ShareCompartir
ShareCompartir
FIGURE 1. Influenza vaccine dosing algorithm for children aged 6 months through 8 years --- Advisory Committee on Immunization Practices (ACIP), 2011--12 influenza season
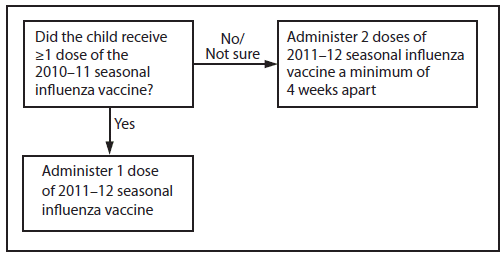
Alternate Text: The figure above shows influenza vaccine dosing algorithm for children aged 6 months through 8 years for the 2011-12 influenza season, according to the Advisory Committee on Immunization Practices (ACIP). Children aged 6 months through 8 years who did not receive at least 1 dose of the 2010-11 seasonal influenza vaccine, or for whom it is not certain whether the 2010-11 seasonal vaccine was received, should receive 2 doses of the 2011-12 seasonal influenza vaccine.