|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
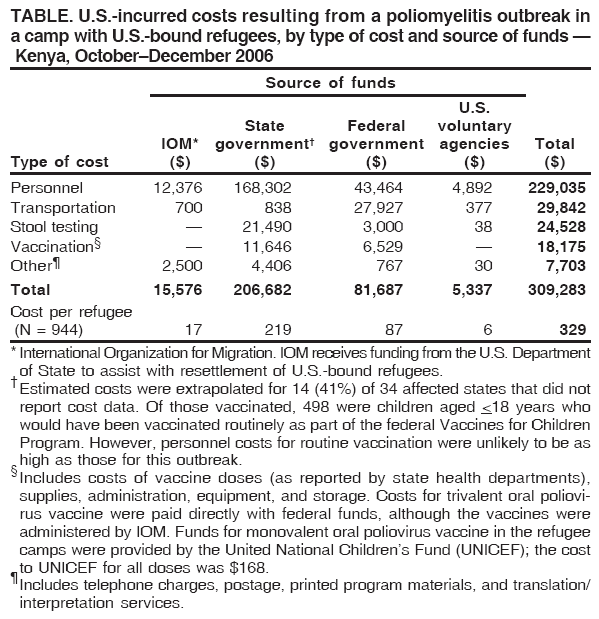
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail. U.S.-Incurred Costs of Wild Poliovirus Infections in a Camp with U.S.-Bound Refugees --- Kenya, 2006Routine predeparture vaccinations are not required for U.S.-bound refugees,* a policy that potentially leaves U.S. communities vulnerable to importation of vaccine-preventable diseases. During October--December 2006, an outbreak of poliomyelitis associated with wild poliovirus type 1 (WPV1) occurred in a camp occupied by refugees awaiting resettlement to the United States. This report describes the costs of domestic and international activities borne by U.S. federal and state governments, U.S.-funded organizations, and U.S. voluntary agencies during their response to this outbreak. Requiring predeparture polio vaccinations for U.S.-bound refugees might reduce the risk for poliovirus importation and reduce the costs associated with responses to polio outbreaks among refugees. On October 16, 2006, CDC was notified of a laboratory-confirmed case of WPV1 infection in a refugee aged 3 years with paralytic polio living in one of three refugee camps in the Dadaab region of northeastern Kenya near Somalia. The camps mostly were occupied by Somali refugees and recently had received an influx of approximately 30,000 persons from Somalia. A second case of WPV1 infection in a child aged 12 years who was living in the same refugee camp was confirmed on December 19. These were the first virologically confirmed cases of polio reported in Kenya in 22 years (1). Viral isolates were genetically linked to WPV1 isolated from specimens in Somalia (2,3). Both children had been born in the camp, had not traveled outside the camp, and had completed all routine childhood vaccinations, including trivalent oral poliovirus vaccine (tOPV), in accordance with World Health Organization (WHO) Expanded Program on Immunization recommendations.† In response to the first polio case, the Kenya Ministry of Health, the United Nations High Commissioner for Refugees, the United Nations Children's Fund (UNICEF), WHO, and several nongovernmental organizations conducted three campaigns to vaccinate children aged <5 years in the camps with monovalent oral poliovirus vaccine type 1 (mOPV1), which is more immunogenic on a per-dose basis against WPV1 than tOPV. At the time of CDC notification of the first case on October 16, a total of 944 refugees from Kenyan camps had recently arrived in or were en route to the United States; of these, 733 refugees had arrived during September 1--October 15 (group 1), 48 were on a trans-Atlantic flight (group 2), and 163 were staying in the Nairobi Transit Center in Kenya, awaiting imminent departure for the United States (group 3). The center is operated by the International Organization for Migration (IOM), which provides overseas medical assessments and care for U.S.-bound refugees during the resettlement process. CDC tracked these 944 refugees, notified the 34 receiving state health departments, and provided recommendations for polio vaccination and follow-up (5). On October 17, before departure from Kenya, group 3 refugees were checked for signs and symptoms of polio (e.g., paralysis, weakness, or meningitis). IOM administered 1 dose of tOPV because mOPV was not available before departure. After arrival in the United States, all three groups of refugees received at least 1 dose of inactivated poliovirus vaccine (IPV) and, for 4 weeks after arrival, all refugees were under active surveillance for signs and symptoms of polio conducted by state and local health departments. Because they could not be vaccinated before departure, the refugees who arrived on the flight on October 16 (group 2) had one stool specimen tested for poliovirus in addition to postarrival vaccination and active surveillance. Some states chose to test one stool specimen from refugees who arrived on other dates. Recommendations for overseas and domestic testing of stool specimens for poliovirus have been published previously (5). In addition to the 944 refugee arrivals, approximately 1,200 refugees were living in the three Dadaab camps awaiting resettlement to the United States during the next several months (group 4). Future travel of these U.S.