 |
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail. Recommendations for the Use of Lyme Disease Vaccine Recommendations of the Advisory Committee on Immunization Practices (ACIP)Please note: An erratum has been published for this article. To view the erratum, please click here. Advisory Committee on Immunization Practices Membership List, March 1999 CHAIRMAN EXECUTIVE SECRETARY MEMBERS Richard D. Clover, M.D. David W. Fleming, M.D. Mary P. Glode, M.D. Marie R. Griffin, M.D., M.P.H. Fernando A. Guerra, M.D. Charles M. Helms, M.D., Ph.D. David R. Johnson, M.D., M.P.H. Chinh T. Le, M.D. Paul A. Offit, M.D. Jessie L. Sherrod, M.D. Bonnie M. Word, M.D. EX-OFFICIO MEMBERS Robert F. Breiman, M.D. William Egan, Ph.D. Geoffrey S. Evans, M.D. T. Randolph Graydon Regina Rabinovich, M.D. Kristin Lee Nichol, M.D., M.P.H. David H. Trump, M.D., M.P.H. LIAISON REPRESENTATIVES American Academy of Family Physicians American Academy of Pediatrics American Association of Health Plans (Vacant) American College of Obstetricians and Gynecologists American College of Physicians American Hospital Association American Medical Association Association of Teachers of Preventive Medicine Biotechnology Industry Organization Canadian National Advisory Committee on Immunization Hospital Infection Control Practices Advisory Committee Infectious Diseases Society of America National Immunization Council and Child Health Program, Mexico National Medical Association National Vaccine Advisory Committee Pharmaceutical Research and Manufacturers of America (Vacant)
The following CDC staff members prepared this report: David T. Dennis, M.D., M.P.H. Martin I. Meltzer, Ph.D. National Center for Infectious Diseases
Recommendations for the Use of Lyme Disease Vaccine Recommendations of the Advisory Committee on Immunization Practices (ACIP) Summary This report provides recommendations for use of a newly developed recombinant outer-surface protein A (rOspA) Lyme disease vaccine (LYMErix,TM SmithKline Beecham Pharmaceuticals) for persons aged 15-70 years in the United States. The purpose of these recommendations is to provide health-care providers, public health authorities, and the public with guidance regarding the risk for acquiring Lyme disease and the role of vaccination as an adjunct to preventing Lyme disease. The Advisory Committee on Immunization Practices recommends that decisions regarding vaccine use be made on the basis of assessment of individual risk, taking into account both geographic risk and a person's activities and behaviors relating to tick exposure. INTRODUCTION Lyme disease is a tickborne zoonosis caused by infection with the spirochete Borrelia burgdorferi. The number of annually reported cases of Lyme disease in the United States has increased approximately 25-fold since national surveillance began in 1982; during 1993-1997, a mean of 12,451 cases annually were reported by states to CDC (1,2, CDC, unpublished data, 1998). In the United States, the disease is primarily localized to states in the northeastern, mid-Atlantic, and upper north-central regions, and to several areas in northwestern California (1). Lyme disease is a multisystem, multistage, inflammatory illness. In its early stages, Lyme disease can be treated successfully with oral antibiotics; however, untreated or inadequately treated infection can progress to late-stage complications requiring more intensive therapy. The first line of defense against Lyme disease and other tickborne illnesses is avoidance of tick-infested habitats, use of personal protective measures (e.g., repellents and protective clothing), and checking for and removing attached ticks. Early diagnosis and treatment are effective in preventing late-stage complications. Recently, two Lyme disease vaccines have been developed that use recombinant B. burgdorferi lipidated outer-surface protein A (rOspA) as immunogen -- LYMErix,TM SmithKline Beecham Pharmaceuticals, and ImuLyme,TM Pasteur Merieux Connaught. As of publication of this report, only LYMErix has been licensed by the U.S. Food and Drug Administration for use in the United States; therefore, these recommendations apply only to the use of that vaccine. Additional statements will be provided as other Lyme disease vaccines are licensed. Results of a large-scale, randomized, controlled (Phase III) trial of safety and efficacy of LYMErix in persons aged 15-70 years residing in disease-endemic areas of the northeastern and north-central United States indicate that the vaccine is safe and efficacious when administered on a three-dose schedule of 0, 1, and 12 months (3,4). Information regarding vaccine safety and efficacy beyond the transmission season immediately after the third dose is not