
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail.
State Medicaid Coverage for Tobacco-Dependence Treatments --- United States, 2007
The prevalence of tobacco use among adults in the United States has been reduced by half since the 1960s (1,2). Despite this progress, low-income populations, such as Medicaid enrollees, continue to smoke at substantially higher rates than the general population (33% versus 20%) (1). The Public Health Service's Clinical Practice Guideline (2) and the Partnership for Prevention's Call for ACTTION (3) recommend comprehensive insurance coverage of tobacco-dependence treatments without barriers such as copayments, limitations in duration of treatment, prior authorization, and stepped-care therapy. Healthy People 2010 aims to expand coverage of evidence-based treatments for nicotine dependency to all 51 Medicaid programs (objective 27-8b) (4). To monitor progress toward that objective, in 2007, the Center for Health and Public Policy Studies at the University of California, Berkeley, surveyed all 51 Medicaid programs. This report summarizes the results of that survey, which found that 43 (84%) programs offered coverage for some form of tobacco-dependence treatment to Medicaid enrollees in traditional fee-for-service (FFS) Medicaid, with four Medicaid programs adding coverage since 2006 and 20 programs adding coverage in the past decade. Only two states (New Mexico and New Jersey) reported access to tobacco-dependence treatments without any limitations or restrictions. Of the 25 states covering pharmacotherapy for Medicaid enrollees in both FFS and managed-care organizations (MCOs), only 13 covered the same tobacco-dependence treatments for enrollees in both populations. Research demonstrates that providing access to comprehensive tobacco-dependence treatments increases quit rates. Providing Medicaid coverage for these treatments would ensure that all enrollees can access and benefit from these treatments.
Medicaid coverage of tobacco-dependence treatments has been assessed regularly, since 1998, by the Center for Health and Public Policy Studies at the University of California, Berkeley. Starting in October 2007, designated Medicaid personnel for each program from all 50 states and the District of Columbia were sent a link to an online survey that included 43 questions regarding coverage of clinically effective tobacco-dependence treatments, the year coverage began, and program requirements and limitations. Programs were asked to respond regarding policies in both traditional FFS Medicaid (n = 51) and their contracts with Medicaid MCOs (n = 32).* All Medicaid programs responded with information on both programs; data for MCOs were first collected starting with the 2007 survey. Medicaid program participation in the 2007 survey was 100%. To validate survey responses, Medicaid programs were asked to submit a written copy of their coverage policies for tobacco-dependence treatments. Of the 45 programs that reported offering any coverage in 2007, supporting documentation was obtained for 41 (91%) programs, 28 (62%) with detailed documentation matching their survey responses (six were missing documentation regarding varenicline [Chantix]) and 13 (29%) providing partial benefit information (e.g., documentation for pharmacotherapy but not counseling).
Of the 51 FFS Medicaid programs, 43 (84%) reported coverage for at least one tobacco-dependence treatment (medication and/or counseling); two additional programs (Arizona and Washington) reported coverage for pregnant women only (Table 1). Forty-one (80%) Medicaid FFS programs covered some form of pharmacotherapy: nicotine patches (40 programs), bupropion (Zyban or its generic equivalent) (40 programs), varenicline (Chantix) (38 programs), nicotine gum (37 programs), nicotine nasal spray (33 programs), nicotine inhalers (32 programs), and nicotine lozenges (30 programs). Twenty-six programs (51%) covered tobacco-cessation counseling, with 19 states covering some form of tobacco-cessation counseling for their FFS population and seven states covering counseling services exclusively for pregnant women (Table 1). Among these 26 states, nine states covered group counseling for FFS enrollees, six states covered group counseling for pregnant women only, and 11 states did not cover group counseling. Individual counseling was covered in all but one of the 26 states (Virginia), with 17 covering FFS enrollees and eight providing coverage exclusively to pregnant women. Only four of the 26 states (Kentucky, Oregon, Utah, and West Virginia) covered telephone counseling using Medicaid funds; however, telephone counseling is available to the public for free in every state through quitlines (accessed by dialing 1-800-QUITNOW [784-8669]).
During 2006--2007, two states began covering tobacco-dependence treatments (Idaho† and Wyoming), two states expanded existing coverage beyond pregnant women only (Kentucky and Iowa), and seven states expanded coverage of existing tobacco-dependence treatments. Specifically, in 2007, four states (Arkansas, California, Maine, and Mississippi) added coverage for varenicline (Chantix), Maryland added coverage for individual counseling, Ohio added coverage for nicotine nasal spray, and New Jersey reinstated coverage for all forms of nicotine replacement therapy.§
Data collected over the past decade on Medicaid program coverage of tobacco-dependence treatments indicate an increase in coverage levels (Figure) (5,6). In 1998, 23 Medicaid programs covered some form of tobacco-dependence treatment, with 22 programs covering pharmacotherapy and three programs covering tobacco-cessation counseling. As of 2007, an upward trend in both forms of coverage was observed, with 41 programs covering pharmacotherapy and 19 covering counseling.
