
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail.
Progress Toward the 2012 Measles Elimination Goal --- Western Pacific Region, 1990--2008
In 2003, the World Health Organization (WHO) Regional Committee of the Western Pacific Region (WPR) formally declared a measles elimination goal* (1), and in 2005, the committee established a target date of 2012 for regional measles elimination (2). Key strategies recommended by WHO for achievement of measles elimination include 1) very high (≥95%) vaccination coverage with 2 doses of measles-containing vaccine (MCV1 and MCV2) through routine vaccination and/or supplemental immunization activities (SIAs)†; 2) high-quality case-based§ measles surveillance; and 3) access to an accredited measles laboratory network for testing of suspected measles cases and identification of measles virus genotypes. This report describes progress toward measles elimination in the WPR through 2008. Measles likely has been eliminated or nearly eliminated in 24 of the 37 countries and areas in the WPR (referred to in this report as countries). However, large numbers of measles cases continue to be reported from several countries. During 2008, a total of 131,441 confirmed measles cases (98.4 per million population) were reported from China and 11,015 cases (86.1 per million population) from Japan, two countries that account for 82% of the region's population and >97% of its confirmed measles cases. Intensified efforts by WPR countries, particularly China and Japan, will be required to achieve the 2012 goal.
Routine Vaccination
Among the 37 countries in the WPR,¶ 36 report administrative and, if available, survey data and their estimates of vaccination coverage among infants annually to WHO and the United Nations Children's Fund (UNICEF). The other country, Pitcairn Islands (with a population of approximately 50 persons), does not report data to WHO/UNICEF and is not included in this report. Based on these and other data available from published literature, WHO/UNICEF make their estimates of actual vaccination coverage for WHO member states (3). Regional MCV1 coverage by year was determined using WHO/UNICEF estimates of vaccination coverage and, when these estimates were not available (such as in certain areas of member states), coverage was determined using country estimates and weighting by country population size. Because China includes 75% of the region's population, its data are reported separately.
The history of measles elimination in the WPR can be divided into three periods: the period of measles control (1990--1995), the period of accelerated measles control (1996--2002), and the period of measles elimination (from 2003 to the present).** This report uses these three periods to describe progress toward measles elimination. Among the 35 WPR countries reporting (i.e., all WPR countries except China and Pitcairn Islands), mean regional MCV1 coverage was 80.8% during the period of measles control (1990--1995), increased to 89.0% during the period of accelerated control (1996--2002), and reached 91.6% during the period of measles elimination (2003--2008) (Figure). The WHO-estimated mean MCV1 coverage in China was 85.5%, 84.4%, and 88.8% during the same periods, but increased from 85% in 2003 to 94% in 2007 (data were not available for 2008). Among 36 countries (including China) reporting dose schedules in 2008, MCV1 was scheduled for administration at age <9 months in two (5.6%) countries, age 9 months in five (13.9%) countries,†† age 12 months in 26 (72.2%) countries, and age 15 months in three (8.3%) countries (Table 1).
Before 2003, few countries reported MCV2 coverage to WHO/UNICEF. During 2003--2008 (the period of measles elimination), the number of reporting countries varied annually from 16 to 24. These country estimates were used to determine the regional weighted MCV2 coverage by year. Mean MCV2 coverage (excluding China) during 2003--2008 was 84.2%. China's reported MCV2 coverage ranged from 84.1% to 96.4% during 2003--2007, with a mean of 92.5%. As of 2008, among the 30 countries that had scheduled administration of MCV2, 12 countries (40%) administered MCV2 at age 13--23 months, three (10%) at age 2 years, eight (26.7%) at age 4 years, one (3.3%) at age 5 years, five (16.7%) at age 6 years, and one (3.3%) at age 7 years.
Supplemental Immunization Activities
During the periods of measles accelerated control (1996--2002) and elimination (2003--2008), many countries conducted SIAs. Approximately 94.4 million children and adolescents in 28 WPR countries (excluding China) were vaccinated through SIAs. In China, SIAs during 2003--2008 reached approximately 101 million children and adolescents in 14 provinces (Table 2). SIA coverage generally has been higher since the region established an elimination goal. Excluding China, SIAs reached 87% of the target population in 25 countries during the period of measles accelerated control (1996--2002) and increased to 94% of the target population in 28 countries during the period of measles elimination (2003--2008). In China, SIA coverage by year during 2003--2008 was 95%--99%, with the exception of 2005. SIAs in the WPR were frequently used to provide vitamin A, oral polio vaccine, and anti-helminthics in addition to MCV.
