Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail.
Acute Idiopathic Pulmonary Hemorrhage Among Infants
Recommendations from the Working Group for Investigation and Surveillance
Prepared by
Clive M. Brown, M.B.B.S.
Stephen C. Redd, M.D.
Scott A. Damon, M.A.I.A. Division of Environmental Hazards and Health Effects
National Center for Environmental Health
The material in this report originated in the National Center for Environmental Health, Richard J. Jackson, M.D., Director; and the Division of Environmental Hazards and Health Effects, Michael A. McGeehin, Ph.D., Director.
Summary
This report presents CDC's recommended case definitions and surveillance practices for Acute Idiopathic
Pulmonary Hemorrhage (AIPH). In 1994 and 1997, CDC reported clusters of acute pulmonary hemorrhage (APH) among infants in Cleveland, Ohio. Subsequent reviews of these investigations identified shortcomings in the conduct of the studies and concluded that the investigations did not prove an association between APH among infants and exposure to molds. In response to recommendations from these reviews, with assistance of external consultants, CDC staff developed a plan to conduct surveillance for and investigation of AIPH. In developing this response, CDC recommends a definition for a clinically confirmed case of AIPH among infants on the basis of evidence of blood in the airway, age
<1 year, absence of medical conditions related to pulmonary hemorrhage, and severe acute respiratory distress or respiratory failure. CDC recommends that pediatric intensive care units (PICUs) report cases that meet the CDC case definition to state health departments. CDC
staff will study the number of reported cases of AIPH among infants and also review the Cleveland and Chicago case series
to determine the degree to which the present case definition applies to them. If these reviews establish that AIPH among infants is a public health problem, on the basis of its magnitude or geographic or temporal distribution, targeted case surveillance will be initiated based on the distribution of cases. CDC staff will work with state and local health departments to
investigate reported clusters of cases of AIPH among infants.
Background
This report presents CDC's recommendations for case definitions for Acute Idiopathic Pulmonary Hemorrhage
(AIPH) among infants and CDC's plan for retrospective surveillance for AIPH among infants, including a study to evaluate
the feasibility of using International Classification of
Diseases (ICD) (1) codes for surveillance for AIPH.
In 1994 and 1997, CDC reported clusters of acute pulmonary hemorrhage (APH) among infants (2,3) in Cleveland, Ohio. During 1992--1994, a similar cluster occurred in the Chicago area (4). In Cleveland, risk factors for illness included male
sex; lack of breast-feeding; residence in households with smokers; residence in homes where water damage had occurred during the previous 6 months; and residence in homes with increased quantities of fungi, including
Stachybotrys atra.
Reviews by CDC staff and external consultants of these
investigations identified shortcomings in the conduct of the
studies (5). These panels concluded that the investigations did not prove an association between APH among infants and exposure to molds, specifically S. chartarum
(atra). These reviewers recommended that CDC, pediatric pulmonologists, and state and
local public health officials collaborate to
develop a standard surveillance case definition;
develop standard protocols for data collection and environmental assessment;
implement surveillance for AIPH;
investigate cases of AIPH among infants, particularly when clusters are identified, considering associations with
multiple possible etiologies; and
enhance sampling and laboratory analytic methods to improve assessment of environmental exposures to molds and
fungi (5).
In response to the reviewers' recommendations, CDC staff developed a plan to conduct surveillance for AIPH,
investigate clusters of cases, and conduct studies. In formulating this response, CDC convened three meetings to establish a
case definition and classification scheme for public health surveillance for AIPH, recommend a standard home
environmental investigation protocol, and outline a plan for surveillance and investigation of AIPH among infants. As a consequence of these meetings, CDC has determined that a series of surveillance activities should be initiated to direct future efforts. In addition to providing an overview of the results of the three meetings, this report
describes surveillance activities and how results
from those activities can guide efforts to investigate the burden and etiology of AIPH among infants.
