|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
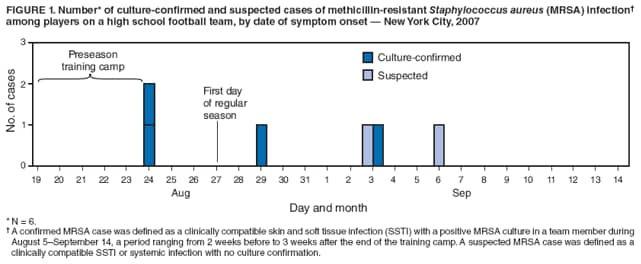
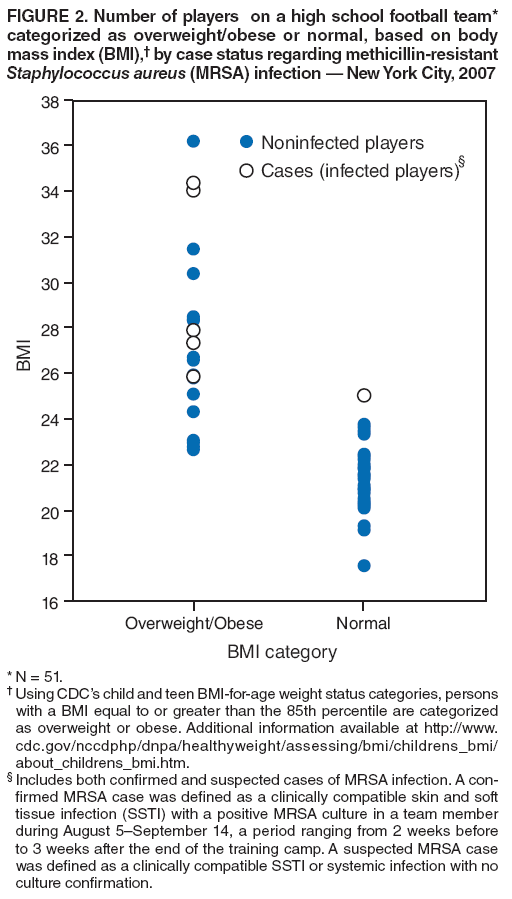
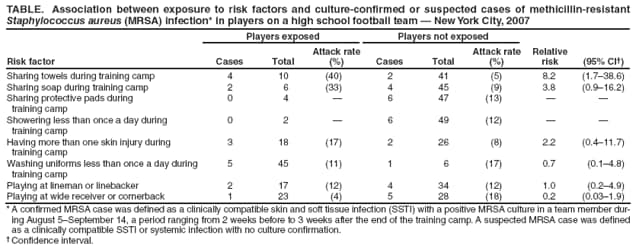
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail. Methicillin-Resistant Staphylococcus aureus Among Players on a High School Football Team --- New York City, 2007On September 12, 2007, the New York City Department of Health and Mental Hygiene (DOHMH) was notified of three players on a Brooklyn high school football team with culture-confirmed methicillin-resistant Staphylococcus aureus (MRSA) skin and soft tissue infections (SSTIs). During August 19--24, the team had attended a preseason football training camp, where all 59 players on the team lived together in the school gymnasium. An investigation by DOHMH revealed four culture-confirmed and two suspected cases of MRSA among 51 players interviewed (11.8% attack rate). Of the six cases, three involved abscesses that required incision and drainage. The risk for MRSA infection was higher among those who shared towels during the training camp than among those who did not (relative risk [RR] = 8.2). In addition, the six players with MRSA infections had a mean body mass index (BMI) that was significantly higher than the mean for those who were not infected. Multivariable logistic modeling determined that sharing towels during camp (adjusted odds ratio [AOR] = 15.7) and higher BMI (AOR = 1.4) were associated independently with MRSA infection. Similar outbreaks have been reported among football teams in which inadequate hygiene, combined with skin injuries and living in close quarters, contributed to the spread of MRSA infection. Such outbreaks might be prevented by better educating players and coaches regarding SSTIs and by better promoting proper player hygiene, particularly during training camps. Initial investigation by DOHMH began on September 12. Investigators learned that all 59 players had attended a preseason training camp during August 19--24. The players had lived together in the school gymnasium, slept on cots in close proximity to each other, and showered in the school locker room, usually only once at the end of the day. The school had supplied antibacterial soap in pump dispensers in the showers; however, several players brought their own soap. Players supplied their own towels. Players reported that they usually left their towels on their cots or on the floor when not in use. The school offered a daily laundry service for uniforms and towels during the camp; however, most players did not have their towels washed and wore their uniforms two or three times between launderings. Players often remained in sweat-soaked clothes between the morning and afternoon practices. The school did not have whirlpools or hot tubs. Investigators hypothesized that sharing facilities and equipment, previous skin injuries, player position, inadequate player hygiene, and having a higher BMI might be risk factors linked to MRSA infections (1--3). To find additional cases, identify risk factors for infection, and implement infection control measures, DOHMH conducted face-to-face interviews on September 14 with 51 of the 59 players, using a close-ended questionnaire; the eight remaining players could not be contacted. In addition, a DOHMH physician further examined the five players reported by the school nurse as potentially infected. A confirmed MRSA case was defined as a clinically compatible SSTI with a positive MRSA culture in a team member during August 5--September 14, a period ranging from 2 weeks before to 3 weeks after the end of the training camp. A suspected MRSA case was defined as a clinically compatible SSTI or systemic infection with no culture confirmation. Date of symptom onset was defined as the date an infected player reported first noticing