-bound refugees in the camps was suspended until they could receive 2 doses of mOPV separated by at least 1 week. To obtain polio response--related cost data, CDC requested information from the following sources: IOM; U.S. state and local health departments that conducted vaccination and follow-up of refugees after arrival in the United States; U.S. Department of Health and Human Services agencies, including CDC and the Office of Refugee Resettlement (ORR), that provided funding and guidance for domestic refugee medical screenings, follow-up, and treatment (6); and 13 U.S. voluntary agencies that assisted refugees with resettlement. Data collected on the response included the cost of the following: tOPV and IPV and administration; salary, hours allocated, and associated overhead; stool-specimen evaluation; transportation, such as nonrefundable tickets, travel within Kenya, and transport of refugees for vaccination and predeparture checks; and communication. Data collected from IOM represented the costs to the U.S. government of vaccinating refugees against polio before embarkation. Because UNICEF provided the mOPV1 used to vaccinate the refugees in the camps, no direct cost was incurred by the U.S. government or government-funded agencies for mOPV1 administered to refugees overseas. An average cost per refugee was calculated, based on cost data for 603 (64%) of the 944 refugees, provided by 20 (59%) of the 34 receiving states. The average cost per refugee was then extrapolated to all 944 refugees to estimate the total cost. Because all costs were incurred within 1 year, no future costs or discounts to current values were calculated. CDC received follow-up health data on 833 (88%) of the 944 refugee arrivals, from 32 (94%) of the 34 receiving states. As part of the response, 163 (17%) of the refugees received tOPV overseas, and 691 (83%) received IPV domestically. Approximately 1,200 refugees received 2 doses of mOPV1 overseas while awaiting resettlement. No cases of polio were identified in the United States, and WPV was not isolated from any of the 372 stool specimens tested by CDC and state health departments. The total U.S.-incurred cost of this response was $309,283 (Table). Personnel compensation, at $229,035, accounted for approximately 74% of the total cost; transportation-associated costs, at $29,842, accounted for nearly 10% of the total. A total of 5,271 personnel hours were logged, 3,271 doses of polio vaccine were administered, and 1,052 miles were traveled by automobile as part of this response. Reported by: CDC International Emerging Infections Program, Kenya. Deutsche Gesellschaft für Technische Zusammenarbeit (GTZ), Eschborn, Germany. United Nations High Commissioner for Refugees. Office of Refugee Resettlement, US Dept of Health and Human Svcs. A Casano, Div of Global Migration and Quarantine, Div of Emerging Infections and Surveillance Svcs, National Center for Preparedness, Detection, and Control of Infectious Diseases; Div of Viral Diseases, Global Immunization Div, National Center for Immunization and Respiratory Diseases, CDC. Editorial Note:Risk for paralytic polio is low in the U.S. population because of sustained high routine vaccination coverage of infants and children and decreasing risk for importation of WPV from a declining number of countries where polio is endemic or outbreaks occur (7). However, certain U.S. subpopulations remain at risk because of vaccination refusal, including refusals based on religious or personal beliefs. Despite progress in global polio eradication, the risk for WPV importation will continue until eradication has been achieved. The identification of WPV1 cases in the Dadaab refugee camps led to a resource-intensive response, with costs incurred for emergency vaccination of refugees who had recently arrived or were en route to the United States, mass polio vaccination campaigns for refugees awaiting resettlement, intensified surveillance, and resettlement logistics. Until polio is eradicated worldwide, the potential remains for the U.S. government or government-funded agencies to incur certain costs associated with measures to prevent importation of poliovirus into the United States. However, the cost of responding to outbreaks might be reduced by requiring that vaccines recommended by the Advisory Committee on Immunization Practices (ACIP) (8) be administered to U.S.