In the 2007 survey, Medicaid programs were asked about limitations placed on tobacco-dependence treatment coverage. Of the 43 programs offering coverage for tobacco-dependence treatments to their entire Medicaid FFS populations, 41 placed some form of limit on coverage by requiring copayments (32 states), limiting duration of treatment (25 states), requiring prior authorization (21 states), and requiring enrollment in behavioral modification to gain coverage for pharmacotherapy (13 states). Only two states (New Mexico and New Jersey) did not report having any of these limitations on coverage for tobacco-dependence treatments.
Although the majority of the survey addressed policies related to FFS Medicaid, data also were collected on coverage for tobacco-dependence treatments in Medicaid MCOs. Of the 51 Medicaid programs surveyed, 13 indicated that they did not contract with MCOs, and six programs reported that pharmacotherapy was not included in MCO contracts but was provided by a third party through a "carve out" arrangement.¶ Of the 32 Medicaid programs that contract with MCOs, 13 reported requiring the same tobacco-dependence treatment for their MCOs and FFS populations (Table 2). Four programs required MCOs to cover some of the tobacco-dependence treatments in FFS Medicaid, and two programs (Rhode Island and New York) required more coverage in MCOs than FFS. Thirteen states reported that they did not require coverage of tobacco-dependence treatments in Medicaid MCO contracts. Of these 13 states, six covered tobacco-dependence treatments in FFS Medicaid, and seven did not. Therefore, of the 25 states covering pharmacotherapy for FFS Medicaid that also contracted with Medicaid MCOs, only 13 had the same tobacco-dependence treatment coverage requirements for both populations.
Reported by: SB McMenamin, PhD, HA Halpin, PhD, NM Bellows, PhD, Center for Health and Public Policy Studies, Univ of California, Berkeley. CG Husten, MD, Partnership for Prevention, District of Columbia. A Rosenthal, Office on Smoking and Health, CDC.
Editorial Note:
This report updates previously published data on Medicaid coverage for tobacco-dependence treatments and provides additional information on coverage of tobacco-dependence treatments in Medicaid MCOs (5,6). The number of Medicaid FFS programs covering effective tobacco-dependence treatments has increased over time, from 23 programs in 1998 to 43 in 2007. In addition, although coverage for tobacco-cessation counseling has increased over time, it still lags far behind coverage for pharmacotherapy. Although Medicaid programs are making progress toward the Healthy People 2010 objective (27-8b) (4), only six states cover all of the effective pharmacotherapies and individual and group counseling. To achieve the Healthy People 2010 objective, 45 Medicaid programs need to expand their coverage to include all pharmacotherapies approved by the Food and Drug Administration (FDA) and behavioral therapies.
Smoking rates among Medicaid enrollees are much higher than among the general population, with 33% of enrollees reporting being current smokers in 2007 (1). This translates into 4.7 million smokers enrolled in Medicaid programs (1). Medicaid expenditures attributable to smoking total nearly $22 billion annually; representing 11% of total Medicaid expenditures (7). Tobacco-dependence treatments are highly cost-effective and even cost-saving (8). However, coverage for tobacco-dependence treatments differs widely from state to state. For example, FFS Medicaid enrollees in Oregon have coverage for all FDA-approved pharmacotherapies and three forms of tobacco-use cessation counseling, whereas FFS Medicaid enrollees in Alabama, Connecticut, Georgia, Missouri, Nebraska, and Tennessee have coverage for none.
Coverage not only varies among different Medicaid programs but also can differ among enrollees within the same Medicaid program, depending on their enrollment in either Medicaid FFS or a Medicaid MCO. In the 12 states where Medicaid MCOs were not required to cover the same benefits as Medicaid FFS, the coverage among the Medicaid populations in the state might differ. The survey did not examine differences between FFS and individual MCO programs; therefore, some states might be voluntarily providing the same FFS Medicaid coverage for tobacco-dependence treatments to certain Medicaid MCO enrollees. Differences in benefits between programs must be taken into account when assessing the overall progress toward the Healthy People 2010 objective.
The findings in this report are subject to at least three limitations. First, although all but four states provided some supporting documentation regarding covered tobacco-dependence benefits, only 62% of the documentation was complete for all covered treatments. Lack of documentation for any self-reported data increases the likelihood of reporting errors. Second, updates for certain Medicaid programs described in this report might differ from previous survey years; therefore, comparison with previous survey results could differ over time (5,6). In most cases, these differences have resulted from particular states reporting data on Medicaid MCO's voluntary coverage of tobacco-dependence treatments and not on FFS Medicaid coverage policies. Finally, these data represent coverage policies in 2007 and might not reflect current coverage policies in effect in some states.
