
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail.
Global Measles Mortality, 2000--2008
The United Nations (UN) Millennium Development Goals include a goal (MDG 4) to achieve a two thirds overall reduction of child deaths by 2015 compared with the 1990 level (1). Because many unvaccinated children die from measles, routine measles vaccination coverage is used as an indicator of progress toward this goal. In 2008, all UN member states reaffirmed their commitment to achieving a 90% reduction in measles mortality by 2010 compared with 2000, from an estimated 733,000 deaths in 2000 worldwide to ≤73,300 by 2010 (2). The World Health Organization (WHO) and UNICEF have identified 47 priority countries with the highest burden of measles for an accelerated strategy for measles mortality reduction (3). The strategy includes 1) achieving and maintaining high coverage (≥90% nationally and ≥80% in each district) with 2 doses of measles-containing vaccine (MCV) delivered through routine services or supplemental immunization activities (SIAs) (4), 2) implementing effective laboratory-supported disease surveillance, and 3) providing appropriate clinical management for measles cases. This report updates a previously published report (5), provides details on activities implemented during 2008, assesses progress toward the 2010 goal, and evaluates the potential effects of decreased financial support. During 2000--2008, global measles mortality declined by 78%, from an estimated 733,000 deaths in 2000 to 164,000 in 2008, but the reduction in measles mortality has been leveling off since 2007. To reach the 2010 goal, India should fully implement the recommended strategies, and financial support for sustaining measles control in the other 46 priority countries should be secured.
Immunization Activities
WHO and UNICEF estimate routine first dose MCV coverage (MCV1) among children aged 1 year based on data from administrative records and surveys.* Coverage levels achieved during measles SIAs† are estimated by dividing the reported number of doses administered by the target population. According to WHO and UNICEF estimates, global routine MCV1 coverage increased to 83% in 2008, up 1% from 2007. Coverage varied substantially by geographic region (Table 1); coverage in the WHO African Region (AFR) and the South-East Asia Region (SEAR) in 2008 was still <80%. Of the 22.7 million infants and young children in 2008 who missed receiving their first dose of measles vaccine through routine immunization services,§ approximately 58% reside in six countries: India (7.63 million population), Nigeria (2.04 million), China (1.10 million), Democratic Republic of the Congo (0.84 million), Pakistan (0.75 million), and Ethiopia (0.74 million).
During 2000--2008, a second opportunity for measles immunization was provided in 46 of the 47 priority countries¶ (except India) to approximately 686 million children aged 9 months to ≤20 years through SIAs. In 2008, 16 (34%) of these countries conducted SIAs reaching approximately 109 million children and adolescents; in 13 countries, the measles SIAs were combined with at least one other child-survival intervention (Table 2).
Surveillance Activities
Effective surveillance for measles entails establishing case-based surveillance that includes investigation and laboratory testing of samples from all suspected measles cases.** In 2008, 173 (90%) of 193 WHO member states had implemented case-based surveillance, compared with 120 (63%) countries in 2004 (earlier data are not available). In 2008, the WHO measles and rubella laboratory network provided standardized and quality-controlled measles and rubella testing for 183 countries (95%), compared with 71 countries (37%) in 2000.
In 2008, 180 countries (94%) reported measles surveillance data to WHO and UNICEF through the annual Joint Reporting Form,†† compared with 169 countries (88%) in 2000. Worldwide, the number of reported measles cases declined 67%, from 852,937 in 2000 to 278,358 in 2008. All regions reported a decrease in reported measles cases; the highest percentage reductions occurred in the WHO Region of the Americas (AMR) (99.9%) and AFR (93%), and the lowest in SEAR (3.6%). However, large outbreaks occurred in several AFR countries during 2008, including the Democratic Republic of the Congo (12,461 reported cases), Ethiopia (3,511), Niger (1,317), and Nigeria (9,960).
Mortality Estimates for 2008
Despite progress in measles surveillance and reporting globally, measles incidence remains underreported, and complete and reliable surveillance data on the number of measles deaths are lacking for many countries, particularly those with the highest disease burden. To estimate measles mortality, WHO used 1) the published natural history model (6),§§ updated with the most recent population data (7), 2) WHO/UNICEF routine MCV1 coverage estimates and reported SIA coverage, and 3) measles incidence as reported to WHO.