an infected wound. Among the 51 players interviewed, four confirmed and two suspected MRSA cases were identified (11.8% attack rate). Molecular typing with pulsed-field gel electrophoresis revealed that three of the confirmed cases were USA300, a strain usually considered to be a community-associated MRSA. An isolate from the fourth player with confirmed MRSA was not available for typing. Symptom onsets ranged from August 24, the last day of training camp, to September 6, a total of 13 days after the camp (Figure 1). In the four confirmed cases, infections initially appeared as a blister on the ankle, calf, hip, or instep. One suspected case involved impetigo on the upper arm; the other suspected case involved impetigo on the arms and eyebrow. Three players reported their wounds to the school nurse or a physician only after blisters had developed into infections requiring medical attention. The six players with confirmed or suspected MRSA infections were referred to their personal physicians for treatment. Three of the players had abscesses that required incision and drainage. Three of the players with confirmed cases were treated with Bactrim and doxycycline, clindamycin and mupirocin, and Bactrim and mupirocin, respectively. One of the players with suspected MRSA infection was treated with ciprofloxacin. Antibiotics used to treat the remaining two players were unknown. Interviews with the players revealed that 33 (65%) had sustained at least one cut, abrasion, or turf burn during the preseason camp or regular season. The players reported that, unless the skin injuries were severe, they had cleaned, dressed, or bandaged them by themselves. No players reported sharing towels or soap during the regular season, because players went home after practice to shower. However, 10 (20%) had shared towels and six (12%) had shared soap during training camp, when the players showered on site. In a retrospective cohort analysis, after combining confirmed and suspected MRSA cases, bivariate RRs and their 95% confidence intervals (CIs) were calculated to identify risk factors associated with infection. Multivariable logistic regression was used to evaluate the independent association of multiple risk factors, including BMI, which was modeled as a continuous variable because the small number of cases did not allow for tests based on BMI categories (i.e., normal, overweight, and obese). Sharing towels during training camp significantly increased the risk for MRSA infection (RR = 8.2) (Table). Sharing protective pads, sharing soap, showering less than once a day, having more than one skin injury, and washing uniforms less than once a day were not significant risk factors for infection. Playing at lineman or linebacker and wide receiver or cornerback positions (previously shown to be potential risk factors in football MRSA outbreaks [2,4]) also were not significant risk factors (Table). The six players with MRSA infection had a mean BMI of 29.1 (CI = 24.7--33.3), which was significantly higher by t-test (t = 2.56; p=0.014) than the mean BMI of 23.8 (CI = 22.8--25.0) for the 45 players without infection. Using CDC's child and teen BMI-for-age weight status categories,* five of the six (83%) players with MRSA infection could be classified as overweight or obese, compared with 20 of the 45 (44%) players without infection (Figure 2). A bivariate analysis using logistic regression revealed that higher BMI was associated with higher risk for infection (OR = 1.3 per unit increase in BMI; CI = 1.1--1.7). A multivariable logistic model confirmed that both sharing towels during training camp (AOR = 15.7; CI = 1.5--167.4) and BMI (AOR = 1.4; CI = 1.1--1.9) were associated independently with MRSA infection. Reported by: P Kellner, MPH, A Yeung, MPH, HA Cook, MPH, J Kornblum, PhD, M Wong, MPH, F Eniola, MPH, D