The 2008 update to the Public Health Service's Clinical Practice Guideline urges all insurers, including Medicaid, to provide comprehensive coverage of effective treatments (both counseling and medication) (2). The Guideline also notes that without insurance coverage, clinicians likely will not assess and treat tobacco use consistently. Although 43 Medicaid programs cover some form of tobacco-dependence treatment in their FFS populations, all but two states (New Mexico and New Jersey) place restrictions on this coverage through co-payments, stepped-care requirements, enrollment in counseling to obtain medication, limitations on number of treatment courses, and not covering combined treatments. To improve cessation rates in low-income populations, Medicaid programs should remove these barriers and improve access to tobacco-dependence treatments (2,9,10).
References
- Pleis JR, Lucas JW. Summary health statistics for U.S. adults: National Health Interview Survey, 2007. Vital Health Stat 2009;10(240).
- Fiore MC, Jaen CR, Baker TB, et al. Treating tobacco use and dependence: 2008 update. Clinical practice guideline. Rockville, MD: US Department of Health and Human Services, Public Health Service; 2008. Available at http://www.surgeongeneral.gov/tobacco/index.html. Accessed October 29, 2009.
- Partnership for Prevention. A call for ACTTION (access to cessation treatment for tobacco in our nation): an action plan to address the lack of access to tobacco-use treatment. Washington, DC: Partnership for Prevention; 2008. Available at http://www.acttiontoquit.org. Accessed October 29, 2009.
- US Department of Health and Human Services. Objective 27-8b: increase insurance coverage of evidence-based treatment for nicotine dependency. In: Healthy People 2010 (conference ed, in 2 vols). Washington, DC: US Department of Health and Human Services; 2000. Available at http://www.healthypeople.gov/document/html/objectives/27-08.htm. Accessed October 29, 2009.
- CDC. State Medicaid coverage for tobacco-dependence treatments---United States, 2006. MMWR 2008;57:117--22.
- Schauffler HH, Barker DC, Orleans CT. Medicaid coverage for tobacco-dependence treatments. Health Affairs 2001;20:298--303.
- Armour BS, Finkelstein EA, Fiebelkorn IC. State-level Medicaid expenditures attributable to smoking. Prev Chronic Dis 2009;6:A84.
- Maciosek MV, Coffield AB, Edwards NM, Flottemesch TJ, Goodman MJ, Solberg LI. Priorities among effective clinical preventive services: results of a systematic review and analysis. Am J Prev Med 2006;31:52--61.
- Bonnie RJ, Stratton K, Wallace RB, eds.; Committee on Reducing Tobacco Use: Strategies, Barriers, and Consequences. Ending the tobacco problem: a blueprint for the nation. Washington, DC: National Academies Press; 2007.
- Zaza S, Briss PA, Harris KW, eds. Tobacco. In: The guide to community preventive services: what works to promote health? New York, NY: Oxford University Press; 2005. Available at http://www.thecommunityguide.org/tobacco/default.htm. Accessed October 29, 2009.
* State Medicaid programs may contract with MCOs in their state to provide services for enrollees in their Medicaid programs. The specific arrangement varies from state to state, and the services covered under that contract also vary. Additional information is available at http://www.kff.org/medicaid/20010109a-index.cfm.
† In Idaho, Medicaid enrollees can use a Preventive Health Assistance program, which provides up to $200 in benefits per enrollee per year to be used for weight-management programs or tobacco-dependence treatments. Additional information is available from the Idaho Department of Health and Welfare at http://healthandwelfare.idaho.gov/site/4161/default.aspx.
§ Coverage for nicotine replacement therapy had been dropped in 2006.
¶ A "carve out" is defined as Medical services that are separated from a contract and paid under a different arrangement (Inkelas M. Incentives in a Medicaid carve-out: impact on children with special health care needs. Health Serv Res 2005;40:79--100).