In 2008, the majority (77%) of measles deaths occurred in SEAR (Table 1). During 2000--2008, global mortality attributed to measles declined by 78%, from an estimated 733,000 deaths in 2000 to 164,000 in 2008 (Table 1, Figure), but the decline leveled off during 2007--2008 (Figure). The regional percentage reduction in estimated measles mortality reached the 2010 target of 90% in the AFR, Eastern Mediterranean Region, and Western Pacific Region, which accounted for 60%, 17%, and 4% of the global reduction in measles mortality, respectively. In 2008, the 47 priority countries accounted for 160,000 (98%) of the estimated 164,000 measles deaths globally.
Cumulatively, an estimated 12.7 million measles deaths were averted during 2000--2008; of these, 8.4 (66%) million deaths were averted by maintaining routine immunization coverage at the 2000 level, and an additional 4.3 million (34%) deaths were averted as a result of measles SIAs and increases in routine vaccination coverage.
Global Mortality Projections, 2010--2013
Since 2008, the funding for measles control activities declined, causing concerns about the possible effect of reduced funding support on global measles mortality (8). During 2007--2009, total financial support to the Measles Initiative¶¶ decreased from $150 million annually to approximately $50 million (Measles Initiative, unpublished data, 2009). In addition, many priority countries have not been able to raise the expected 50% of operational costs for SIAs.
The natural history model (6) was used to project global measles mortality for the period 2010--2013. Two projections were considered. The first, a "worst case" projection, assumes that routine MCV1 coverage in the 47 priority countries remains at the 2008 levels during 2009--2013, and that none of these countries carry out follow-up SIAs during 2010--2013; assumptions for all other countries are that they continue to increase routine MCV1 coverage at current rates and conduct regular high-quality SIAs as required. The second, a "status quo" projection, assumes that SIAs will be conducted during 2010--2013 in 46 of the 47 priority countries (India will not implement an SIA during 2010--2013, the same as during 2000--2009), and that routine MCV1 coverage remains at the 2008 levels among countries with ≥90% coverage in 2008 and increases 1% per year among lower performing countries.
Results from these projections suggest that, under the worst case scenario, the annual number of measles deaths will rebound, resulting in approximately 1.7 million measles-related deaths during 2010--2013, including approximately 500,000 deaths in 2013 alone (Figure). Even if MCV1 coverage continues to increase at the current rate and if SIAs continue to be implemented in 46 of the 47 priority countries, as assumed in the status quo scenario, the projected global mortality during 2010--2013 will continue to level off at approximately 151,000--163,000 deaths annually if India does not implement "catch-up" SIA campaigns (Figure).
Reported by: A Dabbagh, PhD, M Gacic-Dobo, E Simons, MHS, D Featherstone, PhD, P Strebel, MBChB, JM Okwo-Bele, MD, Dept of Immunization, Vaccines, and Biologicals, World Health Organization, Geneva, Switzerland. E Hoekstra, MD, M Chopra, MBChB, United Nations Children's Fund, New York, New York. A Uzicanin, MD, S Cochi, MD, Global Immunization Div, National Center for Immunization and Respiratory Diseases, CDC.
Editorial Note:
After a period of rapid progress in reducing global measles mortality during 2000--2006, the reduction in measles mortality has begun to level off, raising the possibility that the 2010 goal might not be reached. Approximately 77% of the estimated global measles mortality in 2008 was concentrated in one region (SEAR). Further progress toward the 90% mortality reduction goal is impeded by two factors: 1) India has not fully implemented the measles mortality strategies recommended by WHO and UNICEF in 2001 (3, 4), and 2) political and financial commitment to sustaining measles control in many of the other 46 priority countries has declined.
Efforts to reduce measles-related mortality since 2000 have contributed substantially to the reduction in overall child mortality. During 2000--2008, child mortality decreased by 1.6 million, from an estimated 10.4 million to 8.8 million deaths***; during the same period, estimated measles deaths declined by 569,000, suggesting that the decline in measles-related deaths played a major role in the overall decline in child mortality. Because measles deaths play a large role in global child mortality, reductions in efforts to further decrease measles deaths (e.g., reductions in regular measles SIAs and laboratory-supported surveillance) could slow progress toward reaching MDG4.
