|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
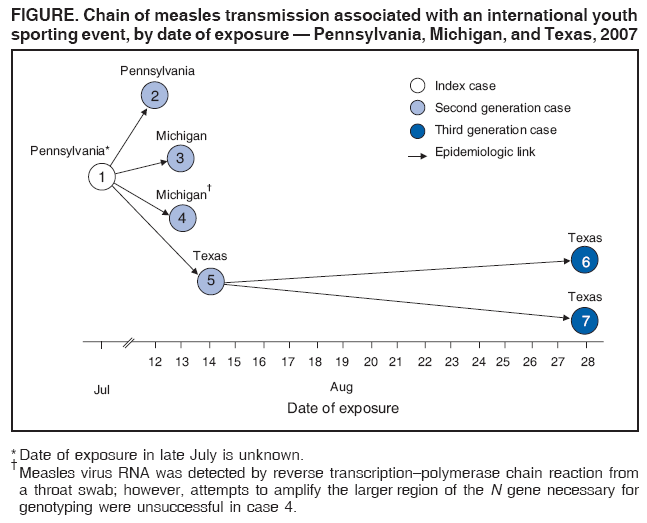
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail. Multistate Measles Outbreak Associated with an International Youth Sporting Event --- Pennsylvania, Michigan, and Texas, August--September 2007Measles, a highly infectious viral illness, is no longer endemic in the United States because of high coverage rates with an effective vaccine (1). However, imported cases continue to cause illness and outbreaks among susceptible U.S. residents (2--5). In August 2007, a participant in an international youth sporting event who traveled from Japan to the United States became ill with measles. Because he traveled while infectious to an event with thousands of participants and spectators, an outbreak investigation was conducted in multiple states by state and local health departments in coordination with CDC, using standard measles surveillance case definitions and classifications.* This report summarizes the results of that investigation, which identified six additional measles cases that were linked epidemiologically to the index case and two generations of secondary transmission. Viral genotyping supported a single chain of transmission; six of the seven cases were linked by genetic sequencing (Figure). U.S. organizers of large-scale events attended by international travelers, especially youths, should consider documentation of adequate participant vaccination. This outbreak highlights the need to maintain the highest possible vaccination coverage in the United States, along with disease surveillance and outbreak-containment capabilities. A sporting event held in central Pennsylvania during August 17--26, 2007, included eight U.S. teams and eight international teams representing Canada, Chinese Taipei, Curaçao, Japan, Netherlands, Mexico, Saudi Arabia, and Venezuela. Combined participant and spectator attendance for the event was approximately 265,000. Team members (boys aged 10--13 years) and coaches resided in the same compound during the event, with a common area shared by all teams. Access to the compound was restricted to a small number of officials, corporate sponsors, and event staff members. Cases 1 and 2: Pennsylvania, Imported from JapanA boy aged 12 years on the Japanese team (the index patient), who had unknown vaccination status, had been exposed to a sibling with measles-like illness in Japan in late July 2007. The boy had a sore throat and malaise on August 11 and traveled to the United States on August 13. The Japanese and Chinese Taipei teams traveled together by aircraft from Tokyo, Japan, to Detroit, Michigan, where they cleared immigration and customs, and then traveled by aircraft to Baltimore, Maryland, where they chartered a bus to Pennsylvania. On August 14, the patient visited the event infirmary to be evaluated for his sore throat. On August 16, he had a measles-compatible rash, cough, Koplik's spots, fever (102.4°F [39.1°C]), and coryza. The infectious period for measles extends from 5 days before to 4 days after rash onset. The Pennsylvania Department of Health (PADOH) was notified, and the patient was isolated. Measles-specific immunoglobulin M (IgM) antibodies were detected in his serum sample; urine culture yielded measles virus, genotype D5. PADOH reviewed vaccination records for 481 players, coaches, translators, and event staff members at the compound; 292 (61%) either had documentation of 2 doses of measles-containing vaccine or history of measles disease, or were born before 1957 and were, therefore, considered immune. The remaining 189 (39%) were offered measles, mumps, and rubella (MMR) vaccine or serologic testing; 104 chose to be vaccinated, and 85 chose serologic testing. Sixteen (19%) of those tested lacked evidence of immunity and subsequently were vaccinated. Public health staff members and health-care providers in Pennsylvania were alerted through the state Health Alert Network, and public announcements were issued. State health departments in California, Georgia, and Texas were informed of potential measles exposures among visiting corporate representatives who had already attended the event and departed from Pennsylvania. A second boy aged 12 years with unknown vaccination status who had direct contact with the index patient only on August 12 in Japan, arrived in the United States on August 15 to watch the competition. On August 20, he had a sore throat and fever, followed by cough and rash on August 23. On August 24, nasopharyngeal, urine, and blood specimens were collected from the boy at a local emergency department. He was placed in isolation in his hotel room. His serum sample was positive for measles-specific IgM antibodies. Nasopharyngeal culture yielded measles virus genotype D5. The boy had minimal public interaction during his infectious period and was deemed not infectious during his airline travel. The 29 members of his travel group and all 27 hotel staff members were interviewed; 38 (68%) persons without adequate evidence of immunity (6) received MMR vaccine. Guests registered at the hotel during the boy's infectious period were advised to contact their physicians and local health departments in the event of illness. No measles cases were identified among these groups. Cases 3 and 4: MichiganIn