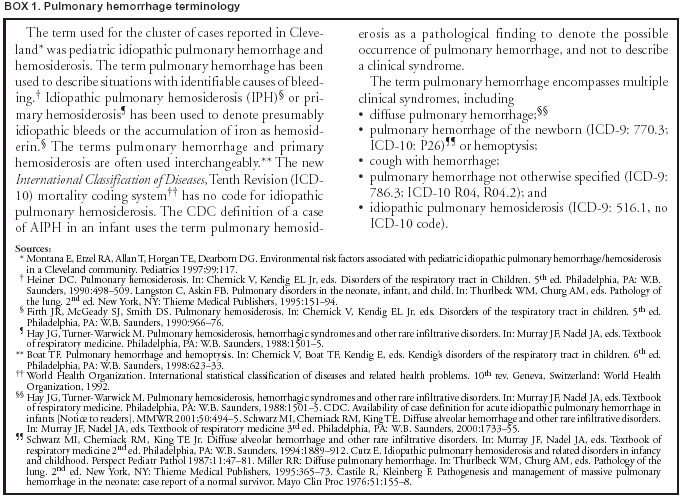
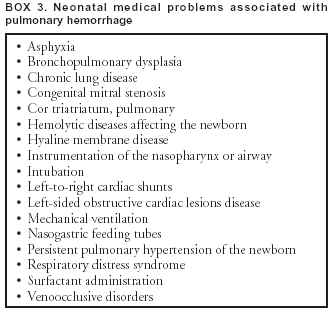
AIPH among infants is a diagnosis of exclusion. Certain syndromes (Box 1) and other disease states can occur
with pulmonary hemorrhage. Thus, differential diagnoses and neonatal medical problems that can cause pulmonary hemorrhage should be ruled out.
Meeting Panelists and Goals
Three meetings of panelists were convened to advise
CDC staff regarding investigation of AIPH among
infants. The Case Definition Panel included three pediatric pulmonologists, one pediatric intensive care specialist, one pediatric pathologist, two epidemiologists, and one environmental epidemiologist. The purpose of this panel was to recommend a case definition for
use in public health surveillance for AIPH to facilitate case finding. Case finding will facilitate documentation of the burden of
the condition and identification of possible etiologic agents or risk factors.
The Surveillance Implementation Panel included one
pediatrician, one pediatric pulmonologist, one forensic
pathologist, three epidemiologists (including one state epidemiologist), and four environmental epidemiologists (including one state epidemiologist and one toxicologist). Its purpose was to recommend a standard approach for public health surveillance for AIPH.
The Home/Indoor Environment and Laboratory Investigation Panel included two mycologists, one biochemist,
two microbiologists, two industrial hygienists, two toxicologists, and one environmental epidemiologist. Its purpose was
to recommend standard approaches and protocols for environmental data collection, laboratory analysis, and data
interpretation during public health surveillance for AIPH.
For each of the three areas, group discussion led by a moderator was based on prepared questions. Participants
produced written summaries, which form the basis of the recommendations provided in this report.
Case Definition
Case Classification and Severity Criteria
AIPH is the sudden onset of pulmonary hemorrhage in a previously healthy infant in whom differential diagnoses
and neonatal medical problems that might cause pulmonary hemorrhage have been ruled out. Pulmonary hemorrhage
can appear as hemoptysis or blood in the nose or airway with no evidence of upper respiratory or gastrointestinal bleeding. Patients have acute, severe respiratory distress or failure,
requiring mechanical ventilation and chest radiograph (CXR),
and usually demonstrate bilateral infiltrates.
AIPH among infants and sudden infant death syndrome (SIDS) potentially share similar risk factors (e.g., age group and maternal cigarette smoking). Also, in certain cases, SIDS is associated with pulmonary hemorrhage found at autopsy
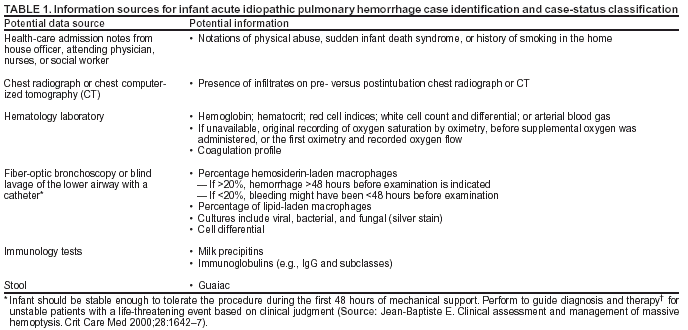
(6,7). Thus, factors that are known risk factors for SIDS should be identified when evaluating an infant possibly having AIPH. Potential information sources for case-identification and case-status classification during an investigation of
pulmonary hemorrhage are provided (Table 1).
Clinically Confirmed Cases of AIPH Among Infants
Criteria for a confirmed case include pulmonary hemorrhage in a previously healthy infant aged <1 year with a gestational age of
>32 weeks, with no history of neonatal medical problems that might cause pulmonary hemorrhage, and whose condition meets all of the following three criteria:
Abrupt or sudden onset of overt bleeding or obvious evidence of blood in the airway, including
--- epistaxis, hemoptysis, or frank blood in the airway below the larynx at visualization, not caused by any medical procedure (e.g., laryngoscopy or intubation); or
--- identification of hemosiderin-laden macrophages (>20% of pulmonary macrophages containing hemosiderin
on bronchoalveolar lavage or biopsy specimen). A source of bleeding from the nose and oropharynx should be ruled out
at the time of admission.