Several related factors influence the measles mortality burden estimates and projections presented in this report. The natural history model used by WHO uses the published age-specific measles case-fatality ratios (CFRs) and keeps them constant; hence, current mortality estimates are primarily determined by changes in the size of the birth cohort and measles vaccination coverage over time (6). However, measles CFRs are known to differ within populations over time (9). Most notably, increased measles vaccination coverage is thought to be the major factor contributing to declines in overall measles CFRs. As measles vaccination coverage increases, the average age of infection rises, and a larger proportion of measles cases occur among previously vaccinated children (10). Because CFRs are one of the key parameters in estimating the global measles mortality burden, additional field studies should be conducted to gather additional CFR data, especially in post-SIA settings. Multiple factors have been associated with increased measles CFRs, including low socioeconomic status, malnutrition, vitamin A deficiency, HIV-infection, young age at infection, and lack of measles immunization. Although an age-appropriate dose of vitamin A is recommended for measles case management (3), access to vitamin A treatment often is limited.
The results achieved in 46 of the 47 priority countries suggest that a 90% reduction in global measles mortality can be achieved and sustained if the recommended strategy is implemented fully. Key factors related to a possible delay in achieving the 90% reduction in global measles mortality beyond 2010 and the risk for a measles mortality resurgence include delayed implementation of catch-up SIAs in India and suboptimal routine MCV and SIA coverage in AFR. Routine vaccination is a cornerstone of the WHO/UNICEF recommended strategy (3), and increasing MCV coverage must be given high priority to achieve and sustain the global goal.
References
- United Nations. The Millennium Development Report 2009. New York, NY: United Nations; 2009. Available at http://mdgs.un.org/unsd/mdg/resources/static/products/progress2009/mdg_report_2009_en.pdf. Accessed November 25, 2009.
- World Health Organization. Global immunization vision and strategy 2006--2015. Geneva, Switzerland: World Health Organization; 2005. Available at http://www.who.int/vaccines-documents/docspdf05/givs_final_en.pdf. Accessed November 25, 2009.
- World Health Organization, United Nations Children's Fund. Measles mortality reduction and regional elimination strategic plan 2001--2005. Geneva, Switzerland: World Health Organization; 2001. Available at http://www.who.int/vaccines-documents/docspdf01/www573.pdf. Accessed November 25, 2009.
- World Health Organization. Measles vaccines: WHO position paper. Wkly Epidemiol Rec 2009;84:349--60.
- CDC. Progress in global measles control and mortality reduction, 2000--2007 MMWR 2008;57:1303--6.
- Wolfson L, Strebel P, Gacic-Dobo M, et al. Has the 2005 measles mortality reduction goal been achieved? A natural history modelling study. Lancet 2007;369:191--200.
- United Nations. World population prospects: the 2008 revision. Available at http://www.un.org/esa/population/unpop.htm. Accessed November 25, 2009.
- World Health Organization. Meeting of the immunization Strategic Advisory Group of Experts, April 2009--conclusions and recommendations. Wkly Epidemiol Rec 2009;84:213--36.
- Wolfson LJ, Grais RF, Luquero FJ, et al., Estimates of measles case fatality ratios: a comprehensive review of community-based studies. Intl J Epidemiol 2009;38:192--205.
- Sudfield CR, Halsey NA. Measles case fatality ratio in India: a review of community based studies. Indian Pediatrics 2009;46:983--9.
* Available at http://www.who.int/immunization_monitoring/routine/immunization_coverage/en/index4.html.
† SIAs generally are carried out using two approaches. An initial, nationwide catch-up SIA targets all children aged 9 months to 14 years; it has the goal of eliminating susceptibility to measles in the general population. Periodic follow-up SIAs then target all children born since the last SIA. Follow-up SIAs are generally conducted nationwide every 2--4 years and target children aged 9--59 months; their goal is to eliminate any measles susceptibility that has developed in recent birth cohorts and to protect children who did not respond to the first measles vaccination.
