|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
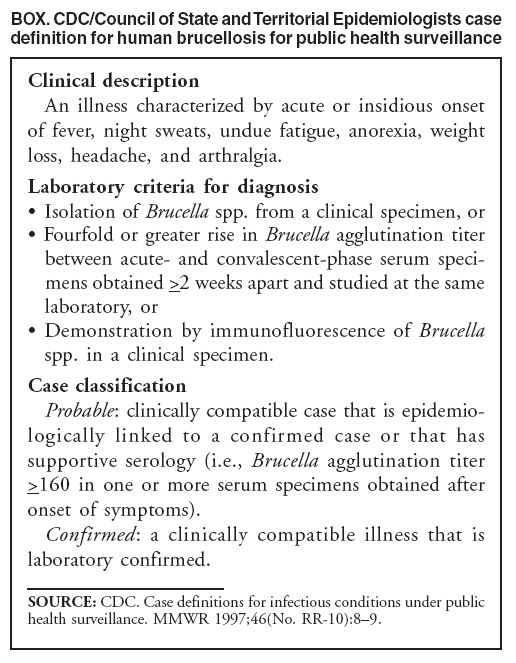
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail. Public Health Consequences of a False-Positive Laboratory Test Result for Brucella --- Florida, Georgia, and Michigan, 2005Human brucellosis, a nationally notifiable disease, is uncommon in the United States. Most human cases have occurred in returned travelers or immigrants from regions where brucellosis is endemic, or were acquired domestically from eating illegally imported, unpasteurized fresh* cheeses (1,2). In January 2005, a woman aged 35 years who lived in Nassau County, Florida, received a diagnosis of brucellosis, based on results of a Brucella immunoglobulin M (IgM) enzyme immunoassay (EIA) performed in a commercial laboratory using analyte specific reagents (ASRs); this diagnosis prompted an investigation of dairy products in two other states. Subsequent confirmatory antibody testing by Brucella microagglutination test (BMAT) performed at CDC on the patient's serum was negative. The case did not meet the CDC/Council of State and Territorial Epidemiologists' (CSTE) definition for a probable or confirmed brucellosis case (3) (Box), and the initial EIA result was determined to be a false positive. This report summarizes the case history, laboratory findings, and public health investigations. CDC recommends that Brucella serology testing only be performed using tests cleared or approved by the Food and Drug Administration (FDA) or validated under the Clinical Laboratory Improvement Amendments (CLIA) and shown to reliably detect the presence of Brucella infection. Results from these tests should be considered supportive evidence for recent infection only and interpreted in the context of a clinically compatible illness and exposure history. EIA is not considered a confirmatory Brucella antibody test; positive screening test results should be confirmed by Brucella-specific agglutination (i.e., BMAT or standard tube agglutination test) methods. On February 1, 2005, the Nassau County Health Department received a report, based on a positive Brucella antibody test result, of a possible case of brucellosis in a female resident aged 35 years. The woman reported having intermittent fever, chills, sweats, body aches, weakness, headaches, and malaise since October 13, 2004. She was examined first at a local emergency department in November 2004, diagnosed with acute bronchitis, and discharged without a prescription for antimicrobials. She subsequently was examined by an infectious disease specialist on January 3, 2005, at which time brucellosis was considered based on continued nonspecific symptoms, polyarthritis, and an atypical lymphocytosis seen on a peripheral blood smear. Blood was obtained for culture and Brucella antibody testing on January 3 and January 24. Blood cultures were negative after 10 days. The EIA results from a commercial laboratory were interpreted as positive IgM and negative IgG, consistent with early brucellosis. On the basis of these results, on February 1 the patient was prescribed a twice daily, 6-week course of antimicrobial therapy of doxycycline (100 mg) and rifampin (300 mg). She stopped taking both antimicrobials after a short period because of side effects. After confirmatory testing by BMAT of the January 24 serum sample, performed February 14 at CDC, was negative, no further treatment for brucellosis was recommended. No other infectious etiologies were identified as a cause of the patient's symptoms, and she was lost to follow-up. After the February 1 report, but before receiving the negative BMAT results, Nassau County and Florida epidemiologists began an investigation to identify possible exposures to Brucella species. The patient reported no recent contact with animals or animal fluids. She had eaten goat cheese from several sources while traveling in Michigan during May--July 2004 and while staying at a Georgia youth hostel in July 2004, 3--5 months before her illness onset. No unpasteurized dairy products were discovered at the identified sources that supplied locations where the woman ate. At the youth hostel, all dairy products used for cooking were pasteurized and purchased from local markets; however, guests often contributed food they had brought with them, and exact origins of shared foods were difficult to determine. Reported by: A Pragle, MS, C Blackmore, DVM, Florida Dept of Health. TA Clark, MD, Div of Bacterial Diseases, National Center for Immunization and Respiratory Diseases; MD Ari, PhD, PP Wilkins, PhD, Div of Foodborne, Bacterial, and Mycotic Diseases, National Center for Zoonotic, Vector-Borne, and Enteric Diseases; D Gross, DVM, PhD, EJ Stern, MD, EIS officers, CDC. Editorial Note:Brucellosis is a classic bacterial zoonosis. Common Brucella species that are pathogenic in humans and their usual animal reservoirs include B. melitensis in sheep and goats, B. abortus in cattle, and B. suis in swine. B. melitensis, considered the most pathogenic species in humans, has not been reported in animals in the United States since 1999. Symptoms of human brucellosis vary, and include periodic or undulant fever, muscle aches, back pain, and fatigue. Diagnosis can be difficult because brucellosis has a prolonged and variable incubation period (5 days to 5 months), often presents as a nonspecific febrile syndrome, and occurs in acute, chronic, and asymptomatic forms. Definitive diagnosis of brucellosis