Severe-appearing illness leading to acute respiratory distress or respiratory failure, resulting in hospitalization in a
pediatric intensive care unit (PICU) or neonatal intensive care unit (NICU) with intubation and mechanical ventilation.
Diffuse unilateral or bilateral pulmonary infiltrates visible on CXR or computerized tomography (CT) of the chest. CXR
or chest CT findings should be documented within 48 hours of examination of the infant.
A previously healthy infant should
have been discharged from the hospital after birth with an uneventful course before the occurrence of bronchoalveolar hemorrhage;
never have been previously intubated, nor required respiratory support with oxygen;
not have evidence of physical abuse;
not have any abnormality identified on admission or
follow-up bronchoscopy that would explain the bleeding; and
not have neonatal medical problems that can cause pulmonary hemorrhage.
CDC will adhere closely to this case definition, requiring that all the criteria be met for a confirmed case. The definition
for a clinically confirmed case excludes pulmonary hemorrhage among older children and infants with restricted access to a
PICU. Because no criteria exist for postmortem examinations, this definition excludes infants who die before hospital and
PICU admission, whose illness might have met the case definition. However, the definitions for probable and suspect cases (see the following) will capture the majority of these cases and allow identification of illness among infants who die before examination by a physician.
Probable Cases of AIPH Among Infants
Criteria for a probable case include a previously healthy
infant aged <1 year with a gestational age of
>32 weeks,
who has a sudden onset of bleeding from the airway, with or without respiratory distress, with or without intubation,
and with or without pulmonary infiltrates on CXR or chest CT;
or
who died and had evidence of bleeding from the airway found on autopsy or postmortem; had been in respiratory
distress; would or should have been intubated in the opinion of a clinician; and would have had infiltrates on CXR or chest CT.
Suspected Cases of AIPH Among Infants
Criteria for a suspected case include a previously healthy infant,
who died and had evidence of bleeding from the airway found on autopsy or postmortem or who
either did not have chest imaging studies or had imaging studies that indicated no pulmonary infiltrates.
Respiratory distress or intubation is not required for a suspected case.
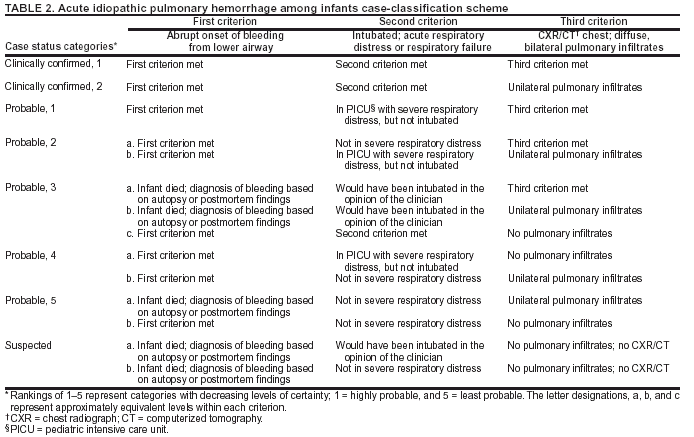
Severity Classification Scheme for AIPH Among Infants
Because of the potential for variation in symptoms among infants for each of the criteria, different case combinations might be related to the timing or duration of symptoms, disease severity, pathologic processes, or etiologic agents associated
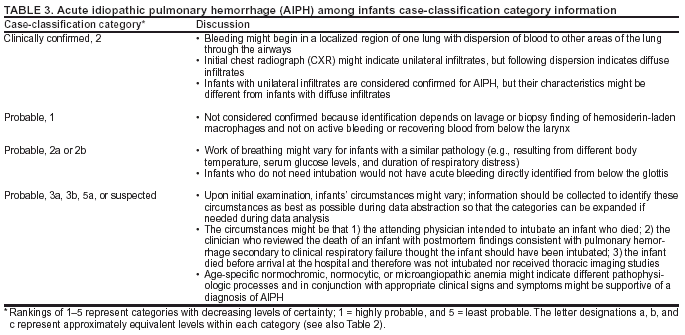
with AIPH among infants. A discussion of the proposed case-classification categories for AIPH among infants is provided (Tables
2 and 3).
