|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
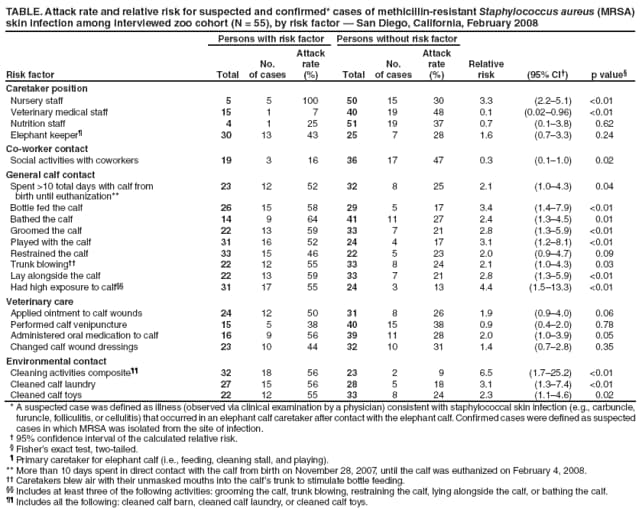
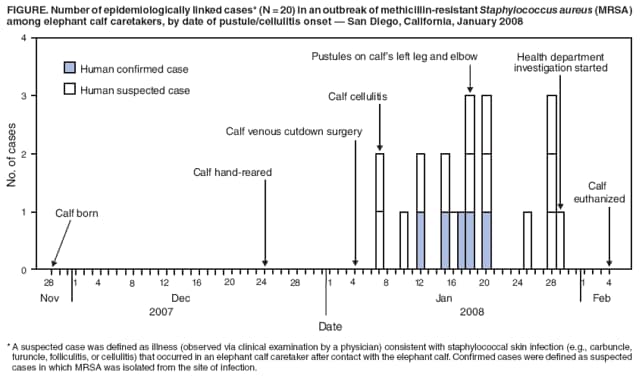
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail. Methicillin-Resistant Staphylococcus aureus Skin Infections from an Elephant Calf --- San Diego, California, 2008Methicillin-resistant Staphylococcus aureus (MRSA) infections are a major cause of human skin and soft tissue infections in the United States (1). MRSA colonization and infection also have been observed in turtles, bats, seals, sheep, rabbits, rodents, cats, dogs, pigs, birds, horses, and cattle (2--8), and MRSA infections with an epidemiologic link to animal contact have been reported in veterinary personnel, pet owners, and farm animal workers (5,7,8). On January 29, 2008, the County of San Diego Health and Human Services Agency was notified of skin pustules on an African elephant (Loxodonta africana) calf and three of its caretakers at a zoo in San Diego County. After each of these infections (including the calf's infection) was laboratory confirmed as MRSA, an outbreak investigation and response was initiated by the zoo and the agency. This report summarizes the results of that investigation, which identified two additional confirmed MRSA infections, 15 suspected MRSA infections, and three MRSA-colonized persons (all among calf caretakers), and concluded that infection of the elephant calf likely came from a colonized caretaker. This is the first reported case of MRSA in an elephant and of suspected MRSA transmission from an animal to human caretakers at a zoo. Recommendations for preventing MRSA transmission in zoo settings include 1) training employees about their risks for infection and the recommended work practices to reduce them; 2) performing proper hand hygiene before and after animal contact; 3) using personal protective equipment (PPE) when working with ill or infected animals, especially during wound treatment; and 4) cleaning and disinfecting contaminated equipment and surfaces. The African elephant calf was born in captivity on November 28, 2007 (approximately 2 weeks before its anticipated due date), with a low birthweight. Because of loss of milk by the mother, the calf was separated from its mother on December 24 and hand-reared by zoo caretakers in an individual stall of the African elephant enclosure. Caretakers ranged in age from 24 to 59 years. Twenty-four--hour care was provided at the enclosure by nursery staff (who typically worked in the nursery building, where other young animals are raised) and elephant keepers, with intermittent visits by nutritionists, veterinarians, and veterinary technicians. Because of poor weight gain with bottle feeding, a central venous line was attempted by venous cutdown in the right neck for total parenteral nutrition on January 4, 2008. Three days later, on January 7, the calf developed cellulitis at the sutured surgical site, followed by pustules on the left leg and elbow on January 18. Swab samples obtained from the calf's left elbow and left leg on January 21 were laboratory confirmed as MRSA on January 26. After topical, oral, and intravenous antibiotics were administered, the calf's wounds healed. Nevertheless, the calf failed to thrive and was euthanized on February 4. Necropsy revealed Enterococcus spp. vegetative endocarditis but no MRSA bacteremia. During January 12--17, three of the calf's caretakers reported cutaneous pustules. Swab samples were obtained from the three caretakers on January 21, and all were laboratory confirmed as MRSA on January 26. An investigation was initiated on January 29. A suspected case was defined as illness (observed via clinical examination by a physician) consistent with staphylococcal skin infection (e.g., carbuncle, furuncle, folliculitis, or cellulitis) that occurred in an elephant calf caretaker after contact with the elephant calf. Confirmed cases were defined as suspected cases in which MRSA was isolated from the site of infection. A case of MRSA colonization was defined as isolation of MRSA from a nasal culture in an elephant calf caretaker. A retrospective cohort study of all caretakers was conducted using a self-administered questionnaire during February 1--15. The cohort included all zoo staff members who had direct contact with the elephant calf or its immediate environment, including the enclosure and animal hospital (N = 55). Investigators conducted environmental sampling and chart reviews of the elephant calf's medical record and the on-site staff medical log. To assess MRSA colonization, investigators obtained rectal and trunk cultures from the 11 other African elephants at the zoo and nasal cultures