 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail. Appendix Methods Used for Creating a National Lyme Disease Risk Map*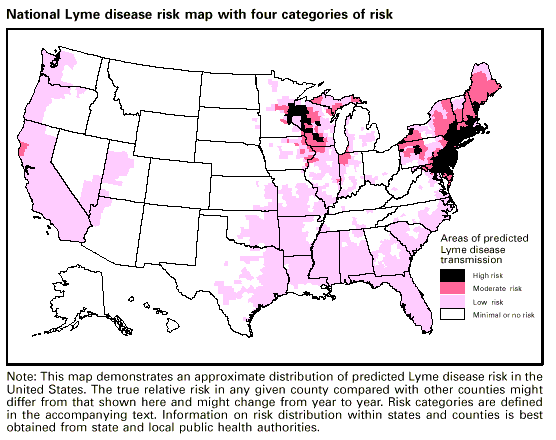 INTRODUCTION Lyme disease risk is measurable as a function of two epidemiologic parameters entomologic risk and human exposure. Entomologic risk for Lyme disease is defined as the density per unit area of host-seeking nymphal ticks infected with Borrelia burgdorferi (1). Field studies needed for determination of entomologic risk require trained entomologists, and such studies are limited to a narrow seasonal window within the life-cycle of vector ticks. Limited resources preclude the direct measurement of entomologic risk over large geographic areas; therefore, indirect measures were used to estimate risk to develop this national Lyme disease risk map. First, data on vector distribution, abundance, B. burgdorferi infection prevalence, and human exposure were compiled on a county-unit scale for the United States. Then geographic information systems (GIS) technology was used to combine these data and categorize each of the 3,140 counties into four risk classes. ENTOMOLOGIC RISK Vector Distribution Vector data were obtained from a national distribution map of Ixodes scapularis and I. pacificus, which was previously published by CDC (2). These data delineate three classes of tick distribution based on all published and unpublished county collection records available to CDC before 1998. The three classes are as follows:
Although these data are currently the best source of vector distribution available, many gaps exist because of uneven sampling efforts among the counties. Therefore, a neighborhood analysis GIS procedure was used to modify the original tick distribution to smooth absent data and minimize the impact of reporting gaps. In this process, the original tick coverage map was rasterized to 1 km, and each cell was given a numeric value corresponding to the county tick class (0 = absent; 1 = reported; and 2 = established). A neighborhood analysis was performed using ERDAS IMAGINE** image-processing software. This function employed a moving filter (25 by 25 km), which summed the values of the area surrounding each 1-km pixel and created a new focally smoothed image. An outline of counties was overlaid to define boundaries on the smoothed map, and new values were summed from the total pixel values for each county. The three original vector classes were maintained with the new classification. The revised map employed a threshold reclassification based on mean summary statistics generated from the neighborhood analysis. This procedure resulted in a weighted value for each county that was determined by the classes of surrounding counties, thus smoothing the map to minimize rough edges and isolated holes in the data. The modified vector distribution increased the number of counties containing I. scapularis and I. pacificus from 1,058 counties (34% of total counties) in the original data set to 1,404 (45% of total) in the modified version. This modification resulted in greater continuity among adjacent counties, as well as a less-conservative description of vector distribution. Infection Prevalence in Vectors The prevalence of infection with B. burgdorferi is low throughout the distribution of I. pacificus (3) with the exception of one California county (4). Within the entire southern distribution of I. scapularis, prevalence of infection with B. burgdorferi is low compared with the Northeast and upper Midwest (3). One possible reason for these differences is the geographic variations in abundance of hosts that are competent reservoirs of infection for immature ticks. The white-footed mouse (Peromyscus leucopus) is the principal host for ticks in the Northeast and upper Midwest and is a competent reservoir for the spirochete. But in the Southeast and West Coast regions, reptiles appear to serve as major hosts for immature ticks, and reptiles are either inefficient or incompetent reservoir hosts for spirochetes. This pattern of tick-host association might result from the greater population density of lizards relative to rodents (5<|>), resulting in reduced transmission rates in regions where lizards dominate. An index was created to map the effect of host-species composition on infection prevalence in I. scapularis ticks. A literature survey was conducted to identify a complete list of hosts for I. scapularis (6). A total of 38 nondomestic host species was identified, including 32 mammal species and 6 reptile species. Birds were excluded because of their migratory nature and their uncertain role as natural reservoir hosts. Species range maps were obtained from the literature (7,8), then digitized by county into ArcView GIS*** software for presence or absence of reservoir hosts. The county data were then summed to