-bound refugees before departure. Routine predeparture vaccinations can be administered at the time of the required medical examination, which is usually performed 6 months before departure, allowing sufficient time for seroconversion and the development of immunity. The costs of outbreak responses are substantially higher than those of routinely administering vaccinations overseas. A cost analysis indicated that predeparture vaccination of approximately 50,000 refugees with all doses of all routine ACIP-recommended vaccination would cost approximately $7.7 million overseas, compared with $26 million domestically (9), a savings of approximately $18 million. Funds for vaccinating refugee children in the United States are provided as part of the federal Vaccines for Children Program. Coverage of costs for vaccinating adult refugees depends on program policies in the receiving state. The cost of certain adult vaccinations is covered by Refugee Medical Assistance, federal funds that are provided to the states by ORR to cover postarrival medical screening of refugees (6). Because routine poliovirus vaccination of adults is not recommended by ACIP (8), many states do not routinely administer IPV to recently arrived adult refugees. The findings in this report are subject to at least three limitations. First, certain states and voluntary agencies did not submit data; therefore, total costs might be underestimated. Although costs from 20 states were extrapolated to the 34 affected states, the 14 states that did not provide such data might have incurred higher costs; in addition, costs were not extrapolated to voluntary agencies that did not report such data. Second, the percentage of costs exclusively attributable to the resettlement program is difficult to estimate. A portion of the costs associated with the outbreak response in the camps would have been incurred as a result of controlling the outbreak, regardless of resettlement status, although these costs would have been reduced if the refugees had been routinely vaccinated overseas. Finally, although the cost of this outbreak included nonrefundable tickets, previous outbreak costs have also included rebooking fees. During an outbreak response in 2003, rebooking fees were estimated at $400,000 (i.e., $1,000 per ticket) (IOM, unpublished data, 2003). Because rebooking fees might be greater in future responses, the costs presented in this report might underestimate future costs. The response by U.S. public health agencies described in this report did not identify any cases of imported poliovirus or any poliovirus-infected persons in the United States. However, the cost of the response suggests that routine predeparture vaccination of U.S.-bound refugees in accordance with ACIP recommendations might further decrease the small risk for poliovirus importation and result in cost savings to the United States by reducing the number of future responses to polio outbreaks among refugees. Acknowledgments This report is based, in part, on data contributed by the International Organization for Migration, the Office of Refugee Resettlement, US Dept of Health and Human Svcs, state and local health departments, Lutheran Social Svcs of North Dakota, Catholic Charities (Charlotte, North Carolina; Kansas City, Missouri; San Diego, California; Kentucky; and Texas), US Committee for Refugees and Immigrants of Vermont, World Relief of Illinois, Catholic Community Svcs of Utah, International Rescue Committee of Utah, and the International Institute of Erie, Pennsylvania. References
* Immigration and Nationality Act section 212 (8 U.S.C. 1182)(a)(1)(A)(ii) as amended by section 341 of the Illegal Immigration Reform and Immigrant Responsibility Act of 1996. † For various reasons (e.g., malnutrition and enteric infections), the effectiveness of tOPV in children living in tropical, less developed countries is lower than in children living in temperate, more developed countries (4). Therefore, not all children who are vaccinated with 3 doses of tOPV through routine immunization programs are immune to WPV infection and paralysis.
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to [email protected].Date last reviewed: 3/5/2008 |
|||||||||
|