from 53 (96%) of elephant calf caretakers. All MRSA isolates were characterized by pulsed-field gel electrophoresis (PFGE) and other methods at the San Diego Public Health Laboratory, the California Microbial Disease Laboratory, and CDC. Review of the on-site staff medical log showed no cellulitis or skin infections among caretakers from November 28, 2007 to January 6, 2008. During January 7--February 4, a total of 20 MRSA wound infections (five confirmed and 15 suspected cases) were identified among 20 of the calf's caretakers (attack rate [20 / 55] = 36%) (Figure). The 20 cases occurred in 13 elephant keepers, five nursery staff members (who were specialty trained in hand-rearing), one veterinarian, and one nutritionist. No underlying diseases or risk factors for MRSA were identified among infected caretakers. Most infections were mild, with small pustules; none required surgical incision and drainage, intravenous antibiotics, or hospitalization. Lesions occurred along uncovered skin surfaces, especially the hands, forearms, and wrists; four patients developed lesions in areas with preexisting cuts or scrapes. In three cases, patients were prescribed oral antibiotics, including clarithromycin, doxycycline, azithromycin, and ciprofloxacin, for their infections. The other 11 African elephants in the herd, including the calf's mother, tested negative for MRSA colonization. Analysis of PGFE results revealed that eight isolates (two wound isolates and one rectal isolate from the elephant calf, wound isolates from three caretakers, and nasal isolates from two caretakers) were USA300, the MRSA PFGE type most commonly identified in community-associated MRSA infections in the United States. Another employee nasal isolate was USA500, a less common MRSA strain. Three employee nasal specimens were positive, yielding a 5.7% MRSA carriage rate. In univariate analysis, calf nursery staff members were three times more likely (relative risk [RR] = 3.3) to be infected compared with other staff members, whereas being a member of the veterinary staff (RR = 0.1) was protective (Table). Other significant risk factors included playing with the calf (RR = 3.1), bottle feeding the calf (RR = 3.4), bathing the calf (RR = 2.4), grooming the calf (RR = 2.8), lying alongside the calf (RR = 2.8), administering oral medication to the calf (RR = 2.0), spending >10 total days with the calf from birth until euthanization (RR = 2.1), and cleaning the calf laundry (RR = 3.1) or calf toys (RR = 2.3). In a logistic regression model of the variables determined to be significant in the univariate analysis (p<0.05), only activities requiring high exposure to the calf (i.e., at least three of the following activities: grooming the calf, bathing the calf, trunk blowing,* playing with the calf, or lying alongside the calf) (adjusted odds ratio [aOR] = 7.8) or cleaning the calf toys and laundry (aOR = 6.5) remained significant after backward elimination. Investigators performed environmental sampling of the calf's immediate environment on February 1. Surfaces sampled included cage doors in the elephant enclosure, countertops in the animal hospital, and the floor of an animal transport van. All the environmental samples, which were collected after bleach disinfection, were negative for MRSA. Reported by: D Janssen, DVM, N Lamberski, DVM, Wild Animal Park, San Diego Zoo; G Dunne, DVM, Office of the County Veterinarian, San Diego County; M Ginsberg, MD, C Roach, S Tweeten, PhD; San Diego County Health and Human Svcs Agency, California. R Gorwitz, MD, Div Healthcare Quality Promotion, S Waterman, MD, Div Global Migration and Quarantine, National Center for Preparedness, Detection, and Control of Infectious Diseases; D Bensyl, PhD, Office of Workforce and Career Development; D Sugerman, MD, EIS Officer, CDC. Editorial Note:MRSA skin infections have become a substantial community public health problem in recent years, and outbreaks of MRSA skin infections have been reported in various animal settings (e.g., veterinary offices, animal farms, and the homes of pet owners) (5,7,8). However, transmission of MRSA from an animal to human caretakers at a zoo has not been reported previously. MRSA infection in zoo elephants also has not been reported previously. The investigation determined that the elephant calf likely acquired its MRSA infection from a colonized human caretaker. The calf developed cellulitis on January 7, after exposure to caretakers who were later found to be colonized with MRSA of the same strain. The USA300 strain identified among the calf's caretakers is the most common type of human community-associated MRSA but it has never been reported de novo from