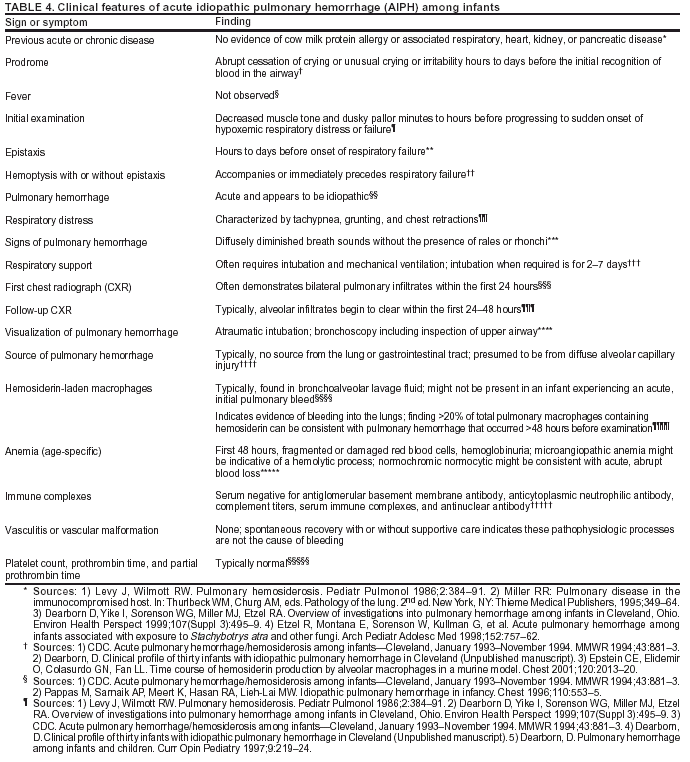
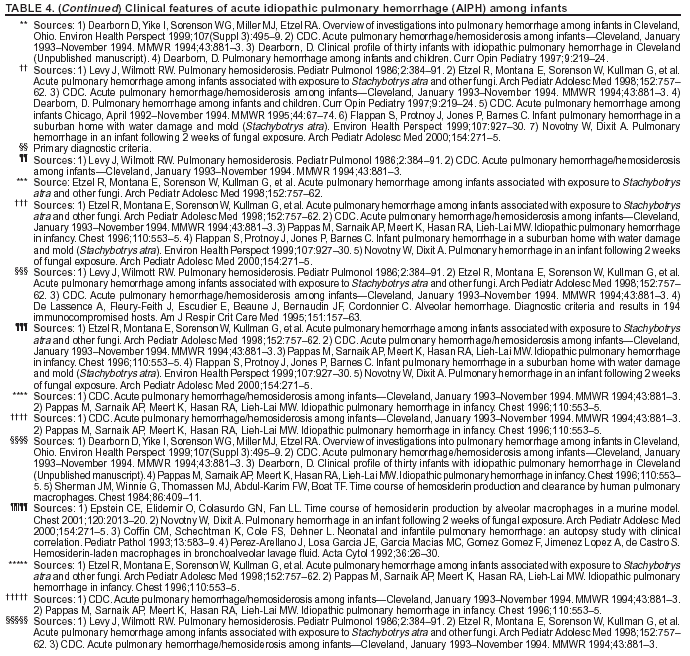
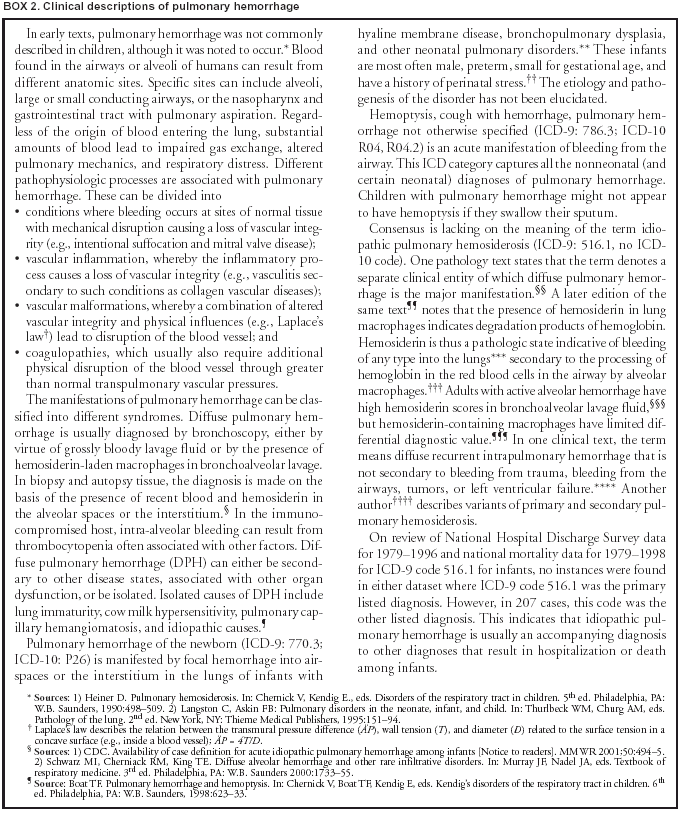
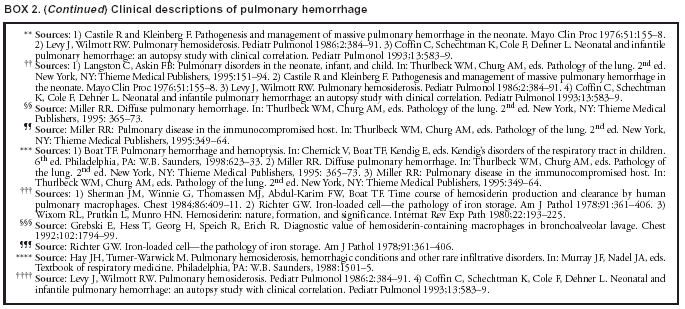
A summary of clinical features of AIPH among infants
(Table 4) (Box 2) and neonatal medical problems and
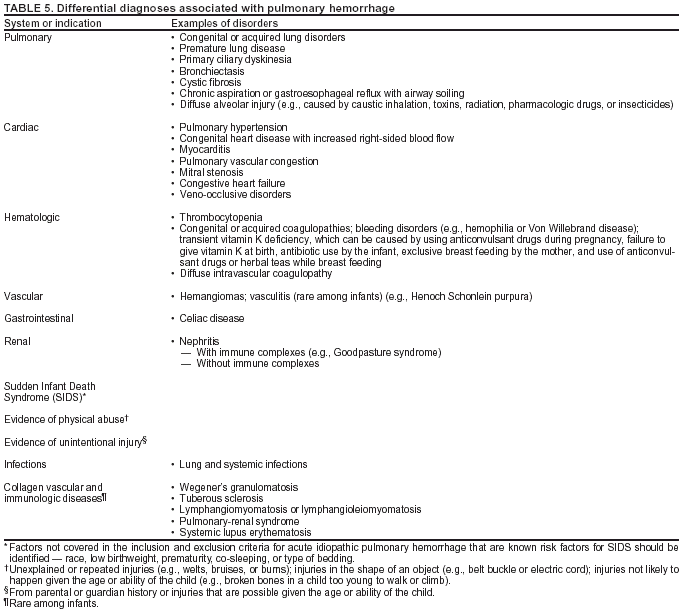
differential diagnoses that should be ruled out before classifying a case as AIPH among infants (Box 3) are included. Other differential diagnoses associated with pulmonary hemorrhage are listed (Table 5).
Feasibility Study To Determine the Concordance of ICD Codes
for
Pulmonary Hemorrhage with the CDC Case Definition
Prospective nationwide surveillance for cases of AIPH among infants is difficult to justify on the basis of the available epidemiologic data. In addition to the limitations reported for the Cleveland study
(5), no risk factors were conclusively
linked to disease in the Chicago investigation
(4), and only one other cluster (in Detroit) was reported during 1992--1996
(7).
CDC will retrospectively review cases of pulmonary hemorrhage to determine the public health impact of AIPH
among infants and to generate hypotheses regarding the importance of risk factors possibly associated with AIPH among infants.
If that review indicates that AIPH among infants is a separate clinical entity and that these cases have occurred in clusters, or that an increase in incidence or mortality is associated with these cases, CDC will initiate prospective surveillance and
case ascertainment to identify cases for epidemiologic studies
designed to confirm or disprove associations between
pulmonary hemorrhage host factors, environmental factors, and biologic agents, including such molds as
S. chartarum (5).
Retrospective Review by Using Existing Data Sources
The ability to use existing data sources should substantially facilitate both determining the public health impact of
AIPH among infants. However, the reliable data regarding mortality from pulmonary hemorrhage is only available at the national level. CDC conducted a preliminary evaluation of ICD codes for surveillance of pulmonary hemorrhage among infants to
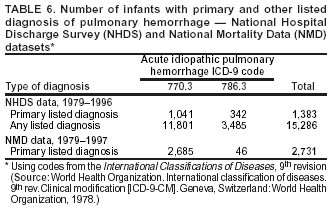
determine whether existing data sources can be used to estimate the magnitude of the problem of AIPH among infants. CDC examined data from the National Hospital Discharge Survey (NHDS) and National Mortality Data. Possible cases of AIPH among infants were identified by using ICD-9 codes 770.3, 784.7, 784.8, 786.3, and 516.1 (Table 6).
