|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
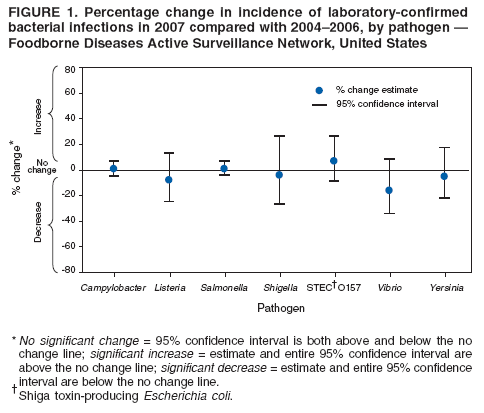
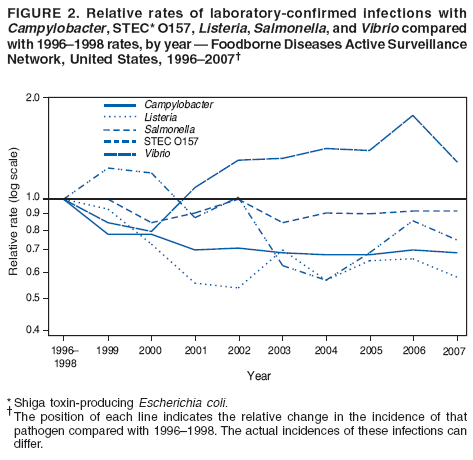
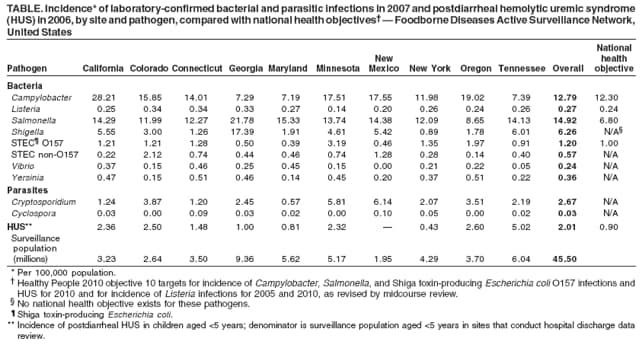
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail. Preliminary FoodNet Data on the Incidence of Infection with Pathogens Transmitted Commonly Through Food --- 10 States, 2007The Foodborne Diseases Active Surveillance Network (FoodNet) of CDC's Emerging Infections Program collects data from 10 U.S. states* regarding diseases caused by pathogens commonly transmitted through food. FoodNet quantifies and monitors the incidence of these infections by conducting active, population-based surveillance for laboratory-confirmed infections (1). This report describes preliminary surveillance data for 2007 and compares them with data for previous years. In 2007, the estimated incidence of infections caused by Campylobacter, Listeria, Shiga toxin-producing Escherichia coli O157 (STEC O157), Salmonella, Shigella, Vibrio, and Yersinia did not change significantly, and Cryptosporidium infections increased compared with 2004--2006. Progress toward the targets for Healthy People 2010 national health objectives and targets (2) regarding the incidence of foodborne infections occurred before 2004; however, none of the targets were reached in 2007. Salmonella incidence was the furthest from its national health target, suggesting that reaching this target will require new approaches. Surveillance MethodsIn 1996, FoodNet began active, population-based surveillance for laboratory-confirmed cases of infection caused by Campylobacter, Listeria, Salmonella, STEC O157, Shigella, Vibrio, and Yersinia. FoodNet added surveillance for cases of Cryptosporidium and Cyclospora infection in 1997 and STEC non-O157 infection in 2000. In 2004, FoodNet began collecting data regarding which laboratory-confirmed infections were associated with outbreaks. Infection with STEC O157 can cause hemolytic uremic syndrome (HUS), a complication in which the kidneys fail. HUS surveillance, which began in 2000, is conducted in nine states through a network of pediatric nephrologists and infection-control practitioners and validated through review of hospital discharge data. Because of the time required for review of hospital records, this report contains preliminary HUS data for 2006. During 1996--2007, the FoodNet surveillance population increased from 14.3 million persons (5% of the U.S. population) in five states to 45.5 million persons (15% of the U.S. population) in 10 states. The preliminary incidence for 2007 was calculated by dividing the number of laboratory-confirmed infections by population estimates for 2006. Final incidence will be reported when population estimates for 2007 are available from the U.S. Census Bureau. In previous years, final incidence has been comparable to preliminary incidence. Surveillance DataIn 2007, a total of 17,883 laboratory-confirmed cases of infection in FoodNet surveillance areas were identified. The number of cases and incidence per 100,000 population were reported as follows: Salmonella (6,790; 14.92), Campylobacter (5,818; 12.79), Shigella (2,848; 6.26), Cryptosporidium (1,216; 2.67), STEC O157 (545; 1.20), STEC non-O157 (260; 0.57), Yersinia (163; 0.36), Listeria (122; 0.27), Vibrio (108; 0.24), and Cyclospora (13; 0.03). Substantial variation occurred across surveillance sites (Table). The highest incidence per 100,000 population for Salmonella (62.11), Shigella (27.77), Campylobacter (24.01), and STEC O157 (3.66) infections was among children aged <5 years. In 2006, FoodNet identified 82 cases of postdiarrheal HUS in persons aged <18 years (0.78 cases per 100,000 children); 58 (0.7%) cases occurred in children aged <5 years (2.01 cases per 100,000 children). Of the 6,299 (92.8%) Salmonella isolates serotyped, seven serotypes accounted for 61.6% of infections: Enteritidis, 1,062 (16.9%); Typhimurium, 1,006 (16.0%); Newport, 656 (10.4%); I 4,[5],12:i:-, 358 (5.7%); Javiana, 347 (5.5%); Heidelberg, 243 (3.9%); and Montevideo, 211 (3.4%). Among 102 (94.4%) Vibrio isolates for which the species was identified, 59 (57.8%) were parahaemolyticus, 18 (17.7%) were alginolyticus, and 13 (12.8%) were vulnificus. Among 260 STEC non-O157 isolates tested for O antigen determination, 228 (87.7%) had an identifiable O antigen, primarily O26 (21.5%), O103 (20.6%), or O121 (19.3%). Comparison