|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
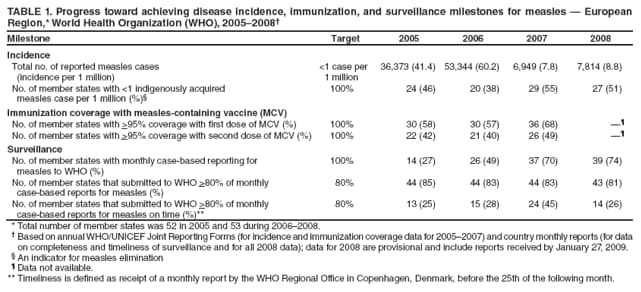
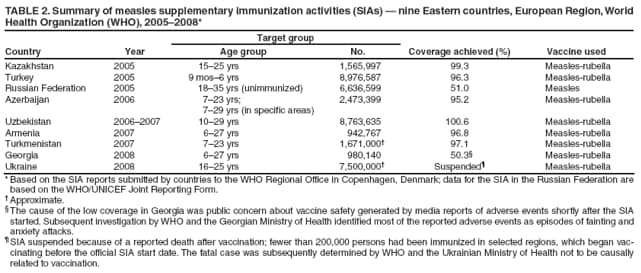
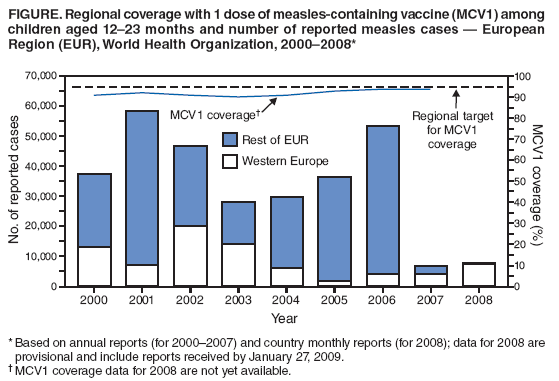
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail. Progress Toward Measles Elimination --- European Region, 2005--2008In 2002, the World Health Organization (WHO) Regional Committee for the European Region (EUR)* revised earlier targets to eliminate indigenous measles and achieve rubella control (1) by resolving to 1) eliminate both diseases in EUR member states by 2010, using a combination of routine and supplementary immunization strategies,† and 2) monitor progress toward this goal through improved surveillance (2). This report summarizes progress toward measles elimination during 2005--2008 and updates a previous report from 2005 (3). In 2005 and 2006, large-scale outbreaks occurred in the eastern EUR member states. However, in 2007 and 2008, overall measles incidence in EUR declined to a historic low of <10 cases per 1 million population, with the majority of cases reported from Western Europe. During 2005--2007, routine vaccination coverage with 1 dose of measles-containing vaccine (MCV) among children aged 12--23 months in EUR reached a high of 93%--94%, up from 90%--91% during 2000--2004. Nevertheless, two major challenges to measles elimination remain: 1) suboptimal vaccination coverage in many countries, which has led to continued outbreaks and the resurgence of indigenous measles in some Western European countries, and 2) setbacks with implementation of supplementary immunization activities (SIAs) in Eastern Europe in 2008. Achieving the measles elimination goal by 2010 will require 1) development of approaches to sustain and increase vaccination coverage, 2) promotion of effective outbreak prevention and control measures, and 3) further strengthening of surveillance. Immunization ActivitiesAll 53 countries in EUR have a national, routine, 2-dose MCV schedule. Fifty-one countries use combined measles, mumps, and rubella (MMR) vaccine nationwide; the Russian Federation has introduced MMR vaccine in some regions, and Tajikistan uses monocomponent measles vaccine. On a yearly basis, countries report routine coverage for first and second doses of MCV (MCV1 and MCV2) to WHO. No coverage data are yet available for 2008. Overall, estimated MCV1 coverage among children aged 12--23 months in EUR increased from 90%--91% during 2000--2004 to 93%--94% during 2005--2007 (Figure). EUR targets of >95% coverage for MCV1 and MCV2 were reached in 2007 by 36 (68%) and 26 (49%) countries, respectively (Table 1). MCV1 coverage remained <90% in 10 countries (eight of them in Western Europe), accounting for 24% of the region's total population, and MCV2 coverage was <90% in 10 countries (eight of them in Western Europe), accounting for 21% of the EUR population. In addition, of the 45 countries reporting subnational level data in 2007, 16 (35%) had MCV1 coverage >95% in all provinces. During 2005--2008, nationwide SIAs reaching approximately 27 million persons were implemented in eight countries in eastern EUR where historic weaknesses in immunization programs had created large susceptible populations among adolescents and adults (4) (Table 2). During 2005--2007, SIAs in six countries achieved >95% vaccination coverage among target age groups, whereas 51% coverage was achieved through an SIA in the Russian Federation (Table 2). In 2008, reports of adverse events, which were perceived by the media and some health-care providers to be caused by the measles-rubella vaccine, resulted in the suspension of an SIA in Ukraine and in only 50% SIA coverage in Georgia (Table 2). These adverse events subsequently were determined by WHO and the ministries of health in Ukraine and Georgia not to be caused by the vaccine (WHO, unpublished data, 2009). Some countries with ongoing measles outbreaks promoted vaccination through enhanced health communication and accelerated routine vaccination activities rather than conducting mass campaigns over short periods. For example, in the United Kingdom, approximately 500,000 unimmunized or underimmunized persons aged 1--18 years received MMR vaccine during 2008. During European Immunization Week in April 2008, MMR vaccination was offered along with other vaccines during outreach efforts in 15 of 32 participating countries, reaching approximately 2 million persons. SurveillanceMeasles is a notifiable disease in all 53 EUR member states. All countries report clinically diagnosed measles cases to WHO on a yearly basis. Countries are encouraged to report additional, case-based information (e.g., case confirmation status, age, and vaccination status for individual measles cases) on a monthly basis (5). In 2008, 39 (74%) countries reported monthly data in a case-based format, compared with 14 (27%) countries in 2005 (Table 1); 11 (20%) countries submitted additional information in their monthly reports as aggregate counts, and three (6%) reported annually. The EUR Regional Laboratory Network for measles, which included 48 national