Infants identified by ICD-9 codes 770.3 and 786.3 differ from the cases reported in Cleveland. In the national datasets, the majority of cases of pulmonary hemorrhage had diagnoses such as prematurity or immaturity and death occurring within the first 7 days of life. The Cleveland cases occurred among stable, healthy, mature infants who had been discharged from the hospital to their homes after birth and subsequently experienced pulmonary hemorrhage
(8--10). Thus, the estimates of deaths and hospital admissions for cases of pulmonary hemorrhage using ICD codes 770.3 and 786.3 does not distinctly identify infants with AIPH as defined by CDC. In addition, these national datasets do not determine if infants had
identifiable etiologies or complications before their discharge from the hospital or their death. Because the estimated number
of hospitalized cases with a primary diagnosis of pulmonary hemorrhage was less than the number of deaths, these
national datasets might not be reliable for surveillance for infantile pulmonary hemorrhage. These analyses might be better
performed by using state-based data.
A retrospective review for AIPH among infants will be performed in metropolitan cities in those states with the
highest death rates and with >100 deaths associated with pulmonary hemorrhage among infants, on the basis of relevant ICD-9 and ICD-10 codes used from 1979 to the most recent available data. By focusing on PICUs and NICUs with substantial
numbers of deaths, cases from innercity catchment areas, where the incidence of AIPH among infants is suspected to be higher, will
be captured. Potential cases will be identified by using standardized methods of case ascertainment and data collection
from hospital discharge and mortality data sources, based on ICD codes. Potential cases will be compared with the
recommended case definition by reviewing medical records
related to all cases of pulmonary hemorrhage observed since 1979 among
children aged <2 years.
This retrospective review of AIPH among infants will
determine whether AIPH among infants is a distinct clinical entity within existing ICD-9/ICD-10 diagnostic codes
for pulmonary hemorrhage;
describe the epidemiology of pulmonary hemorrhage;
identify trends in the frequency of cases and the geographic distribution and clustering of cases;
estimate the public health impact of AIPH among
infants;
identify groups at high risk for AIPH among infants; and
determine the need for prospective surveillance as a source of cases for a case-control study.
The data will be reviewed to determine how these cases, including the apparent case clusters of AIPH among infants
in Cleveland and Chicago, have been coded on hospital discharge abstracts, and how deaths attributed to the syndrome have been characterized on death certificates. Both Ohio and Illinois meet the criteria of
>100 deaths from pulmonary hemorrhage.
In Cleveland and Chicago, this review also will determine the positive predictive value (PPV) between the clusters
of pulmonary hemorrhage cases previously reported and the CDC definition of AIPH among infants. Because
the relation between IPH, pulmonary hemorrhage, and AIPH among infants is not clearly understood in terms of rate,
etiology, and risk factors, this analysis will define basic demographics of cases among infants and whether the proposed case
definition for AIPH among infants is clearly distinguishable from other conditions. The magnitude and dimensions of AIPH
among infants will be determined by describing the distribution of cases on the basis of ICD codes and the CDC case definition. This will involve enumerating cases, determining hospital discharge and mortality rates, and describing the distributions
for available demographic variables (e.g., temporal and urban versus rural differences), if any.
Investigation of Suspected Clusters of AIPH Among Infants
If an apparent cluster of cases of pulmonary hemorrhage
occurs, CDC recommends that state health departments initiate
an investigation. CDC staff will work with each state, upon request, to evaluate case reports
to assist the epidemiologic and environmental investigation, if any. State health departments can use existing protocols for outbreak or cluster investigations and collect information to determine if cases meet the CDC case definition for AIPH among infants. Because these cases
probably will be identified in PICUs, CDC recommends that if PICU staff identify any suspected cases, they report them to their
state epidemiologist.
For each case of AIPH in an infant, CDC recommends that PICU and NICU staff collect clinical information to
certify case status, demographic information, and reports regarding the status of the patient's home. PICU and NICU staff
also should carefully document illnesses that are similar clinically to AIPH, even if another specific etiology is confirmed, because they might offer additional information or indicate the need to re-assess the case definition.
