diabetes who check their blood glucose at least once a day increased at the national level, and 25 of the 38 states examined had statistically significant rate increases from 1997 to 2006. In 2006, the daily SMBG rate was 63.4% among all adults with diabetes and 86.7% among those treated with insulin. Collaborations to ensure adequate health insurance coverage, diabetes education and counseling to encourage more intensive medical care and self-management practices, and continued surveillance measures to track changes in SMBG rates are needed to improve and monitor SMBG trends. BRFSS is an ongoing state-based, random-digit--dialed telephone survey of the noninstitutionalized, U.S. civilian population aged >18 years; the survey is conducted in all 50 states, the District of Columbia, and three U.S. territories. The survey sample size ranged from 135,582 in 1997 to 356,112 in 2005. The median response rate* among jurisdictions was 62.5% (range: 41.3%--88.9%) in 1997 and 51.4% (range: 35.1%--66.0%) in 2006, based on Council of American Survey and Research Organizations (CASRO) guidelines. The median cooperation rate† was 65.9% (range: 46.8%--90.1%) in 1997 and 74.5% (range: 56.9%--83.5%) in 2006. Persons with diabetes were defined as respondents who answered "yes" to the question, "Have you ever been told by a doctor that you have diabetes?" Women who said they were told that they had diabetes only during pregnancy and respondents who stated they had prediabetes or borderline diabetes were not included. Daily SMBG was determined by response to the question, "About how often do you check your blood for glucose or sugar?" Statistical software was used to analyze data, incorporating the survey sampling design and sampling weights to make results representative of the U.S. population. Linear regression weighting the annual estimates by the inverse of their variances was used to test for 10-year national trends in SMBG. Logistic regression was used to identify factors associated with self-monitoring. A t test was used to compare rate differences between 1997 and 2006 at the state level. Results were considered significant if p<0.05, unless otherwise noted. In 2006, 63.4% (95% confidence interval [CI] = 62.2%--64.7%) of adults with diabetes aged >18 years reported self-monitoring their blood glucose at least once a day (Table 1), exceeding the Healthy People 2010 target of 61%. Among adults treated with insulin, 86.7% (CI = 84.9%--88.4%) checked their blood glucose at least daily. The overall rate of SMBG increased from 40.6% in 1997 to 63.4% in 2006 among adults with diabetes. The modeled average annual increase was 2.5 percentage points (Figure). Rates increased across all age groups examined, from 44.0% to 65.5% (with an annual increase of 2.4 percentage points) among persons aged 18--44 years, from 42.9% to 62.4% (with an annual increase of 2.2 percentage points) among those aged 45--64 years, from 37.3% to 65.9% (with an annual increase of 2.9 percentage points) among those aged 65--74 years, and from 36.4% to 61.5% (with an annual increase of 3.0 percentage points) among those aged >75 years (Figure). During 2006, the state-specific rates of SMBG among adults with diabetes ranged from 47.1% to 78.2% (Table 2). From 1997 to 2006, a total of 25 of the 38 states collecting data in both 1997 and 2006 had significant rate increases, and no state had a significant decrease (Table 2). In multivariate analyses of 2006 data, the following had significant positive associations with daily SMBG: having a high school education compared with having less than a high school education (adjusted odds ratio [AOR] = 1.4); having health insurance coverage (AOR = 1.4); using oral medication only (AOR = 2.7), insulin only (AOR = 11.0), or both insulin and oral medication (AOR = 7.8) compared with not using insulin or oral medication; making doctor visits 1--2 times (AOR = 1.5), 3--4 times (AOR = 2.3), 5--10 times (AOR = 2.1), or >11 times (AOR = 2.6) annually compared with making no visits; and having ever taken a diabetes-education course (AOR = 1.6) (Table 1). In contrast, being male (AOR = 0.7) was associated with decreased odds for daily SMBG. Reported by: L Pan, MD, Q Mukhtar, PhD, LS Geiss, MA, Div of Diabetes Translation, National Center for Chronic Disease Prevention and Health Promotion, CDC. Editorial Note:SMBG allows patients to adjust food intake, physical activity, or pharmacologic therapy in response to their blood-glucose readings and to assess whether their blood-glucose levels are under control (2). In 2006, the national rate of SMBG exceeded the Healthy People 2010 target of 61%. From 1997 to 2006, rates of SMBG increased overall, in all age groups examined, and in the majority of states examined. Health insurance policy changes and improvements in monitoring devices during this period might have influenced the rate increases. The Balanced Budget Act of 1997 provided Medicare coverage for blood-glucose monitors and testing strips for persons with insulin-treated or non--insulin-treated diabetes.