 ShareCompartir
ShareCompartir
Sources: CDC. National Health and Nutrition Examination Survey data. Available at http://www.cdc.gov/nchs/nhanes/nhanes2007-2008/nhanes07_08.htm.
US Department of Health and Human Services, US Department of Agriculture. Dietary guidelines for Americans, 2010. 7th ed. Washington, DC: US Government Printing Office; 2010.
US Department of Agriculture. What we eat in America. Washington, DC: US Department of Agriculture, Agricultural Research Service; 2010. Available at http://www.ars.usda.gov/service/docs.htm?docid=15044.
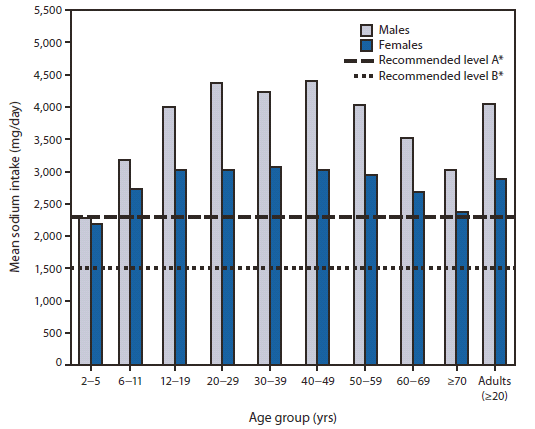
* Current dietary guidelines recommend reducing consumption of sodium to <2,300 mg/day, and that blacks, persons aged ≥51 years, and persons of any age with hypertension, diabetes, or chronic kidney disease further reduce intake to 1,500 mg/day.
Alternate Text: The figure above shows mean sodium intake (excluding table salt), by age and sex, in the United States, during 2007-2008, according to the National Health and Nutrition Examination Survey, and current recommended levels of dietary sodium. Regardless of age or sex, sodium intake by most U.S. residents considerably exceeds recommended levels.