If performed, environmental assessment of the home to gather pertinent risk-assessment data should use standard protocols designed by trained environmental health professionals. At a minimum, the assessment should involve visual inspection, including checks for dampness, water damage,
obvious mold, evidence of pests, and environmental tobacco
smoke. Depending on the assessed need for further evaluation and the resources available, additional investigation might include determining moisture content, settled dust sampling, air sampling for different allergens, and biologically active compounds, and other investigations as needed.
Conclusion
CDC recommends a definition for a clinically confirmed case of AIPH among infants on the basis of 1) evidence of blood
in the airway; 2.) age <1 year; 3) absence of medical conditions related to pulmonary hemorrhage; and 4) severe acute respiratory distress or respiratory failure, requiring
admission to a PICU with intubation and mechanical ventilation. CDC recommends
that PICUs report cases that meet the CDC case definition to state health departments and to CDC.
CDC will retrospectively analyze state-level mortality and hospitalization data based on ICD codes and will
retrospectively review discharges for pulmonary hemorrhage in selected PICUs. These studies will
distinguish between the clinical findings associated with different symptoms of AIPH among infants;
determine whether ICD codes capture cases that meet the
CDC-recommended case definition for AIPH among infants;
determine whether AIPH among infants is a distinct recognizable clinical entity;
determine the proportion of cases ascertained retrospectively through ICD-9 codes that meet the clinical case definition by estimating PPV of ICD-coded data; and
define the magnitude of AIPH among infants and the need for conducting etiologic studies.
CDC will review the Cleveland and Chicago case series to determine the degree to which the present case
definition applies to them. In addition, CDC will evaluate the present case definition on the basis of data from initial
surveillance findings and modify it as appropriate.
If these reviews establish that AIPH among infants is a public health problem on the basis of increasing numbers or
clusters of cases geographically or temporally, targeted prospective case surveillance will be initiated. If prospective surveillance is initiated, CDC will maintain a database of current cases of AIPH among infants, reported by PICUs that meet the
case definition. The database will serve as a source of cases for case-control studies to determine etiology. CDC will work with
state and local health departments to investigate clusters of AIPH among infants cases.
Acknowledgments
The following CDC staff provided program support for this
report: Wesley J. Hodgson, James A. Rifenburg, Tammy T. Rowe, and
Sala S. Sharp, Division of Environmental Hazards and Health Effects, National Center for Environmental Health. We also thank
Dorr Dearborn, M.D., for reviewing draft manuscripts and for his feedback regarding portions of this report. We also thank Roy Baron, M.D., for sharing background documents from the internal and external panels that prepared the March 2001 CDC report regarding pulmonary hemorrhage.
References
World Health Organization. International classification of diseases.
9th rev. Clinical modification (ICD-9-CM). Geneva, Switzerland: World
Health Organization, 1978.
CDC. Update: pulmonary hemorrhage/hemosiderosis among infants---Cleveland, Ohio, 1993--1996. MMWR 1997;46:33--5.
CDC. Acute pulmonary hemorrhage among infants Chicago, April 1992--November 1994 [Current trends]. MMWR 1995;44:67--74.
CDC. Update: pulmonary hemorrhage/hemosiderosis among infants---Cleveland, Ohio, 1993--1996. MMWR 2000;49:180--4.
Hanzlick R. Pulmonary hemorrhage in deceased infants: baseline data for further study of infant mortality. Am J Forensic Med Pathol
2001;22:188--92.
Pappas MD, Sarnaik AP, Meert KL, Hasan RA, Lieh-Lai MW. Idiopathic pulmonary hemorrhage in infancy: clinical features and management
with high frequency ventilation. Chest 1996;110:553--5.
Etzel R, Montana E, Sorenson WG, et al. Acute pulmonary hemorrhage in infants associated with exposure to
Stachybotrys atra and other fungi. Arch Pediatr Adolesc Med 1998;152:757--62.
Novotny W, Dixit A. Pulmonary hemorrhage in an infant following 2 weeks of fungal exposure. Arch Pediatr Adolesc Med 2000;154:271--5.
Elidemir O, Colasurdo GN, Rossmann SN, Fan LL. Isolation of
Stachybotrys from the lung of a child with pulmonary hemosiderosis. Pediatrics 1999;104:964--6.