§ This change in Medicare coverage and its possible influence on the policies of private insurers might have contributed to the increases in SMBG rates. The improvement in monitoring technology makes the monitoring practice more convenient, which might also contribute to the upward trends. However, considerable variation in SMBG rates was observed among states. States with lower SMBG rates should consider taking additional steps to increase daily SMBG. Unlike previous studies (4,5), multivariate analysis in this study indicated no significant associations between SMBG and age, race/ethnicity, or having at least two HbA1c measurements per year. However, consistent with findings from other studies (4,5), lower rates of SMBG were correlated with being male, having less than a high school education, having no health insurance coverage, taking no medication or oral medication only, making two or fewer doctor visits annually, and not having taken a diabetes-education course. The negative associations between SBMG and lower education or lack of health insurance coverage suggest that socioeconomic barriers might impede the practice of SMBG. The cost of blood glucose--monitoring supplies might be a barrier for patients with limited economic resources (6). Positive associations were observed between SMBG and number of doctor visits, insulin use, or having ever taken a diabetes-education course, which indicates that SMBG might be associated with better disease management or more intensive medical care. The findings in this report are subject to at least five limitations. First, BRFSS data are self-reported and subject to recall bias. Therefore, SMBG rates might be underestimated or overestimated; further investigation of the reliability and validity of self-reported SMBG is needed. Second, BRFSS excludes persons without landline telephones. Adults with only wireless telephones tend to be younger, to have lower incomes, to be Hispanic, and to have no health insurance coverage.¶ As a result, the SMBG rates might be overestimated and might not be generalizable to certain segments of the U.S. population. Third, the median response rate of BRFSS was only 62.5% in 1997 and 51.4% in 2006; however, the potential for bias attributed to selected respondents who refused to be interviewed is low.** Fourth, the states using BRFSS diabetes modules varied from year to year. During the past decade, the number of states collecting data on SMBG ranged from 39 (in 1998 and 1999) to 49 (in 2003), which might have influenced the observed upward trends. However, an average annual increase of 2.3 percentage points was observed in the overall rate, and annual increases of 2.0--2.7 percentage points were observed in age-specific rates when limiting the data analysis to the 25 states reporting data in all years from 1997 to 2006. Finally, a dichotomous variable measuring daily SMBG (i.e., did or did not practice daily) was created for this analysis, which did not allow for analysis of correlation with the intensity of self-monitoring (i.e., once or multiple times per day). Nearly 30% of adults with diabetes are using insulin, either alone or combined with oral medication (7). Although studies on the efficacy of SMBG for patients with type 2 diabetes not treated with insulin remain inconclusive (8,9), SMBG helps persons with type 1 diabetes and insulin-treated type 2 diabetes improve their blood-glucose control (9,10). Given this scientific evidence, intervention strategies to increase SMBG should focus on persons treated with insulin. Access to health care is an important factor associated with SMBG. Health insurance coverage of monitoring devices and supplies is integral in encouraging self-monitoring and self-management practices. Collaborations to ensure adequate insurance coverage for blood-glucose monitors, test strips, and lancets are essential for increasing the rates and benefits of SMBG. Recommendations from health professionals and the provision of diabetes education can influence the self-management practices of patients. Diabetes-education programs might increase the benefits of self-monitoring by teaching patients the optimal timing and frequency of self-monitoring, how to interpret the results correctly, and how to make appropriate diet, exercise, and pharmacologic-therapy adjustments in response to SMBG readings. Continued surveillance will be important for monitoring future trends in SMBG and the effectiveness of intervention strategies. References
* The percentage of persons who completed interviews among all eligible persons, including those who were not successfully contacted. † The percentage of persons who completed interviews among all eligible persons who were contacted. § Additional information available at http://www.cms.hhs.gov/demoprojectsevalrpts/downloads/cc_section4016_bba_1997.pdf. ¶ Additional information available at http://www.cdc.gov/nchs/data/nhis/earlyrelease/wireless200705.pdf. ** Additional information available at http://ftp.cdc.gov/pub/data/brfss/userguide.pdf.
Table 1
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to [email protected].Date last reviewed: 11/1/2007 |
|||||||||
|