animals. No MRSA colonization or skin infections were found in the other African elephants with which the calf shared living space. The results of this investigation suggest that transmission also occurred from the calf to human caretakers, resulting in an outbreak of MRSA skin infections. Although transmission from caretaker to caretaker or transmission through contact with equipment surfaces cannot be ruled out, several factors support likely transmission directly from the calf. Veterinary staff members more often used PPE when handling the calf and were less likely to acquire MRSA than nursery staff or elephant keepers. Among caretakers, activities involving direct contact with the calf were associated with infection. The caretakers also did not report sharing personal items (e.g., towels, uniforms, bar soap, or razors), which has been implicated in other human-to-human MRSA outbreaks. Infected staff members kept their lesions covered. MRSA in animals can be of human or animal origin. MRSA strains isolated from household pets typically are prevalent human strains that likely were acquired from human contacts (3,4,8). In contrast, MRSA strains most commonly identified in horses and pigs are not prevalent human strains and might represent strains that are animal-adapted or of animal origin. Although animals likely are not a major source of MRSA acquisition for humans, transmission of MRSA from infected or colonized animals to humans is possible via contact with contaminated body fluids. Veterinary personnel and others who have direct contact with animals that have a high prevalence of colonization (e.g., pigs) might be at increased risk for MRSA acquisition (5). Surveys of MRSA colonization in veterinary personnel have indicated colonization rates ranging from 4.6% to 18.0%, compared with a colonization rate of 1.5% in the general U.S. population (4,9,10). Although MRSA has been cultured from veterinary hospitals (4), only one report documents MRSA skin infections in veterinary personnel acquired from an animal. In that report, workers had close animal contact with a neonatal horse that was colonized with MRSA (8). The National Association of State Public Health Veterinarians has published recommendations for standard infection control precautions to be implemented by veterinary personnel in its Compendium of Veterinary Standard Precautions: Zoonotic Disease Prevention in Veterinary Personnel.† According to these recommendations, hygiene is critical to preventing disease transmission from animals to humans. Hands should be washed with running water and soap before and after handling animals. The use of hand sanitizer is inadequate when gross contamination with organic debris is present. Before handling or treating animals, caretakers should don 1) dedicated clothing or protective outerwear; 2) gloves, if touching blood, body fluids, secretions, excretions, mucous membranes, or non-intact skin (including wounds); and 3) face protection, if splashes or sprays might occur. During a MRSA cluster or outbreak, wound cultures of animals and humans are indicated, especially if skin pustules are present. In addition, training employees working with animals about their risk for MRSA infection, recommended work practices, and the proper care and use of PPE is important in reducing their risk for exposure to MRSA and other zoonoses. In addition, cleaning equipment and surfaces with detergent-based cleaners or Environmental Protection Agency (EPA)-registered detergent-disinfectants, followed by disinfection of contaminated surfaces, is important to remove MRSA from the environment. Acknowledgments This report is based, in part, on contributions by C Peter, PhD, M Victoria, G Washabaugh, MPH, R Patel, MS, R Jansen, and P Temprendola, County of San Diego Public Health Laboratory; W Probert, PhD, and J O'Connell, Microbial Disease Laboratory Br, California Dept of Public Health; and G Fosheim, MPH, Div Healthcare Quality Promotion, National Center for Preparedness, Detection, and Control of Infectious Diseases, CDC. References
* Caretakers blew air with their unmasked mouths into the calf's trunk to stimulate bottle feeding. † Available at http://www.nasphv.org/Documents/VeterinaryPrecautions.pdf. Table
All MMWR HTML versions of articles are electronic conversions from typeset documents. This conversion might result in character translation or format errors in the HTML version. Users are referred to the electronic PDF version (http://www.cdc.gov/mmwr) and/or the original MMWR paper copy for printable versions of official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to [email protected].Date last reviewed: 3/5/2009 |
|||||||||
|