Surveillance Activities
By 2008, all countries in WPR conducted case-based measles surveillance, supported by the measles and rubella laboratory network (LabNet), a network of 382 laboratories. Standard indicators for high-quality measles surveillance include 1) two or more suspected measles cases per 100,000 discarded as nonmeasles; 2) ≥80% of suspected measles cases with adequate investigations (i.e., investigations within 48 hours of rash onset that include all essential data elements); 3) ≥80% of suspected measles cases with clinical specimens collected within 28 days of rash onset; and 4) ≥80% of specimens with laboratory results available within 7 days after receipt in the laboratory (4,5). In 2008, the region's indicator achievements were 1.6, 47%, 62%, and 76%, respectively (6).
Genotypes of endemic measles virus identified among measles patients in the WPR since 2007 include D5 in Japan, D9 in Lao People's Democratic Republic, Malaysia, and New Zealand, and H1 in China, Hong Kong (China, Special Administrative Region [SAR]), and Vietnam. In addition, genotypes B3, D4, D8, and G3 were identified among measles patients; some of these genotypes were imported from other regions.
Monitoring Measles Incidence
Suspected measles cases can be confirmed by the laboratory (e.g., presence of anti-measles immunoglobulin M (IgM) antibodies in clinical specimens), by epidemiologic linkage to another confirmed case, and by clinical criteria (i.e., cases that satisfy the measles clinical case definition§§ and cannot be discarded as nonmeasles by laboratory or other criteria). Since 1990, the largest annual number of measles cases reported from the WPR (excluding China) was 106,172 (255.6 per million population) in 2000. In 2008, excluding China, 14,724 cases (32.6 per million) were reported, a decrease of 86%. (Figure). China reported 131,441 measles cases (98.4 per million) in 2008. A large outbreak in Japan resulted in over 18,000 (140.7 per million) reported cases in 2007 and 11,015 (86.1 per million) in 2008 (7). Excluding China and Japan, 3,564 measles cases (11.8 per million) were reported from the rest of the region in 2008. In descending order, the majority of these were from Cambodia (1,765), Philippines (880), Malaysia (333), Vietnam (258), and Lao People's Democratic Republic (117) (6).
Country Measles Elimination Status
Several WPR countries have achieved or nearly achieved the indicator targets suggesting substantial progress toward measles elimination. In 2006, Republic of Korea declared measles eliminated after having successfully implemented WHO-recommended strategies (8). In Australia, measles incidence has ranged from 0.5 to 6.1 per million since 2002; case investigations and genotype analysis indicated that the majority of these cases were imported or import-related (9). Reported routine vaccination coverage in Australia is high; however, sensitivity of suspected measles reporting is uncertain because surveillance performance is not monitored nationally. In Macau (China, SAR), fewer than five cases per year have been reported since 2001, corresponding to an annual incidence of zero to 8.3 per million; case investigations and genotype analysis of specimens during this period indicate that most of these cases were imported. In 2008, surveillance performance in Macau (China, SAR) satisfied all key indicator targets. All 21 Pacific island countries have reported zero measles cases in 2007 and 2008.
Reported by: Unit of Expanded Programme on Immunization, World Health Organization Regional Office of the Western Pacific, Manila, Philippines. Vaccines and Biologicals Dept, World Health Organization, Geneva, Switzerland. Global Immunization Div, Div of Viral Diseases, National Center for Immunization and Respiratory Diseases, CDC.
Editorial Note:
The WPR has made progress toward the 2012 regional goal of measles elimination as evidenced by increasing routine and SIA measles vaccination coverage and declining measles incidence in the presence of improving case-based, laboratory-supported measles surveillance systems. Nevertheless, in the region overall and in many countries, surveillance does not yet meet elimination standards, leading to underreporting or misclassification of cases. Moreover, countries such as Cambodia, Lao People's Democratic Republic, Papua New Guinea, and others face challenges to achieving the 2012 goal because of general weaknesses of public health services that result in low routine vaccination coverage. In such countries, continuing periodic SIAs to attain high MCV coverage while working to strengthen routine vaccination systems will be critical to achieve the goal. Ensuring that all suspected measles cases are identified, reported and fully investigated by providing training, adequate operational costs, and laboratory support is urgently needed to monitor progress toward and ultimately validate achievement of measles elimination. Monitoring of circulating measles genotypes also is needed to validate interruption of endemic measles virus transmission.