|
What is already known on this topic? Low-income populations, such as Medicaid enrollees, continue to smoke at substantially higher rates than the general population (33% versus 20%), and a Healthy People 2010 objective calls for expanding coverage for nicotine dependency treatment to all 51 Medicaid programs. What is added by this report? This 2007 survey of all 51 Medicaid programs found that although 43 (84%) programs offered coverage for some form of tobacco-dependence treatment to Medicaid enrollees, only six states covered all of the effective pharmacotherapies and individual and group counseling and only two states reported access to tobacco-dependence treatments without any limitations or restrictions. What are the implications for public health practice? Because access to comprehensive tobacco-dependence treatments has been shown to increase quit rates, providing coverage for these treatments to all Medicaid enrollees would reduce smoking in the Medicaid population. |
|
TABLE 1. (Continued) State Medicaid fee-for-service program coverage of tobacco-dependence treatments,* by type of coverage and year coverage began --- United States, 2007† |
|||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
|
SOURCE: 2007 State Medicaid Tobacco-Dependence Treatment Survey, Center for Health and Public Policy Studies, University of California, Berkeley. * Based on response to the following survey item: "Please indicate if your Medicaid program covered any of the following tobacco-dependence treatments in 2007: nicotine gum, nicotine patch, nicotine nasal spray, nicotine inhaler, nicotine lozenge, Chantix, Zyban, bupropion, individual face-to-face counseling, group counseling, proactive telephone counseling." Each state also was asked to provide documentation of coverage. † N = 45. In 2007, four states with Medicaid programs (Alabama, Connecticut, Missouri, and Tennessee) covered none of the tobacco-dependence treatments recommended in the 2000 Public Health Service Clinical Practice Guideline. Two states (Georgia and Nebraska) covered bupropion without prior authorization; therefore, it could have been used for smoking cessation, although this was not the intention of the coverage policy. § Covered specifically for smoking cessation. ¶ P = Medicaid coverage exclusively for pregnant women. ** Treatment added in 2007. †† Response differs from previous year's survey because of a previous reporting error. In most cases, this was a result of the state reporting on managed-care organization coverage policies and not Medicaid fee-for-service. §§ Covered only after the gum or patch was used in conjunction with quitline support for 2 weeks. ¶¶ In 2007, Idaho provided a $200 per enrollee per year allowance for personal health benefits that could be applied to smoking cessation benefits. *** Maine covered bupropion, but not specifically for smoking cessation. ††† Coverage for nicotine patches differs from the 2006 report because of a different interpretation of Maryland's coverage policy. Generally, Maryland does not cover any pharmaceuticals that are available over-the-counter; however, some prescription-only (legend) patches are still available and therefore were covered. §§§ Covered since 2006. This was erroneously reported as "not covered" in the previous report. ¶¶¶ Fee-for-service covers when a valid behavioral health diagnosis other than tobacco dependence exists. **** Fee-for-service Medicaid did not cover, but Medicaid managed-care organizations were required to cover. †††† Utah's coverage will continue until Tobacco Settlement funds expire. §§§§ Telephone counseling is available for free to the entire population in every state and the District of Columbia through quitlines (available by dialing 1-800-QUITNOW [784-8669]). Four states use some of their Medicaid funds to support quitline operations. ¶¶¶¶ Since 2006, two states (Kentucky and Iowa) expanded coverage beyond exclusively pregnant women to the general Medicaid population, and two states (Idaho and Wyoming) began new coverage for tobacco-dependence treatments. |
FIGURE. Number of state Medicaid programs* covering tobacco-dependence treatments --- United States, 1998--2007
SOURCE: 2007 State Medicaid Tobacco-Dependence Treatment Survey, Center for Health and Public Policy Studies, University of California, Berkeley.
* Of 51 Medicaid programs.
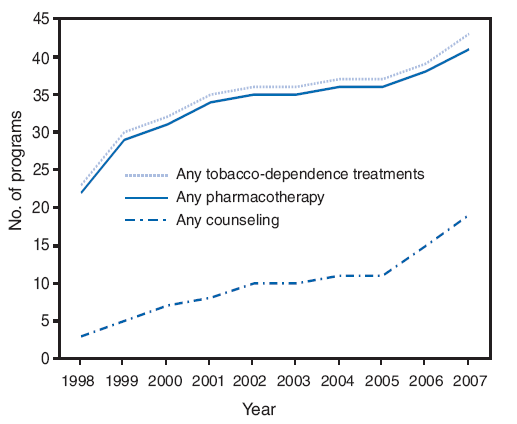
Alternative Text: The figure above shows the number of state Medicaid programs covering tobacco-dependence treatments in the United States from 1998 to 2007. Data collected over the past decade on Medicaid program coverage of tobacco-dependence treatments indicate an increase in coverage levels. In 1998, 23 Medicaid programs covered some form of tobacco-dependence treatment, with 22 programs covering pharmacotherapy and three programs covering tobacco-cessation counseling. As of 2007, an upward trend in both forms of coverage was observed, with 41 programs covering pharmacotherapy and 19 covering counseling.
Use of trade names and commercial sources is for identification only and does not imply endorsement by the U.S. Department of
Health and Human Services. |
All MMWR HTML versions of articles are electronic conversions from typeset documents. This conversion might result in character translation or format errors in the HTML version. Users are referred to the electronic PDF version (http://www.cdc.gov/mmwr) and/or the original MMWR paper copy for printable versions of official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices.
**Questions or messages regarding errors in formatting should be addressed to [email protected].Date last reviewed: 11/5/2009