available. Thus, the duration of protective immunity and need for booster doses beyond the third dose are unknown. CLINICAL FEATURES OF LYME DISEASE Clinical Description Most often, Lyme disease is evidenced by a characteristic rash (erythema migrans) accompanied by nonspecific symptoms (e.g., fever, malaise, fatigue, headache, myalgia, and arthralgia) (5-7). The incubation period from infection to onset of erythema migrans is typically 7-14 days but can be as short as 3 days or as long as 30 days. Some infected persons have no recognized illness (i.e., asymptomatic infection determined by serologic testing), or they manifest only nonspecific symptoms (e.g., fever, headache, fatigue, and myalgia). Lyme disease spirochetes disseminate from the site of inoculation by cutaneous, lymphatic, and bloodborne routes. The signs of early disseminated infection usually occur from days to weeks after the appearance of a solitary erythema migrans lesion. In addition to multiple or secondary erythema migrans lesions, early disseminated infection can be manifested as disease of the nervous system, the musculoskeletal system, or the heart (5-7). Early neurologic manifestations include lymphocytic meningitis; cranial neuropathy, especially facial nerve palsy; and radiculoneuritis. Musculoskeletal manifestations can include migratory joint and muscle pains with or without objective signs of joint swelling. Cardiac manifestations are rare but can include myocarditis and transient atrioventricular block of varying degree. B. burgdorferi infection in the untreated or inadequately treated patient can progress to late-disseminated disease from weeks to months after infection (5-7). The most common objective manifestation of late-disseminated Lyme disease is intermittent swelling and pain of one or some joints, usually large, weight-bearing joints (e.g., the knee). Some patients experience chronic axonal polyneuropathy, or encephalopathy, the latter usually manifested by cognitive disorders, sleep disturbance, fatigue, and personality changes. Infrequently, Lyme disease morbidity can be severe, chronic, and disabling (8,9). An ill-defined post-Lyme disease syndrome occurs in some persons after treatment for Lyme disease (10-12). Lyme disease is rarely, if ever, fatal. Diagnosis The diagnosis of Lyme disease is based primarily on clinical findings, and treating patients with early disease solely on the basis of objective signs and a known exposure is often appropriate (13). Serologic testing can, however, provide valuable supportive diagnostic information in patients with endemic exposure and objective clinical findings that indicate later-stage disseminated Lyme disease (13). When serologic testing is indicated, CDC recommends testing initially with a sensitive first test, either an enzyme-linked immunosorbent assay (ELISA) or an indirect fluorescent antibody test, followed by testing with the more specific Western immunoblot (WB) test to corroborate equivocal or positive results obtained with the first test (14). Although antibiotic treatment in early localized disease can blunt or abrogate the antibody response, patients with early disseminated or late-stage disease usually have strong serologic reactivity and demonstrate expanded WB immunoglobulin G (IgG) banding patterns to diagnostic B. burgdorferi antigens (15,16). Antibodies often persist for months or years after successfully treated or untreated infection. Thus, seroreactivity alone cannot be used as a marker of active disease. Neither positive serologic test results nor a history of previous Lyme disease ensures that a person has protective immunity. Repeated infection with B. burgdorferi has been reported (17). B. burgdorferi can be cultured from 80% or more of biopsy specimens taken from early erythema migrans lesions (18). However, the diagnostic usefulness of this procedure is limited because of the need for a special bacteriologic medium (i.e., modified Barbour-Stoenner-Kelly medium) and protracted observation of cultures. Polymerase chain reaction (PCR) has been used to amplify genomic DNA of B. burgdorferi in skin, blood, cerebrospinal fluid, and synovial fluid (19,20), but PCR has not been standardized for routine diagnosis of Lyme disease. Treatment Lyme disease can usually be treated successfully with standard antibiotic regimens (5,6). Early and uncomplicated infection, including infection with isolated cranial nerve palsy, usually responds satisfactorily to treatment with orally administered antibiotics (21). Parenteral antibiotics are generally recommended for treating meningitis, carditis, later-stage neurologic Lyme disease, and complicated Lyme disease arthritis. Late, complicated Lyme disease might respond slowly or