Challenges also exist in China and Japan, which together accounted for 82% of the region's population and more than 97% of its reported measles cases in 2008. Both countries have made renewed commitments and plans for achieving the 2012 regional goal. China has strengthened routine measles vaccination by scheduling earlier administration of MCV2 (at age 18--24 months instead of 7 years), providing incentives to health-care workers for immunizing children, and requiring proof of receiving 2 doses of measles vaccine at school entry. Japan is implementing a national measles elimination plan established in December 2007 (7).
Efforts to eliminate measles help strengthen health systems and reduce child mortality from pneumonia, diarrhea, and micronutrient deficiencies that occur after measles infection, thereby helping to achieve the United Nations' Millennium Development Goal No. 4 (to reduce by two thirds, from 1990 to 2015, the mortality rate in children aged <5 years).¶¶ To achieve measles elimination and Millennium Development Goal No. 4, intensified and innovative efforts will be required by WPR countries and measles elimination partners*** to implement recommended strategies and target potentially new high-risk groups (e.g., young adults) revealed by epidemiologic analysis of surveillance data.
References
- World Health Organization. Fifty-fourth session of the Regional Committee for the Western Pacific. Summary record of the fifth meeting. Resolution WPR/RC54.R3. Expanded programme on immunization: measles and hepatitis B. Manila, Philippines: World Health Organization; 2003. Available at http://www.wpro.who.int/rcm/en/archives/rc54/rc_resolutions/wpr_rc54_r03.htm.
- World Health Organization. Fifty-sixth session of the Regional Committee for the Western Pacific. Summary record of the eighth meeting. Resolution WPR/RC56.R8. Measles elimination, hepatitis B control, and poliomyelitis eradication. Manila, Philippines: World Health Organization; 2005. Available at http://www.wpro.who.int/nr/rdonlyres/185af547-3c1a-4510-96f2-94d4402355e9/0/rc56_r08.pdf.
- World Health Organization. WHO-UNICEF estimates of MCV coverage. Available at http://www.who.int/immunization_monitoring/en/globalsummary/timeseries/tswucoveragemcv.htm.
- World Health Organization Regional Office of the Western Pacific. Monitoring measles surveillance and progress towards measles elimination. Measles Bulletin 2007;1:1--3. Available at http://www.wpro.who.int/nr/rdonlyres/7be6353c-7d82-4368-a300-57db3f38148d/0/measbulletinissue13.pdf.
- World Health Organization Regional Office of the Western Pacific. Field guidelines for measles elimination. Geneva, Switzerland: World Health Organization; 2004. Available at http://www.wpro.who.int/nr/rdonlyres/0f24b92e-ae2c-4c9b-b73b-e16acb833c35/0/fieldguidelines_for_measleselimination.pdf.
- World Health Organization Regional Office of the Western Pacific. Tables 2a and 2b. Measles Bulletin 2009;3:3--4 Available at http://www.wpro.who.int/nr/rdonlyres/fe4ce60a-5418-4a39-a666-0ce86aa4465e/0/measbulletinvol3issue1.pdf.
- CDC. Progress toward measles elimination---Japan, 1999--2008. MMWR 2008;57:1049--52.
- CDC. Elimination of measles---South Korea, 2001--2006. MMWR 2007;56:304--7.
- Heywood AE, Gidding HF, Riddell MA, et al. Elimination of endemic measles transmission in Australia. Bull World Health Organ 2009;87:64--71.
* Measles elimination is defined as the absence of endemic measles virus transmission.
† SIAs generally are carried out in two stages: 1) an initial nationwide catch-up SIA usually targets all children aged 9 months--14 years, followed by 2) periodic follow-up SIAs targeting all children born since the last SIA.
§ Data collected and reported on individual cases rather than in aggregate form.
¶ The WPR includes 37 countries and areas: Australia, Brunei Darussalam, Cambodia, China, Hong Kong (China, Special Administrative Region [SAR]), Macau (China, SAR), Japan, Malaysia, Mongolia, New Zealand, Lao People's Democratic Republic, Papua New Guinea, Philippines, Republic of Korea, Singapore, Vietnam, and 21 Pacific island countries and areas including American Samoa, Commonwealth of the Northern Marianas Islands, Cook Islands, Federated States of Micronesia, Fiji, French Polynesia, Guam, Kiribati, Marshall Islands, New Caledonia, Niue, Nauru, Pitcairn Islands, Samoa, Solomon Islands, Tokelau, Tonga, Tuvalu, Vanuatu, and Wallis and Futuna.