Weiss, MD, New York City Dept of Health and Mental Hygiene. HP Nair, PhD, EIS Officer, CDC. Editorial Note:Since 2000, outbreaks of MRSA SSTIs have been reported among players on high school, college, and professional football teams with attack rates similar to those described in this report (1--4). Despite education efforts by CDC and state and local health departments, MRSA infections continue to be a problem among football players. A 2007 CDC survey of high school athletic trainers revealed that 53% had treated MRSA infections in football players (1). The results of this investigation suggest that sharing of towels among players at a preseason training camp was associated with MRSA infection, a risk factor previously linked to football-related MRSA outbreaks (1--3). These results are also consistent with three previous reports that identified MRSA infections in football teams temporally linked to training camps (2--4), which might be a setting that increases risk behaviors for infection (4). Living in close quarters for an extended period, a potential risk factor identified in other settings (5), might have further contributed to the outbreak. The results also indicated that higher BMI among team players was associated with higher risk for MRSA infection, independent of sharing towels. These results are consistent with those of two other football-related outbreaks (5) and published reports linking higher BMI with a range of infections, including skin infections (6). The possibility that higher BMI is confounded by player positions (e.g., lineman) involving heavier players and more frequent contact is not supported by the data, which found no differences by player position. Evaluating player position in general is statistically problematic because sample sizes vary substantially by position on most football rosters. The findings in this report are subject to at least two limitations. First, the small number of cases reduced the precision of the point estimates, as reflected in the wide CIs. Second, because players were not interviewed until 3 weeks after the first reported symptom onsets, they might not have been able to accurately recall events, leading to misclassification of players by risk factor. High school football programs might be able to reduce the risk for MRSA outbreaks by improving their procedures and facilities to promote optimal player hygiene, particularly during training camps. Improvements might include providing a towel service and collecting used towels from players on a daily basis. Skin injuries should be monitored closely by coaches and trainers, rather than by players alone. Living arrangements might be modified so that players are not living in close quarters for extended periods. Education on SSTI identification, prevention, and intervention might be included as a standard component of football training camps. Acknowledgments This report is based, in part, on contributions by M Marx, PhD, J Nguyen, MPH, M Layton, MD, Bur of Communicable Disease; L Thorpe, PhD, K Konty, PhD, Div of Epidemiology; T Matte, MD, Div of Environmental Surveillance and Policy, New York City Dept of Health and Mental Hygiene. J Magri, MD, Office of Workforce and Career Development, CDC. References
* Additional information available at http://www.cdc.gov/nccdphp/dnpa/healthyweight/assessing/bmi/childrens_bmi/about_childrens_bmi.htm. Figure 1
All MMWR HTML versions of articles are electronic conversions from typeset documents. This conversion might result in character translation or format errors in the HTML version. Users are referred to the electronic PDF version (http://www.cdc.gov/mmwr) and/or the original MMWR paper copy for printable versions of official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to [email protected].Date last reviewed: 1/28/2009 |
|||||||||
|