incompletely, and more than one antibiotic treatment course can be required to eliminate active infection (8,9). Refractory Lyme disease arthritis is associated with expression of certain Class II major histocompatibility complex (MHC II) molecules (22), and can require anti-inflammatory agents and surgical synovectomy for relief of symptoms (8). In a limited number of patients, persistent or recurrent symptoms after appropriate antibiotic therapy often can be attributed to causes other than persistent infection (22,23). EPIDEMIOLOGY OF LYME DISEASE Antigenic Variation of B. burgdorferi Sensu Lato* In the United States, a number of genospecies of B. burgdorferi sensu lato have been isolated from animals and ticks, but only OspA expressing B. burgdorferi sensu stricto** has been isolated from humans (24). Existing evidence also demonstrates that rOspA vaccines will be protective against most if not all human infections in the United States (25). B. burgdorferi sensu stricto also occurs in Europe, but the dominant European and Asian genospecies are B. garinii and B. afzelii, both of which are antigenically distinct from B. burgdorferi sensu stricto (26) and vary in their expression of OspA. Vaccines using combinations of immunogenic proteins might be necessary to provide protection against multiple genospecies (27). Routes of Transmission Humans acquire B. burgdorferi infection from infected ticks at the time the tick takes a blood meal (28); Lyme disease is not spread by person-to-person contact or by direct contact with infected animals. Transplacental transmission of B. burgdorferi has been reported (29,30), but the effects of such transmission on the fetus remain unclear. The results of two epidemiologic studies document that congenital Lyme disease must be rare, if it occurs at all (31,32). Transmission in breast milk has not been described. B. burgdorferi can be cultured from the blood in some patients with early acute infection, and it is able to survive for several weeks in stored blood. However, at least one study has found that the risk for transfusion-acquired infection is minimal (33). Tick Vectors of Lyme Disease B. burgdorferi is transmitted to humans by ticks of the Ixodes ricinus complex (34). I. scapularis, the black-legged or deer tick, is the vector in the eastern United States; I. pacificus, the western black-legged tick, transmits B. burgdorferi in the western United States (35,36). I. scapularis is also a vector for human granulocytic ehrlichiosis and babesiosis (34,37). In their nymphal stage, these ticks feed predominantly in the late spring and early summer. The majority of Lyme disease cases result from bites by infected nymphs. In highly enzootic areas of the United States, approximately 15%-30% of questing I. scapularis nymphs and up to 14% of I. pacificus nymphs are infected with B. burgdorferi (38-41). However, in the southern United States, the prevalence of infection in I. scapularis ticks is generally 0%-3% (36). The risk for acquiring Lyme disease in the United States varies with the distribution, density, and prevalence of infection in vector ticks (Appendix). During the past several decades, the distribution of I. scapularis has spread slowly in the northeastern and upper north-central regions of the United States (42). Although deer are not competent reservoirs of B. burgdorferi, they are the principal maintenance hosts for adult black-legged ticks, and the presence of deer appears to be a prerequisite for the establishment of I. scapularis in any area (43). The explosive repopulation in the eastern United States by white-tailed deer during recent decades has been linked to the spread of I. scapularis ticks and of Lyme disease in this region. The future limits of this spread are not known (42). Distribution of Human Cases of Lyme Disease Lyme disease is endemic in several regions in the United States, Canada, and temperate Eurasia (1,44). The disease accounts for more than 95% of all reported cases of vectorborne illness in the United States. Using a national surveillance case definition (45), state health officials reported greater than 62,000 cases to CDC during 1993-1997, and the national mean annual rate during this 5-year period was 5.5 cases/100,000 population (1,2, CDC, unpublished data, 1998). Persons of all ages are equally susceptible to infection, although the highest reported rates of Lyme disease occur in children aged less than 15 years and in adults aged 30-59 years (1). Both underreporting and overdiagnosis are common (46-48). Approximately 90% of cases are reported by approximately 140 counties located along the northeastern and mid-Atlantic seaboard and in the upper north-central region of the United States (Appendix). A rash similar to erythema migrans of Lyme disease, but not caused by B. burgdorferi infection, has been described in patients who have been bitten by ticks in the southern United States (49,50). This rash is suspected of being associated with the bite of Amblyomma americanum ticks (51). Populations at Risk for Lyme Disease Most B. burgdorferi infections result from periresidential exposure to infected ticks (38,52-55) during property maintenance, recreation, and leisure activities. Thus, persons who live or work in residential areas surrrounded by woods or overgrown brush infested by vector ticks are at risk for acquiring Lyme disease. In addition, persons who participate in recreational activities away from home (e.g., hiking, camping, fishing, and hunting) in tick habitat and persons who engage in outdoor occupations (e.g., landscaping, brush clearing, forestry, and wildlife and parks management) in endemic areas might also be at elevated risk for acquiring Lyme disease (56-58). PREVENTION AND CONTROL OF LYME DISEASE Avoidance of Tick Habitat Whenever possible, persons should avoid entering areas that are likely to be infested with ticks, particularly in spring and summer when nymphal ticks feed. Ticks favor a moist, shaded environment, especially that provided by leaf litter and low-lying vegetation in wooded, brushy, or overgrown grassy habitat. Both deer and rodent hosts must be abundant to maintain the enzootic cycle of B. burgdorferi. Sources of information regarding the distribution of ticks in an area include state and local health departments, park personnel, and agricultural extension services. Personal Protection Persons who are exposed to tick-infested areas should wear light-colored clothing so that ticks can be spotted more easily and removed before becoming attached. Wearing long-sleeved shirts and tucking pants into socks or boot tops can help keep ticks from reaching the skin. Ticks are usually located close to the ground, so wearing high rubber boots can provide additional protection. Applying insect repellents containing DEET (n,n-diethyl-m-toluamide) to clothes and exposed skin and applying permethrin, which kills ticks on contact, to clothes, should also help reduce the risk of tick attachment. DEET can be used safely on children and adults but should be applied according to the U.S. Environmental Protection Agency guidelines to reduce the possibility of toxicity (59). Because transmission of B. burgdorferi from an infected tick is unlikely to occur before 36 hours of tick attachment (28,60), daily checks for ticks and their prompt removal will help prevent infection. Strategies for Reducing Tick Abundance The number of ticks in endemic residential areas can be reduced by removing leaf litter, brush, and woodpiles around houses and at the edges of yards and by clearing trees and brush to admit more sunlight, thus reducing deer, rodent, and tick habitat (61). Tick populations have also been effectively suppressed by applying pesticides to residential properties (62,63). Community-based interventions to reduce deer populations or to kill ticks on deer and rodents have not been extensively implemented, but might be effective in reducing communitywide risk for Lyme disease (64). The effectiveness of deer feeding stations equipped with pesticide applicators to kill ticks on deer and other baited devices to kill ticks on rodents is currently under evaluation. Prophylaxis After Tick Bite The relative cost-effectiveness of postexposure treatment of tick bites to avoid Lyme disease in endemic areas is dependent on the probability of B. burgdorferi infection after a tick bite (65). In most circumstances, treating persons for tick bite alone is not recommended (6,66). Persons who are bitten by a deer tick should remove the tick and seek medical attention if any signs and symptoms of early Lyme disease, ehrlichiosis, or babesiosis develop during the ensuing days or weeks. Early Diagnosis and Treatment Lyme disease is readily treatable in its early stages (5,6). The early diagnosis and proper antibiotic treatment of Lyme disease are important strategies for avoiding the morbidity and costs of complicated and late-stage illness. LYME DISEASE VACCINE Description LYMErix is made from lipidated rOspA of B. burgdorferi sensu stricto. The rOspA protein is expressed in Escherichia coli and purified. Each 0.5-mL dose of LYMErix contains 30 ug of purified rOspA lipidated protein adsorbed onto aluminum hydroxide adjuvant. Mechanism of Action Several studies in animals have provided evidence that B. burgdorferi in a vector tick undergoes substantial antigenic change between the time of tick attachment on a mammalian host and subsequent transmission of the