requires isolation and identification of the Brucella species. More commonly, cases are diagnosed serologically by detection of agglutinating antibodies. The reference method is the standard tube agglutination test (SAT), of which BMAT is a modified format (4). Brucella-specific agglutination tests involve direct agglutination of bacterial antigens by specific antibodies. Agglutination tests detect antibodies of IgM, IgG, and IgA classes. IgM antibodies are predominant in acute infection but decline within weeks, whereas relapses are accompanied by transient elevations of IgG and IgA antibodies but not IgM (5). Evidence of Brucella antibody by nonagglutination-based tests does not meet the current CDC/CSTE case definition for brucellosis (Box). In the context of a clinically compatible illness, brucellosis is confirmed by a fourfold or greater rise in Brucella agglutination titer between acute- and convalescent-phase serum specimens obtained at least 2 weeks apart, isolation of Brucellae in culture, or demonstration of organism presence by specific immunohistochemical staining (3). A clinically compatible case that is epidemiologically linked to a confirmed case or that has supportive serology (i.e., Brucella agglutination titer of >160 in one or more serum specimens obtained after onset of symptoms) is considered a probable case. The Brucella EIA reagents used in this investigation were obtained from Panbio, Inc. (Columbia, Maryland); they are sold as ASRs in the United States but elsewhere as complete test kits. ASRs are used as active components of assays developed by individual clinical laboratories (6). Laboratories that use ASRs are responsible for evaluating and validating their assay and for establishing and maintaining assay interpretation and performance criteria, including sensitivity and specificity (6). Specificity of the Panbio IgM and IgG EIA, based on a study in a brucellosis endemic area, was reported as 100% (7); IgM detection sensitivities using different EIA formats has been reported as 67%--100%, with limited specificity data (8). Such tests might have different performance characteristics when used in areas with low disease prevalence, such as the United States. The CDC laboratory has observed that specimens that were positive using EIA tests from commercial laboratories often were negative when tested by BMAT. Results of EIA tests must be confirmed by a reference method such as BMAT, which is quantitative and provides evidence of rising antibody titers when paired sera are tested. Cross-reactions and false-positive test results can occur in Brucella antibody tests. The primary immunodeterminant and virulence factor for Brucella species is the cell wall surface lipopolysaccharide, which is antigenically similar to the lipopolysaccharide of other gram-negative rods. False-positive Brucella antibody test results can be caused by cross-reactivity of antibodies to Escherichia coli O157, Francisella tularensis, Moraxella phenylpyruvica, Yersinia enterocolitica, and certain Salmonella species (9). Most cross-reacting antibodies are IgM (10), making interpretation of any IgM assay difficult because of false positivity. Therefore, results obtained using EIA should be confirmed by a reference method. This investigation highlights the need to confirm screening serologic test results by using established reference testing methods and to identify the presence of known risk factors before committing a patient to prolonged antimicrobial therapy for brucellosis or initiating public health investigations. Testing of persons with compatible signs and symptoms for brucellosis should be supported by a thorough history that reveals likely exposure through travel to an area where brucellosis is endemic, consumption of an unpasteurized dairy product, hunting potentially infected wildlife species, or laboratory exposure. Testing of persons in the absence of a suggestive exposure increases the likelihood of false-positive results and lowers the overall positive predictive value of the assay used. Rapid Brucella antibody assays can be useful as screening tools when results are interpreted in the context of performance characteristics of the particular test; however, CDC recommends that all positive results obtained by rapid serologic assays be confirmed with Brucella-specific agglutination testing. For questions about risk factors or to request confirmatory testing for brucellosis in patients with strong evidence of exposure, health-care providers should contact their local or state health department. Acknowledgments The findings in this report are based, in part, on contributions by K Geib, Nassau County Health Dept; K Ward, Florida Dept of Health; and L Brumble, MD, Mayo Clinic, Jacksonville, Florida. References
* Fresh cheeses, such as cottage cheese and Neufchâtel, also are referred to as soft or unripened cheeses. They are made by curdling milk and draining the whey, with little additional processing, and spoil more quickly than processed hard cheeses.
All MMWR HTML versions of articles are electronic conversions from typeset documents. This conversion might result in character translation or format errors in the HTML version. Users are referred to the electronic PDF version (http://www.cdc.gov/mmwr) and/or the original MMWR paper copy for printable versions of official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to [email protected].Date last reviewed: 6/4/2008 |
|||||||||
|