accordance with CDC protocol (CDC, unpublished document, 2008), passenger manifests for the August 13 Tokyo--Detroit and Detroit--Baltimore flights were obtained to contact persons seated within one row of the index patient. A woman aged 53 years seated one row in front of the index patient on the Detroit--Baltimore flight acquired measles (case 3). Although born in 1954, she recalled no history of measles or receiving measles-containing vaccine and was administered immunoglobulin prophylaxis after being identified as a contact. On August 25, she had fever, cough, and coryza, followed by rash on August 28. Serum initially was negative for measles IgM and immunoglobulin G antibodies, but she subsequently seroconverted. Measles viral RNA, detected in urine by reverse transcription--polymerase chain reaction (RT-PCR), had an identical sequence to the genotype D5 sequences obtained from the two patients in Pennsylvania. Case 4 was identified in a U.S.-born man aged 25 years who was employed as a federal airport officer and had no documented measles vaccination. The officer and the index patient had been present in the same Detroit customs area on August 13. On August 23, the officer had wheezing, abdominal pain, and sweating, followed by rash on August 27. A serum sample obtained August 30 was positive for measles IgM antibodies. Measles virus RNA was detected by RT-PCR from a throat swab; however, attempts to amplify the larger region of the N gene necessary for genotyping were unsuccessful in this case. A coworker of the officer at the same airport had measles 1 month later. The source of this infection could not be determined; the coworker's measles might have been linked to case 4 through an unrecognized chain of transmission (because the incubation period for measles ranges from 7 to 18 days) or might have resulted from a separate, unrelated exposure. Cases 5, 6, and 7: TexasCase 5 was identified in a U.S.-born man aged 40 years who was employed as a corporate sales representative and had no documented measles vaccination. The sales representative had met the index patient on August 14 in Pennsylvania and had cough, conjunctivitis, coryza, and fever on August 26. He had rash on August 28 and was hospitalized the next day with a seizure, fever of 105.7°F (40.9°C), and pneumonia. Measles was confirmed by serum IgM antibodies and viral RNA detected in urine by RT-PCR. He recovered and was discharged from the hospital after 4 days. Before his hospitalization, the man had made sales visits to three Houston-area colleges. Cases 6 and 7 were identified among male college roommates, aged 18 and 19 years, who had attended one of the sales events on August 28. Both students were born in the United States and had received 2 documented doses of MMR vaccine. They had fever, chills, and myalgia on September 9 and 10, respectively; one had conjunctivitis. Both had rash on September 11, detectable measles IgM antibodies in serum, and measles virus RNA by RT-PCR in throat swab specimens. No additional cases were identified. The genotype D5 sequences obtained from the three Texas patients were identical to those of the two patients from Pennsylvania and to one of the two patients (case 3) from Michigan. On August 30, the outbreak was reported to the World Health Organization under the revised International Health Regulations† as a public health emergency of international concern. Reported by: E Hunt, MPH, P Lurie, MD, J Lute, PhD, M Moll, MD, H Stafford, J Bart, DO, A Gray, MEd, V Urdaneta, MD, S Ostroff, MD, Pennsylvania Dept of Health. J Blostein, MPH, R Potter, DVM, E Wells, MD, Michigan Dept of Community Health. C Kilborn, MPH, D Martinez, MPH, Harris County Public Health and Environmental Svcs; M Lowrey, City of Houston Health and Human Svcs, R Espinoza, MPH, Texas Dept of State Health Svcs. A Ferraro, PhD, Applied Epidemiology Fellow, Council of State and Territorial Epidemiologists. P Kutty, MD, A Barskey, MPH, D Payne, PhD, S Redd, L Lowe, MS, J Rota, MPH, W Bellini, PhD, P Rota, PhD, J Seward, MBBS, Div of Viral Diseases; M Thorley, MPH, S Reef, MD, Global Immunizations Div, National Center for Immunization and Respiratory Diseases; C Kim, MD, J Sinclair, DVM, C Dykewicz, MD, F Averhoff, MD, Div of Global Migration and Quarantine, National Center for Preparedness, Detection, and Control of Infectious Diseases; T Chen, MD, M Nguyen, MD, EIS officers, CDC. Editorial Note:Measles is no longer endemic in the United States because of high 2-dose MMR vaccination coverage rates among children and adolescents (1) in conjunction with effective surveillance and outbreak response. Today, measles among U.S. residents typically is linked to imported cases, although source cases are not always detected (2). Imported cases have caused outbreaks resulting in morbidity and substantial expenditure of local, state, and federal public health resources (5,7). This importation-associated outbreak demonstrates the highly infectious nature of measles, the potential severity of the disease (case 5), and the possibility that illness can occur among persons not considered at high risk for measles (cases 3, 6, and 7). Although the risk for measles transmission through air travel in the United States is considered low because of high U.S. population immunity (8), infection was