determine the total host species composition available for I. scapularis. A ratio of total reptiles divided by the total hosts multiplied by 100 was calculated for each county and mapped. The reptile ratio index delineates those areas having a high reptile-to-total-hosts ratio (>10) and forms a linear boundary, below which reptiles are more likely to serve as hosts for ticks. The geographic boundary runs roughly on the 38Ý north latitude from Virginia to Missouri. This reptile ratio illustrates that although total hosts in the northern states can be equal to those of the southern states, reptiles dilute the force of transmission, thus lowering the prevalence of infection in ticks and creating less of a risk to humans in the South. HUMAN EXPOSURE TO RISK CDC case reports were used as a measure of human exposure to entomologic risk. County-specific data were compiled for the years 1994 1997. Counties comprising the ninetieth percentile of all human cases reported during this 4-year period were selected to represent counties with high human exposure. These 137 counties reported a minimum total of 23 cases. Heuristic, or procedure-based decision rule, was employed to construct the national Lyme disease risk map. Expert decision rule was applied to construct the risk classification as follows: Risk Classes
The national map illustrates a clear focal pattern of Lyme disease risk with the greatest risk occurring in the Northeast and upper Midwest regions. Overall, 115 (4%) counties were classified as high risk, followed by 146 (5%) moderate risk, 1,143 (36%) low risk, and 1,736 (55%) as minimal or no-risk counties. ReferencesAppendix References
* Source: Durland Fish, Ph.D. and Carrie A. Howard, M.A. Department of Epidemiology and Public Health, Yale University School of Medicine, New Haven, Connecticut. ** ERDAS IMAGINE map production computer software, a product of ERDAS, Inc., 2801 Buford Highway, Atlanta, GA 30329-2137, (404) 248-9000, <http://www.erdas.com>. *** ARCView GIS computer software, a product of Environmental Systems Research Institute, Inc., 380 New York Street, Redlands, CA 92373-8100, <http://www.esri.com>. Summary Table To print large tables and graphs users may have to change their printer settings to landscape and use a small font size.
Summary Table
Recommendations for Use of Recombinant Outer-Surface Protein A Vaccine
for the Prevention of Lyme Disease
Advisory Committee on Immunization Practices, 1999
Vaccination
Recommendation
---------------------------------------------------------------------------------------------
Persons who reside, work, or recreate in areas of high or moderate
risk
Persons aged 15-70 years whose exposure to tick-infested habitat
is frequent or prolonged Should be considered
Persons aged 15-70 years who are exposed to tick-infested habitat,
but whose exposure is not frequent or prolonged May be considered
Persons whose exposure to tick-infested habitat
is minimal or none Not recommended
Persons who reside, work, or recreate in areas of low or no risk Not recommended
Travelers to areas of high or moderate risk
Travelers aged 15-70 years whose exposure to tick-infested habitat
is frequent or prolonged Should be considered
Children aged <15 years Not recommended
Pregnant women
Health-care providers are encouraged to register vaccinations
of pregnant women by calling SmithKline Beecham, toll free,
at (800) 366-8900, ext. 5231 Not recommended
Persons with immunodeficiency No available data
Persons with musculoskeletal disease Limited data
available
Persons with previous history of Lyme disease
Persons aged 15-70 years with previous uncomplicated
Lyme disease who are at continued high risk Should be considered
Persons with treatment-resistant Lyme arthritis Not recommended
Persons with chronic joint or neurologic illness related to
Lyme disease and persons with second- or third-degree
atrioventricular block No available data
Other Recommendations
Vaccine schedule
Three doses administered by intramuscular injection as follows:
Initial dose, followed by a second dose 1 month later,
followed by a third dose 12 months after the first dose
Second dose (year 1) and third dose (year 2) administered
several weeks before the beginning of the disease-transmission
season, which is usually April
Boosters
Existing data indicate that boosters might be needed, but
additonal data are required before recommendations can be
made regarding booster schedules
Simultaneous administration with other vaccines
Additional data needed
If simultaneous administration is necessary, use separate
syringes and separate injection sites
---------------------------------------------------------------------------------------------
All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to [email protected].Page converted: 6/3/99 |
|||||||||
This page last reviewed 5/2/01
|