§ Measles immunization coverage is the percentage of children aged 1 year who have received at least 1 MCV dose in a given year. For member states recommending the first dose of MCV in children aged >12 months, the indicator is calculated as the proportion of children aged <24 months receiving 1 MCV dose
¶ Afghanistan, Angola, Bangladesh, Benin, Burkina Faso, Burundi, Cambodia, Cameroon, Central African Republic, Chad, Congo, Côte d'Ivoire, Democratic Republic of the Congo, Djibouti, Equatorial Guinea, Eritrea, Ethiopia, Gabon, Ghana, Guinea, Guinea-Bissau, India, Indonesia, Kenya, Lao People's Democratic Republic, Liberia, Madagascar, Mali, Mozambique, Myanmar, Nepal, Niger, Nigeria, Pakistan, Papua New Guinea, Rwanda, Senegal, Sierra Leone, Somalia, Sudan, Timor-Leste, Togo, Uganda, United Republic of Tanzania, Vietnam, Yemen, and Zambia.
** Available at http://www.who.int/vaccines-documents/docspdf01/www617.pdf.
†† Includes aggregated annual case counts as reported by member states. Additional information available at http://www.who.int/immunization_monitoring/routine/joint_reporting/en/index.html.
§§ This method applies age and country-specific case fatality ratios to measles incidence estimates, which are generated by 1) reported measles case data, if reliable, adjusted for reporting efficiency, or 2) a static natural history model driven by vaccination coverage data and rates of measles transmission among unvaccinated children.
¶¶ Launched in 2001, the Measles Initiative is an international partnership committed to reducing measles deaths worldwide, and led by the American Red Cross, CDC, UNICEF, United Nations Foundation, and WHO. Additional information available at http://www.measlesinitiative.org.
*** Regional data available at http://www.childinfo.org/mortality_underfive.php.
|
What is already known on this topic? In 2008, all World Health Organization (WHO) member states reaffirmed their commitment to achieving a 90% reduction in measles mortality by 2010 compared with 2000 (with a 2010 goal of no more than 73,300 measles deaths worldwide). What is added by this report? During 2000--2008, recommended strategies were implemented in 46 or 47 countries (except India) with high measles mortality burden, resulting in a 78% decline in estimated global measles mortality, from an estimated 733,000 deaths in 2000 to 164,000 in 2008. What are the implications for public health practice? Two factors are critical for further progress toward the 90% mortality reduction goal: 1) India should fully implement the recommended measles mortality reduction strategies; and 2) financial support to sustaining measles control in the other 46 high-burden countries should be secured. |
|
TABLE 1. First-dose measles vaccination coverage through routine vaccination services among children aged 1 year* and estimated number of deaths from measles, by World Health Organization (WHO) region and among priority countries† --- Worldwide, 2000 and 2008 |
|||||||
|---|---|---|---|---|---|---|---|
|
WHO region/priority countries |
2000 |
2008 |
Proportion of estimated global decrease in measles deaths attributable to region/priority countries (%) |
||||
|
First-dose measles vaccination coverage (%) |
Estimated no. of measles deaths (uncertainty bounds)§ |
First-dose measles vaccination coverage (%) |
Estimated no. of measles deaths (uncertainty bounds)§ |
Estimated decrease in measles deaths 2000--2008 |
|||
|
No. |
(%) |
||||||
|
Africa |
56 |
371,000 (270,000--483,000) |
73 |
28,000 (19,000--40,000) |
343,000 |
(92) |
60 |
|
Americas |
92 |
<1,000¶ |
93 |
<1,000¶ |
--- |
--- |
--- |
|
Eastern Mediterranean |
72 |
101,000 (75,000--131,000) |
83 |
7,000 (5,000--10,000) |
94,000 |
(93) |
17 |
|
European |
91 |
<1,000¶ |
94 |
<1,000¶ |
--- |
--- |
--- |
|
South-East Asia |
61 |
234,000 (169,000--309,000) |
75 |
126,000 (90,000--168,000) |
108,000 |
(46) |
19 |
|
Western Pacific |
85 |
25,000 (17,000--35,000) |
93 |
2,000 (1,000--4,000) |
23,000 |
(92) |
4 |
|
Total** |
72 |