with Previous YearsA main-effects, log-linear Poisson regression model (negative binomial) was used to estimate statistically significant changes in incidence of infections in 2007 compared with previous years. This model accounts for the increase in the surveillance population and for variations in incidence among sites (1). The average annual incidence for 2004--2006 and for 1996--1998 (1997--1998 for Cryptosporidium), the first years of surveillance, were used for comparison. The estimated change in incidence (relative rate) between 2007 and the comparison periods was calculated, along with 95% confidence intervals (CIs). For HUS surveillance, 2000--2001, the first years of surveillance, was used as the comparison period. Changes over time have not been analyzed for non-O157 STEC, partly because changes in clinical laboratory practices might have affected incidence reporting (3). The estimated incidence of Campylobacter, Listeria, Salmonella, Shigella, STEC O157, Vibrio, and Yersinia infections (Figure 1) did not change significantly in 2007 compared with 2004--2006, but the estimated incidence of Cryptosporidium infections increased 44% (CI = 8%--91%). Among the seven most common Salmonella serotypes, the incidence of Typhimurium and Heidelberg decreased, I 4,[5],12:i- and Newport increased, and the others did not change significantly. In comparison with 1996--1998, relative rates of Yersinia decreased 49% (CI = 36%--59%), Listeria decreased 42% (CI = 28%--54%), Shigella decreased 36% (CI = 9%--55%), Campylobacter decreased 31% (CI = 25%--36%), STEC O157 decreased 25% (CI = 9%--38%), and Salmonella decreased 8% (CI = 1%--14%) in 2007 (Figure 2). The estimated incidence of infection with Cryptosporidium and Vibrio did not change significantly. The incidence of postdiarrheal HUS has paralleled that of STEC O157, declining in 2003 and 2004, followed by increases the next 2 years. The estimated incidence of postdiarrheal HUS in children aged <5 years in 2006 did not change significantly compared with 2000--2001. Outbreak-Associated Cases of InfectionIn 2007, outbreak-associated infections accounted for 86 (15.8%) of STEC O157 cases and 364 (5.4%) of Salmonella cases ascertained, similar to proportions in previous years. Four large multistate outbreaks of Salmonella infections that included FoodNet sites were investigated in 2007: an outbreak of S. Tennessee infections caused by contaminated peanut butter (4), an outbreak of S. I 4,[5],12:i:- infections caused by contaminated frozen pot pies, an outbreak of S. Wandsworth and S. Typhimurium infections attributed to a puffed vegetable snack, and an outbreak of S. Paratyphi B var. Java associated with exposure to turtles (5). Reported by: D Vugia, MD, California Dept of Public Health. A Cronquist, MPH, Colorado Dept of Public Health and Environment. J Hadler, MD, Connecticut Dept of Public Health. M Tobin-D'Angelo, MD, Div of Public Health, Georgia Dept of Human Resources. D Blythe, MD, Maryland Dept of Health and Mental Hygiene. K Smith, DVM, Minnesota Dept of Health. S Lathrop, PhD, New Mexico Dept of Health. D Morse, MD, New York State Dept of Health. P Cieslak, MD, Oregon Public Health Div. J Dunn, DVM, Tennessee Dept of Health. PL White, DVM, Food Safety and Inspection Svc, US Dept of Agriculture. JJ Guzewich, MPH, Center for Food Safety and Applied Nutrition, Food and Drug Admin. OL Henao, PhD, RM Hoekstra, PhD, E Scallan, PhD, FJ Angulo, DVM, PM Griffin, MD, RV Tauxe, MD, Div of Foodborne, Bacterial and Mycotic Diseases, National Center for Zoonotic, Vector-Borne and Enteric Diseases; C Barton Behravesh, DVM, EIS Officer, CDC. Editorial Note:Although significant declines in the incidence of certain foodborne pathogens have occurred since 1996, these declines all occurred before 2004. Comparing 2007 with 2004--2006, the estimated incidence of infections caused by Campylobacter, Listeria, Salmonella, Shigella, STEC O157, Vibrio, and Yersinia did not decline significantly, and the incidence of Cryptosporidium infections increased. The incidence of Salmonella infections in 2007 (14.92 cases per 100,000) was the furthest from the national target for 2010 (6.80 cases), and only infections caused by Salmonella serotypes Typhimurium and Heidelberg declined significantly. Salmonella organisms live in the intestines of most food animals. Transmission of Salmonella to humans can occur by many