bacterium to the host. The spirochetes residing in the tick gut at the initiation of tick feeding express primarily OspA. As tick feeding begins, the expression of outer-surface protein C (OspC) is increased and the expression of OspA is decreased, so that spirochetes that reach the mammalian host after passing through the tick salivary glands express primarily OspC (67). Thus, the rOspA vaccine might exert its principal protective effect by eliciting antibodies that kill Lyme disease spirochetes within the tick gut (68,69). Route of Administration, Vaccination Schedule, and Dosage LYMErix is administered by intramuscular injection, 0.5 mL (30 ug), into the deltoid muscle. Three doses are required for optimal protection. The first dose is followed by a second dose 1 month later and a third dose administered 12 months after the first dose. Vaccine administration should be timed so that the second dose of the vaccine (year 1) and the third dose (year 2) are administered several weeks before the beginning of the B. burgdorferi transmission season, which usually begins in April. The safety and immunogenicity of alternate dosing schedules are currently being evaluated. VACCINE PERFORMANCE Safety Randomized, Controlled Clinical (Phase III) Trial of LYMErix A total of 10,936 subjects aged 15-70 years living in Lyme disease-endemic areas were recruited at 31 sites and randomized to receive three doses of vaccine or placebo (3); 5,469 subjects received at least one 30-ug dose of rOspA vaccine, and 5,467 subjects received at least one injection of placebo. The subjects were then followed for 20 months. Information regarding adverse events that were believed to be related or possibly related to injection were available from 4,999 subjects in each group. Soreness at the injection site was the most frequently reported adverse event, which was reported without solicitation by 24.1% of vaccine recipients and 7.6% of placebo recipients (p less than 0.001). Redness and swelling at the injection site were reported by less than 2% of either group but were reported more frequently among vaccine recipients than among those who received placebo (p less than 0.001). Myalgia, influenza-like illness, fever, and chills were more common among vaccine recipients than placebo recipients (p less than 0.001), but none of these was reported by more than 3.2% of subjects (3). Reports of arthritis were not significantly different between vaccine and placebo recipients, but vaccine recipients were significantly (p less than 0.05) more likely to report arthralgia or myalgia within 30 days after each dose (70). No statistically significant differences existed between vaccine and placebo groups in the incidence of adverse events more than 30 days after receiving a dose, and no episodes of immediate hypersensitivity among vaccine recipients were noted (3). Safety in Patients with Previously Diagnosed Lyme Disease The safety of three different dosage strengths of rOspA vaccine with adjuvant in 30 adults with previous Lyme disease was evaluated in an uncontrolled safety and immunogenicity trial (71). Doses were administered at 0, 1, and 2 months. Follow-up of subjects was conducted 1 month after the third dose. No serious adverse events were recorded during the study period. In the randomized controlled Phase III trial of LYMErix, the incidence of adverse events among vaccinees who were seropositive at baseline was similar to the incidence among those who were seronegative (70). The incidence of musculoskeletal symptoms within the first 30 days after vaccination was higher among vaccinees with a self-reported previous history of Lyme disease compared with vaccinees with no such history. This difference was not statistically significant at the p = 0.05 level in the placebo group. No statistically significant difference existed in the incidence of late musculoskeletal adverse events between vaccine and placebo recipients with a self-reported previous history of Lyme disease (70). Risk for Possible Immunopathogenicity of rOspA Vaccine After infection with B. burgdorferi, persons who express certain MHC II molecules are more likely than others to develop chronic, poorly responsive Lyme arthritis associated with high levels of antibody to OspA in serum and synovial fluid (22). In chronic Lyme arthritis patients, the levels of antibody to OspA, and especially to the C-terminal epitope of OspA, have been found to correlate directly with the severity and duration of the arthritis (72). Researchers have proposed that an autoimmune reaction might develop within the joints of some Lyme arthritis patients as a result of molecular mimicry between the dominant T-cell epitope of OspA and human leukocyte function associated