733,000 (530,000--959,000) |
83 |
164,000 (115,000--222,000) |
569,000 |
(78) |
--- |
|
Priority countries |
58 |
709,000 (517,000--925,000) |
74 |
160,000 (112,000--215,000) |
549,000 |
(81) |
96 |
|
* Coverage estimates available at http://www.who.int/immunization_monitoring/routine/immunization_coverage/en/index4.html. † Afghanistan, Angola, Bangladesh, Benin, Burkina Faso, Burundi, Cambodia, Cameroon, Central African Republic, Chad, Congo, Côte d'Ivoire, Democratic Republic of the Congo, Djibouti, Equatorial Guinea, Eritrea, Ethiopia, Gabon, Ghana, Guinea, Guinea-Bissau, India, Indonesia, Kenya, Lao People's Democratic Republic, Liberia, Madagascar, Mali, Mozambique, Myanmar, Nepal, Niger, Nigeria, Pakistan, Papua New Guinea, Rwanda, Senegal, Sierra Leone, Somalia, Sudan, Timor-Leste, Togo, Uganda, United Republic of Tanzania, Vietnam, Yemen, and Zambia. § Based on Monte Carlo simulations that account for uncertainty in key input variables (i.e., vaccination coverage and case-fatality ratios). ¶ Because the static natural history model is not sufficiently precise at low incidence levels, mortality rates below 1,000 deaths per year cannot be specified. ** Numbers and percentages in tables do not necessarily add to totals because of rounding. |
|||||||
FIGURE. Estimated number of measles deaths worldwide, 2000--2008,* and worst case/status quo projections† of possible resurgence in measles mortality, 2009--2013
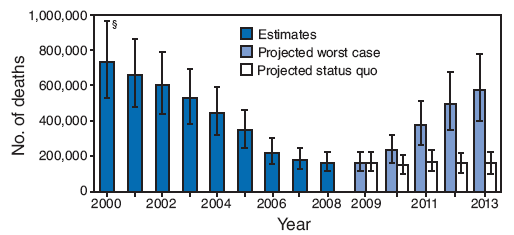
* Based on Monte Carlo stimulations that account for uncertainty in key input variables (i.e. vaccination coverage and case fatality ratios).
† Projected "worst case" scenario assumes that none of 47 priority countries carry out catch-up or follow-up supplemental immunization activities (SIAs) during 2010--2013. Under this assumption, routine first-dose measles-containing vaccine (MCV1) coverage remains at the 2008 levels during 2009--2013 in the 47 priority countries, but continues to increase at current rates in all remaining countries. Projected "status quo" scenario assumes that SIAs will continue to be conducted during 2010--2013 in 46 of the 47 priority countries (excluding India); routine MCV1 coverage remains at the 2008 levels among countries with ≥90% coverage in 2008, and increases 1% per year among lower-performing countries. The 47 priority countries include Afghanistan, Angola, Bangladesh, Benin, Burkina Faso, Burundi, Cambodia, Cameroon, Central African Republic, Chad, Congo, Côte d'Ivoire, Democratic Republic of the Congo, Djibouti, Equatorial Guinea, Eritrea, Ethiopia, Gabon, Ghana, Guinea, Guinea-Bissau, India, Indonesia, Kenya, Lao People's Democratic Republic, Liberia, Madagascar, Mali, Mozambique, Myanmar, Nepal, Niger, Nigeria, Pakistan, Papua New Guinea, Rwanda, Senegal, Sierra Leone, Somalia, Sudan, Timor-Leste, Togo, Uganda, United Republic of Tanzania, Vietnam, Yemen, and Zambia
§ 95% uncertainty intervals.
Alternative Text: The figure above shows the estimated number of measles deaths worldwide from 2000 through 2008. During that period, global mortality attributed to measles declined by 78%, from an estimated 733,000 deaths in 2000 to 164,000 in 2008, but the decline leveled off during 2007-2008. The figure also shows worst case and status quo projections for a possible resurgence in global measles mortality from 2009 through 2013.
Use of trade names and commercial sources is for identification only and does not imply endorsement by the U.S. Department of
Health and Human Services. |
All MMWR HTML versions of articles are electronic conversions from typeset documents. This conversion might result in character translation or format errors in the HTML version. Users are referred to the electronic PDF version (http://www.cdc.gov/mmwr) and/or the original MMWR paper copy for printable versions of official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices.
**Questions or messages regarding errors in formatting should be addressed to [email protected].Date last reviewed: 12/2/2009