laboratories in 2008, provides laboratory support for surveillance (e.g., quality assurance, confirmation of cases, and genotyping of measles viruses circulating in the region). In 2008, the network reported 18,721 specimens tested for measles, of which 3,549 (19%) were positive. In 2007 and 2008, the most commonly isolated genotype of measles virus in EUR was D4, which accounted for >90% of all genotyped viruses. Measles IncidenceDuring 2007 and 2008, the incidence of measles in EUR was substantially lower (7.8 and 8.8 cases per 1 million population, respectively) than during 2005 and 2006 (41.4 and 60.2 cases per 1 million population, respectively) (Table 1, Figure). By comparison, measles incidence in 2002 was 53.3 cases per 1 million. During 2005--2008, the number of countries reporting measles incidence of less than one case per 1 million population (one indicator for measles elimination) ranged from 20 (38%) to 29 (55%) (Table 1). In 2008, a total of 3,575 (46%) reported cases were confirmed by laboratory testing, 952 (12%) were confirmed by epidemiologic link, and 3,287 (42%) were diagnosed clinically. In 2008, of the 7,627 cases with known age and vaccination status, 2,899 (38%) occurred among persons aged >15 years and 6,268 (82%) occurred among unvaccinated persons. During 2005--2008, a total of 120 measles outbreaks (including 17 outbreaks with more than 250 cases) were reported in 28 countries. Large, nationwide, multiyear outbreaks (some of which started as early as in 2004) occurred in Ukraine (46,121 cases during 2005--2007), Romania (8,542 cases during 2004--2007), and Georgia (8,391 cases during 2004--2005). Measles cases during 2005--2006 primarily occurred in Eastern Europe (Figure). However, the proportion of cases from Western Europe increased from 6% (n = 5,524) during 2005--2006 to 57% (n = 3,933) in 2007 and 95% (n = 7,436) in 2008, when cases occurred primarily in Austria, France, Germany, Israel, Italy, Spain, Switzerland, and the United Kingdom. Measles deaths generally are underreported; during 2005--2008, a total of 25 deaths were reported (14 in 2005, 10 in 2006, and one in 2008), compared with 27 deaths during 2001--2004. Consistent with the increase in the proportion of measles cases from Western European countries, where measles patients are not routinely hospitalized, the proportion of hospitalizations among patients with reported cases declined from 47% in 2005 to 17% in 2008. Reported by: R Martin, PhD, S Deshevoi, MD, D Jankovic, MD, A Goel, D Mercer, PhD, E Laurent, World Health Organization Regional Office for Europe, Copenhagen, Denmark. A Dabbagh, PhD, P Strebel, MD, World Health Organization, Geneva, Switzerland. N Khetsuriani, MD, S Wassilak, MD, A Uzicanin, MD, Global Immunization Div, National Center for Immunization and Respiratory Diseases, CDC. Editorial Note:During 2005--2008, measles incidence in EUR declined to its lowest level to date. This decline was attributable to high vaccination coverage achieved through 2-dose MCV routine vaccination schedules and implementation of SIAs. In addition, surveillance has been strengthened by expanding case-based reporting and laboratory testing. However, measles outbreaks continued to occur because of 1) past weaknesses in immunization programs, which resulted in large, susceptible, young adult populations in eastern EUR (4) and some Western European countries, and 2) limited access to health-care services for certain minority groups throughout the region (e.g., the Roma populations). The decline in measles cases in Eastern Europe largely is attributed to improved routine coverage with MCV and successful SIAs. However, in countries where SIAs have not been implemented successfully, the reduction of cases might represent a post-outbreak decline, reflecting the cyclical nature of measles. Since 2007, as the outbreaks in eastern parts of EUR subsided, measles resurgence occurred in some Western European countries because of persistent suboptimal coverage with MCV and problems with vaccine acceptance (6,7). Ongoing transmission in Western Europe has been linked to multiple introductions of measles virus into other regions, including the United States, where indigenous measles has been eliminated (7,8). Belief systems have become the principal barrier to vaccinating children in Western Europe, resulting in decreased MCV coverage in many countries (6,7,9). Certain groups are rejecting vaccination because of philosophic or religious beliefs (6,7). In addition, certain parents, influenced by antivaccine movements and negative media reports, are choosing not to vaccinate their children or delay vaccination because of safety concerns. Recent measles cases in Western Europe occurred primarily among unimmunized or underimmunized persons from these subgroups (6,7). Unsubstantiated concerns about vaccine safety and quality also have adversely affected recent SIAs in Ukraine and Georgia. Reaching the measles elimination goal by the target date of 2010 will require high-level political commitment to increase and sustain at high levels 2-dose MCV coverage