antigen 1 (hLFA-1) (73). The Phase III trial did not detect differences in the incidence of neurologic or rheumatologic disorders between vaccine recipients and their placebo controls during the 20 months after the initial dose (3). However, because the association between immune reactivity to OspA and treatment-resistant Lyme arthritis is poorly understood, the vaccine should not be administered to persons with a history of treatment-resistant Lyme arthritis. Efficacy Randomized, Controlled Trial (Phase III) of LYMErix Using an intention-to-treat analysis, the vaccine efficacy in protecting against "definite" Lyme disease after two doses was 49% (95% confidence interval [CI] = 15%-69%) and after three doses was 76% (95% CI = 58%-86%) (3). (In this study, "definite" Lyme disease was defined as the presence of erythema migrans or objective neurologic, musculoskeletal, or cardiovascular manifestations of Lyme disease, plus laboratory confirmation of infection by cultural isolation, PCR positivity, or WB seroconversion.) Efficacy in protecting against asymptomatic infection (no recognized symptoms, but with WB seroconversions recorded in year 1 or year 2) was 83% (95% CI = 32%-97%) in year 1 and 100% (95% CI = 26%-100%) in year 2. Immunogenicity A subset of adult subjects enrolled in the Phase III clinical trial of LYMErix was studied for the development of OspA antibodies at months 2, 12, 13, and 20 (3). At month 2, one month after the second injection, the geometric mean antibody titer (GMT) of IgG anti-OspA antibodies was 1,227 ELISA units/mL. Ten months later, the GMT had declined to 116 ELISA units/mL. At month 13, one month after the third injection, a marked anamnestic response resulted in a GMT of 6,006 ELISA units/mL. At month 20, the mean response had decreased to 1,991 ELISA units/mL (70). An analysis of antibody titers and the risk for developing Lyme disease for a subset of subjects enrolled in the Phase III clinical trial concluded that a titer greater than 1,200 ELISA units/mL correlated with protection (SmithKline Beecham poster at Infectious Disease Society of America Conference, Denver, Colorado, November 1998). Effect of Vaccination on the Serologic Diagnosis of Lyme Disease Care providers and laboratorians should be advised that vaccine-induced anti-rOspA antibodies routinely cause false-positive ELISA results for Lyme disease (74). Experienced laboratory workers, through careful interpretation of the results of WB, can usually discriminate between B. burgdorferi infection and previous rOspA immunization, because anti-OspA antibodies do not develop after natural infection. COST-EFFECTIVENESS OF LYME DISEASE VACCINATION The cost of Lyme disease has been evaluated from both a societal and a third-party-payer perspective (75). The cost-effectiveness of vaccinating against Lyme disease has also been analyzed from a societal perspective (76). At an assumed cost of vaccination of $100/person/year, a vaccine effectiveness of 0.85, a probability of 0.85 of correctly identifying and treating early Lyme disease, and an assumed incidence of Lyme disease of 1,000/100,000 persons/year, the net cost of vaccination to society was $5,692/case averted and $35,375/complicated neurologic or arthritic case avoided (Figure 1). Using these same baseline assumptions, the societal cost of vaccination exceeds the cost of not vaccinating, unless the incidence of Lyme disease is greater than 1,973/100,000 persons/year. Of the variables examined, the incidence of Lyme disease had the greatest impact on cost-effectiveness of vaccination. The likelihood of early diagnosis and treatment also has a substantial impact on vaccine cost-effectiveness because of the reduced incidence of sequelae when Lyme disease is diagnosed and patients are treated early in the disease. Most disease-endemic states and counties report Lyme disease incidence that are substantially below 1,000/100,000 persons/year. For example, in 1997, the highest reported state incidence was 70/100,000 persons in Connecticut, and the highest reported county incidence was 600/100,000 population in Nantucket County, Massachusetts. However, some studies document that approximately 10%-15% of physician-diagnosed cases of Lyme disease are reported to state authorities in highly endemic areas (46,47). Epidemiologic studies of populations at high risk in the northeastern United States have estimated annual incidence of greater than 1,000/100,000 persons/ year in several communities (77-80). ASSESSING THE RISK FOR LYME DISEASE The decision to administer Lyme disease vaccine should be made on the basis of an assessment of individual risk, which depends on a person's likelihood of being bitten by tick vectors infected with B. burgdorferi. This likelihood is primarily determined by the following:
Assessing risk should include considering the geographic distribution of Lyme disease. The areas of highest Lyme disease risk in the United States are concentrated within some northeastern and north-central states. The risk for Lyme disease differs not only between regions and states and counties within states (Appendix), but even within counties and townships. Detailed information regarding the distribution of Lyme disease risk within specific areas is best obtained from state and local public health authorities. The second step in determining Lyme disease risk is to assess a person's activities. Activities that place persons at high risk are those that involve frequent or prolonged exposure to the habitat of infected ticks at times of the year when the nymphal stages of these ticks are actively seeking hosts, which in most endemic areas is April-July. Typical habitat of Ixodes ticks are wooded, brushy, or overgrown grassy areas that are favorable for deer and the ticks' rodent hosts. Several recreational, property maintenance, occupational, or leisure pursuits that are carried out in tick habitat can be risky activities. When in highly endemic areas, persons can reduce their risk for Lyme disease and other tickborne illnesses by avoiding tick-infested habitats. If exposure to a tick-infested habitat cannot be avoided, persons should use repellents, wear protective clothing, and regularly check themselves for ticks. Persons who are unlikely to seek medical care for early manifestations of Lyme disease can be at increased risk for Lyme disease complications. Morbidity from Lyme disease can be substantially reduced by detecting and treating the infection in its early stages, because early and correct treatment usually results in a prompt and uncomplicated cure. RECOMMENDATIONS FOR USE OF LYME DISEASE VACCINE Lyme disease vaccine does not protect all recipients against infection with B. burgdorferi and offers no protection against other tickborne diseases. Vaccinated persons should continue to practice personal protective measures against ticks and should seek early diagnosis and treatment of suspected tickborne infections. Because Lyme disease is not transmitted person-to-person, use of the vaccine will not reduce risk among unvaccinated persons. Decisions regarding the use of vaccine should be based on individual assessment of the risk for exposure to infected ticks and on careful consideration of the relative risks and benefits of vaccination compared with other protective measures, including early diagnosis and treatment of Lyme disease. The risk for Lyme disease is focally distributed in the United States (Appendix). Detailed information regarding the distribution of Lyme disease risk within specific areas is best obtained from state and local public health authorities. The following recommendations are made regarding use of Lyme disease vaccine:
Travelers can obtain some protection from two doses of vaccine but will not achieve optimal protection until the full series of three doses has been administered. All travelers to high- or moderate-risk areas during Lyme disease transmission season should practice personal protection measures as described earlier and seek prompt diagnosis and treatment if signs or symptoms of Lyme disease develop. Lyme disease is endemic in some temperate areas of Europe and Asia; however, considerable heterogeneity of expression exists in the Eurasian strains of B. burgdorferi sensu lato that infect humans, and whether the rOspA vaccine licensed for use in the United States would protect against infection with Eurasian strains is uncertain.
No evidence exists that pregnancy increases the risk for Lyme disease or its severity. Acute Lyme disease during pregnancy responds well to antibiotic therapy, and adverse fetal outcomes have not been reported in pregnant women receiving standard courses of treatment. A vaccine pregnancy registry has been established by SmithKline Beecham Pharmaceuticals. In the event that a pregnant women is vaccinated, health-care providers are encouraged to register this vaccination by calling, toll-free, (800) 366-8900, ext. 5231.
FUTURE CONSIDERATIONS Recommendations for Surveillance, Research, Education, and Program Evaluation Activities
References
* sensu lato: including all subordinate taxa of a taxon that would otherwise be considered separately. ** sensu stricto: excluding similar taxa that otherwise would be considered together. Figure 1 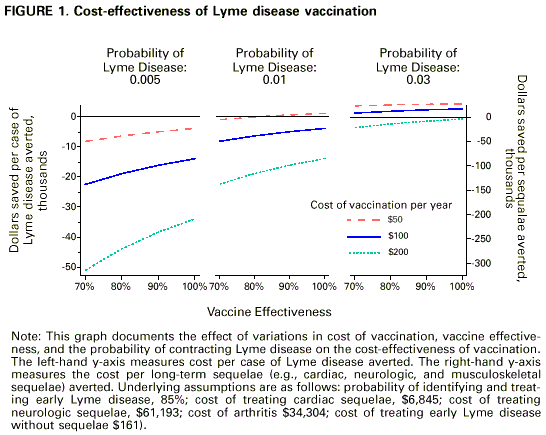 Return to top. Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to [email protected].Page converted: 6/3/99 |
|||||||||
This page last reviewed 5/2/01
|