** Measles control aims to reduce the number of measles cases and deaths by 1) high (≥90%) coverage with a single dose of measles vaccine; 2) measles surveillance in every district with aggregate data reporting; and 3) case management with vitamin A and treatment for measles complications. Accelerated measles control aims to prevent measles outbreaks by providing a second dose of measles vaccine, often through campaigns, and conducting active measles surveillance with laboratory confirmation of suspected outbreaks. Measles elimination aims to interrupt transmission of measles by 1) very high (≥95%) coverage with 2 doses of measles vaccine through routine vaccination systems or SIAs; 2) high-quality case-based surveillance; and 3) access to an accredited measles laboratory network for confirmation of suspected measles cases and identification of measles genotypes.
†† Papua New Guinea also provides a supplementary dose of MCV at age 6 months.
§§ The WHO-recommended clinical case definition of measles is illness in a person of any age with fever, rash, and at least one of the following: cough, coryza, or conjunctivitis.
¶¶ Additional information available at http://www.un.org/millenniumgoals.
*** Current partners providing financial and technical support for measles elimination in the WPR include American Red Cross, Australian Agency for International Development, Government of Korea, Government of Japan, New Zealand Agency for International Development, CDC (United States), UNICEF, United Nations Foundation, and WHO.
FIGURE. Number of reported measles cases and coverage with first dose of measles-containing vaccine (MCV1) --- World Health Organization, Western Pacific Region, 1990--2008*
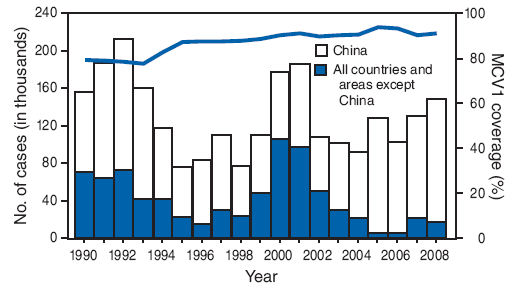
* The history of measles elimination in the Western Pacific Region can be divided into three periods: the period of measles control (1990--1995), the period of accelerated measles control (1996--2002), and the period of measles elimination (from 2003 to the present). Measles control aims to reduce the number of measles cases and deaths by 1) high (≥90%) coverage with a single dose of measles vaccine; 2) measles surveillance in every district with aggregate data reporting; and 3) case management with vitamin A and treatment for measles complications. Accelerated measles control aims to prevent measles outbreaks by providing a second dose of measles vaccine, often through campaigns, and conducting active measles surveillance with laboratory confirmation of suspected outbreaks. Measles elimination aims to interrupt transmission of measles by 1) very high (≥95%) coverage with 2 doses of measles vaccine through routine vaccination systems or SIAs; 2) high-quality case-based surveillance; and 3) access to an accredited measles laboratory network for confirmation of suspected measles cases and identification of measles genotypes.
Alternative Text: The figure above shows the number of reported measles cases and coverage with first dose of measles-containing vaccine (MCV1) from 1990 through 2008 for the Western Pacific Region (WPR), as reported by the World Health Organization. The history of measles elimination in the WPR can be divided into three periods: the period of measles control (1990-1995), the period of measles accelerated control (1996-2002), and the period of measles elimination (from 2003 to the present). Among the 35 WPR countries reporting (i.e., all WPR countries except China and Pitcairn Islands), mean regional MCV1 coverage was 80.8% during the period of measles control (1990-1995), increased to 89.0% during the period of accelerated control (1996-2002), and reached 91.6% during the period of measles elimination (2003-2008).
Use of trade names and commercial sources is for identification only and does not imply endorsement by the U.S. Department of
Health and Human Services. |
All MMWR HTML versions of articles are electronic conversions from typeset documents. This conversion might result in character translation or format errors in the HTML version. Users are referred to the electronic PDF version (http://www.cdc.gov/mmwr) and/or the original MMWR paper copy for printable versions of official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices.
**Questions or messages regarding errors in formatting should be addressed to [email protected].Date last reviewed: 6/25/2009