among children and, where necessary, implement SIAs to reduce measles susceptibility among older cohorts. To reverse decreases in MCV coverage in some areas, trust in immunization by the general public must be restored and maintained. European Immunization Week, held annually in April, provides an opportunity to actively communicate the benefits and risks of immunization and advocate for the protection of children. Achieving measles elimination also requires the continued education of public health professionals and health-care providers, focusing on highlighting the distinction between coincidental and causally related adverse events after vaccination. Unlike in the United States, regulations related to immunization (e.g., school entry requirements) are minimal or nonexistent in many EUR countries (7). Therefore, health professionals should be educated on how to guide parents who have questions and concerns about immunization. To monitor progress toward measles elimination more effectively, surveillance needs to be strengthened through adoption of revised WHO regional surveillance guidelines that 1) are adapted to overall lower measles incidence levels and 2) emphasize the importance of laboratory confirmation, case-based reporting, coordination between laboratory and epidemiologic components, and use of standardized performance indicators. Advocacy with member states to improve measles surveillance also is important. When outbreaks occur, International Health Regulations§ provide a mechanism to alert other member states and limit further transmission. The findings in this report are subject to at least four limitations. First, measles cases might be underreported overall and variably among EUR countries. Second, comparisons between countries are difficult because of this underreporting and because of variations in reporting cases by confirmation status (some countries report only confirmed cases) and the extent of laboratory testing. Third, 2008 data are provisional because of delayed reporting and are based on monthly reports because countries submit final annual reports later in the year. Finally, a regionally standardized definition of measles outbreaks does not exist. Measles elimination in EUR is achievable, as demonstrated by countries that have maintained high vaccination coverage and have been free of indigenous measles for several years (e.g., Finland) (7,10). However, suboptimal MCV coverage, which has resulted in continued transmission of measles virus and increasing numbers of cases in certain parts of EUR, increases the likelihood of future outbreaks and threatens to delay measles elimination. These threats need to be urgently addressed to sustain the gains and reach the goal of measles elimination in EUR by 2010. Acknowledgments This report is based, in part, on contributions by immunization program staff members in all 53 EUR member states. References
* Included 53 member states in 2008: Andorra, Austria, Belgium, Denmark, Finland, France, Germany, Greece, Hungary, Iceland, Ireland, Israel, Italy, Luxembourg, Monaco, Netherlands, Norway, Portugal, San Marino, Spain, Sweden, Switzerland, and the United Kingdom (grouped for this report as Western European), and Albania, Armenia, Azerbaijan, Belarus, Bosnia and Herzegovina, Bulgaria, Croatia, Cyprus, Czech Republic, Estonia, Georgia, Kazakhstan, Kyrgyzstan, Latvia, Lithuania, Malta, Montenegro, Poland, Republic of Moldova, Romania, Russian Federation, Serbia, Slovakia, Slovenia, Tajikistan, The former Yugoslav Republic of Macedonia, Turkey, Turkmenistan, Ukraine, and Uzbekistan (grouped for this report as Eastern European). Estimated population of EUR in 2006: 887.3 million. † Supplementary immunization activities (SIAs) increase population immunity by immunizing large numbers of susceptible persons in a short period. SIAs aimed at achieving >95% vaccination coverage among the targeted age groups are recommended for all EUR countries with susceptible cohorts older than the age appropriate to receive the second routine dose or with inadequate first- or second-dose coverage. Three types of SIAs are used in EUR: 1) catch-up campaigns (i.e., one-time national campaigns targeting multiple cohorts in whom susceptible persons have accumulated); 2) follow-up campaigns (i.e., national campaigns conducted every 3--5 years to reach children who were not targeted by the previous mass campaign); and 3) focal campaigns (i.e., campaigns targeting children who have missed routine vaccination and previous mass campaigns in specific, geographically limited areas) (2). § Additional information available at http://www.who.int/csr/ihr. Table 1
All MMWR HTML versions of articles are electronic conversions from typeset documents. This conversion might result in character translation or format errors in the HTML version. Users are referred to the electronic PDF version (http://www.cdc.gov/mmwr) and/or the original MMWR paper copy for printable versions of official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to [email protected].Date last reviewed: 2/19/2009 |
|||||||||
|