transmitted to an airline passenger and at least one airport worker. Persons in routine contact with international travelers entering the United States can be exposed to persons with measles. All persons aged >12 months without adequate evidence of immunity should receive 1 or 2 doses of measles or MMR vaccine in accordance with current recommendations (6). Vaccination records should be actively maintained for adults and children. Although 2 doses of measles vaccine are 99% effective, cases can still occur in appropriately vaccinated persons, as observed in this investigation (cases 6 and 7). Likewise, persons born before 1957 might also remain susceptible to measles. Health-care providers should consider measles in any person with clinically compatible illness. As endemic measles has disappeared in the United States, viral genotyping has become an increasingly important component of measles surveillance. The variety of measles genotypes now detected in the United States reflects measles activity in countries of visitor origin and countries visited by U.S. travelers. Genotype D5 was associated with a large, concurrent outbreak in Japan.§ The identical genotype D5 sequences obtained from the index patient, who came from Japan, and from five of six patients with secondary cases suggests that Japan was the source of the virus and confirms the epidemiologic link between the cases. Because international events provide opportunities for measles transmission (3,9), organizers of large gatherings attended by international travelers, especially youths, should consider documentation of adequate participant vaccination. To prevent spread of measles, international travelers are encouraged to be fully vaccinated. MMR vaccine, administered to susceptible persons within 72 hours of measles exposure, is a recommended intervention for measles outbreak containment.¶ Ongoing circulation of measles virus outside the United States necessitates continued measures by national and international health agencies to achieve and maintain high vaccination coverage rates. After success in eliminating endemic measles virus transmission in the Pan-American Health Organization Region in 2002, three other World Health Organization regions have established target dates for measles elimination: the European and Eastern Mediterranean regions by 2010, and the Western Pacific Region (of which Japan is a member) by 2012. The attack rate of measles among susceptible persons has been documented as >90% (10). Previous imported measles cases have demonstrated the potential for larger outbreaks in U.S. communities with poor vaccination coverage (3). The small number of identified cases in this outbreak, despite the large number of exposed persons, demonstrates the value of maintaining high measles vaccination coverage in the U.S. population through adherence to routine vaccination recommendations. This outbreak also highlights the continuing importance of promoting measles control and elimination in other countries and sustaining strong surveillance and response measures in the United States. Acknowledgments This report is based, in part, on data contributed by J Lundy; J Battin, D Fontaine, J Mincer, C Nicolardi, M Dincher, and other Northcentral District staff members; J Clodgo, A Regec, M Strohecker, Pennsylvania Dept of Health. R Pestronk, Genesee County Health Dept; K Lokar, S Tremonti, L Childers, Macomb County Public Health; C Bird, S Bies, K Burdinie, Oakland County Health Div, Michigan. D Blythe, Maryland Dept of Health and Mental Hygiene. J Butwin, C Jones, V Caine, Marion County Health Dept; K Buffin, W Staggs, Indiana State Dept of Health. A Siston, Chicago Dept of Public Health, Illinois. C Fruthaler, U Shah, H Palacio, R Obey, M Garza, Harris County Public Health and Environmental Svcs; A Awosika-Olumo, S Khuwaja, M Chin, T Fasoranti, City of Houston Health and Human Svcs; T Kram, W Sessions, Texas Dept of State Health Svcs. D Kodagoda, V Nguyen, Los Angeles County Dept of Public Health; M McDonald, Orange County Health Agency; R Shaikh, California Dept of Public Health. E Ward, Georgia Div of Public Health. E Lopareva, Div of Viral Diseases, National Center for Immunization and Respiratory Diseases; J Thomas, S Blumensaadt, K Marienau, G Palumbo, Div of Global Migration and Quarantine, National Center for Preparedness, Detection, and Control of Infectious Diseases, CDC. References
* Available at http://www.cdc.gov/ncphi/disss/nndss/casedef/measles_current.htm. † World Health Organization. International health regulations (2005). Geneva, Switzerland: World Health Organization; 2005. Available at http://www.who.int/csr/ihr/en. § Infectious Disease Surveillance Center. Measles update in Japan as of week 21 (from 21 to 27 May 2007). Tokyo, Japan: National Institute of Infectious Diseases, Infectious Disease Surveillance Center; 2007. Available at http://idsc.nih.go.jp/disease/measles_e/idwr200721.html. ¶ American Academy of Pediatrics. Summaries of infectious diseases: measles. In: Pickering LK, Baker CJ, Long SS, McMillan JA, eds. Red book: 2006 report of the Committee on Infectious Diseases. 27th ed. Elk Grove Village, IL: American Academy of Pediatrics; 2006:443.
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to [email protected].Date last reviewed: 2/20/2008 |
|||||||||
|