Consultants --- October 31, 2000
Chairs: James Buehler, M.D., CDC, Atlanta, Georgia, Case
Definition Panel Chair; David Warnock, Ph.D., CDC, Atlanta, Georgia,
Home/Indoor Environment and Laboratory Investigation Co-Chair and Chair,
Biological Agents Subpanel; Kenneth Martinez, M.S.E.E., CDC, Cincinnati,
Ohio, Home/Indoor Environment and Laboratory Investigation Panel Co-Chair
and Chair, Nonbiological Agents Subpanel; Steven MacDonald, Ph.D.,
Washington State Department of Health, Olympia, Washington and Council of
State and Territorial Epidemiologists, Atlanta, Georgia, Surveillance
Implementation Panel Chair, member of Case Definition and Home/Indoor
Environment and Laboratory Investigation Panels.
Members: Allen Cohen, M.D., Georgia Pediatric Pulmonary
Associates, Atlanta, Georgia; Mark Wylan, M.D., Mayo Clinic, Rochester,
Minnesota; Leland Fan, M.D., Baylor College of Medicine, Houston, Texas;
Claire Langston, M.D., Texas Children's Hospital, Houston, Texas; William
MacKenzie, M.D., Private Consultant Medical Epidemiologist, Atlanta,
Georgia; William Novotny, M.D., University Health Systems of East
Carolina, Greenville, North Carolina; Michael McGinnis, Ph.D., University
of Texas Medical Branch, Galveston, Texas; David Miller, Ph.D., Carleton
University and Health Canada, Ottawa, Ontario, Canada; Philip Morey,
Ph.D., Air Quality Sciences Inc, Atlanta, Georgia; Stephen Vesper, Ph.D.,
Environmental Protection Agency, Cincinnati, Ohio; Kenneth Dillon, Ph.D.,
University of Alabama, Birmingham, Alabama; Daniel Sudakin, M.D., Private
Consultant Medical Toxicologist, Portland, Oregon; Kenneth Orloff, Ph.D.,
CDC, Atlanta, Georgia; Bruce Jarvis, Ph.D., University of Maryland,
College Park, Maryland; Coreen Robbins, Ph.D., GlobalTox, Redmond,
Washington; Anthony Mansell, M.D., Rhode Island Hospital, Providence,
Rhode Island; Frances Dunston, M.D., Morehouse School of Medicine,
Atlanta, Georgia; Randy Hanzlick, M.D., Fulton County Office of the
Medical Examiner, Atlanta, Georgia; Richard Hopkins, M.D., Florida
Department of Health, Tallahassee, Florida, and Council of State and
Territorial Epidemiologists, Atlanta, Georgia; William Halperin, M.D.,
CDC, Cincinnati, Ohio; Lorann Stallones, Ph.D., Colorado State University,
Fort Collins, Colorado; Donald Mattison, M.D., March of Dimes, White
Plains, New York; Eugene Gangarosa, M.D., Private Consultant Medical
Epidemiologist, Atlanta, Georgia; Donald Millar, M.D., Private Consultant
Medical Epidemiologist, Atlanta, Georgia.
Observers: Laura Kolb, M.P.H., Environmental Protection Agency,
Washington, D.C.; Terry Allan, M.P.H., Cuyahoga County Health Department,
Cleveland, Ohio; Brian Shelton, M.P.H., PathCon Laboratories, Atlanta,
Georgia; Roy Baron, M.D., CDC, Atlanta, Georgia; Henry Slack, M.S.,
Environmental Protection Agency, Region IV, Atlanta, Georgia; Angela
Weber, M.S., CDC, Atlanta, Georgia; Brent Lasker, Ph.D., CDC, Atlanta,
Georgia; John Sobolowski, Cuyahoga County Health Department, Cleveland,
Ohio.
Use of trade names and commercial sources is for identification only and does not imply endorsement by the U.S. Department of
Health and Human Services.References to non-CDC sites on the Internet are
provided as a service to MMWR readers and do not constitute or imply
endorsement of these organizations or their programs by CDC or the U.S.
Department of Health and Human Services. CDC is not responsible for the content
of pages found at these sites. URL addresses listed in MMWR were current as of
the date of publication.
All MMWR HTML versions of articles are electronic conversions from ASCII text
into HTML. This conversion may have resulted in character translation or format errors in the HTML version.
Users should not rely on this HTML document, but are referred to the electronic PDF version and/or
the original MMWR paper copy for the official text, figures, and tables.
An original paper copy of this issue can be obtained from the Superintendent of Documents,
U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800.
Contact GPO for current prices.
**Questions or messages regarding errors in formatting should be addressed to
[email protected].