routes, including consumption of food animal products or raw produce contaminated with animal waste, contact with animals and their environment, and contaminated water. Outbreaks caused by contaminated peanut butter, frozen pot pies, and a puffed vegetable snack in 2007 underscore the need to prevent contamination of commercially produced products. The outbreak associated with turtle exposure highlights the importance of animals as a nonfood source of human infections. To reduce the incidence of Salmonella infections, concerted efforts are needed throughout the food supply chain, from farm to processing plant to kitchen. Recognizing the need to prevent Salmonella contamination of poultry products and other meats, the U.S. Department of Agriculture's Food Safety and Inspection Service (USDA FSIS) launched a Salmonella initiative in 2006, with enhancements in 2008 (5). A USDA FSIS testing program reported recent declines in the percentage of broiler chicken carcasses that yielded Salmonella, from 16.3% in 2005 to 11.4% in 2006 and 8.5% in 2007 (7). Declines in the incidence of STEC O157 infections in 2003 and 2004 have not been maintained. Although the USDA FSIS and the beef processing industry have implemented interventions to reduce ground beef contamination, 21 beef product recalls for possible contamination with STEC O157 were issued in 2007, of which 10 were illness associated, an increase compared with previous years. USDA FSIS launched an STEC O157 initiative in fall 2007 and hosted a public meeting in spring 2008 to explore solutions to the challenges this pathogen presents.† Additional efforts are needed to control STEC O157 in cattle and to prevent its spread to other food animals and food products, such as produce. The increase in reported Cryptosporidium infections compared with 2004--2006 might reflect an increase in diagnostic testing stimulated by licensing of a new treatment (nitazoxanide). The incidence of Campylobacter, Salmonella, Shigella, and STEC O157 infections remains highest among children aged <5 years, highlighting the need for targeted interventions. Identified risk factors for bacterial enteric illness in young children include riding in a shopping cart next to raw meat or poultry, attendance at day care, visiting or living on a farm, and living in a home with a reptile (8,9). Recent Salmonella outbreaks associated with exposure to small turtles (carapace lengths of <4 inches) highlight the importance of enforcing a 1975 prohibition on their sale and distribution in the United States (5). The findings in this report are subject to at least four limitations. First, FoodNet relies on laboratory diagnoses, and changing laboratory practices might affect the reported incidence for some pathogens, especially STEC. Second, many foodborne illnesses (e.g., norovirus) are not reported to FoodNet. Third, differences in health-care seeking behaviors might contribute to a higher incidence of reported illnesses in certain age groups (e.g., young children). Finally, although the FoodNet population is similar to the U.S. population, the findings might not be generalizable (1). Enhanced measures are needed to understand the complex ecologies that link pathogens to animals and plants; to control or eliminate pathogens in food sources; to reduce or prevent contamination during food growing, harvesting, and processing; and to educate restaurant workers and consumers about infection risks and prevention measures. Such measures can be more focused when the sources of human infections are known. More outbreaks can be recognized through more rapid and complete subtyping of pathogens and interviewing of ill persons and controls when clusters of illness are recognized. Consumers can reduce their risk for foodborne illness by following safe food-handling and preparation recommendations and avoiding unsafe foods. Information on food safety practices is available at http://www.foodsafety.gov, http://www.fightbac.org, and http://www.cdc.gov/healthypets. References
* Connecticut, Georgia, Maryland, Minnesota, New Mexico, Oregon, Tennessee, and selected counties in California, Colorado, and New York. † Additional information about USDA FSIS and the STEC O157 initiative and meeting is available at http://www.fsis.usda.gov.
Figure 1
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to [email protected].Date last reviewed: 4/9/2008 |
|||||||||
|