Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail.
Preventing Tetanus, Diphtheria, and Pertussis Among
Adolescents: Use of Tetanus Toxoid, Reduced Diphtheria Toxoid and
Acellular Pertussis Vaccines
Recommendations of the Advisory Committee on Immunization
Practices (ACIP)
Prepared by
Karen R. Broder, MD,1,5 Margaret M. Cortese,
MD,1,5 John K. Iskander,
MD,2,5 Katrina Kretsinger,
MD,1,5 Barbara A. Slade, MD,1
Kristin H. Brown,1 Christina M. Mijalski,
MPH,1 Tejpratap Tiwari, MD,1 Emily J. Weston,
MPH,1 Amanda C. Cohn,
MD,1,4,5 Pamela U. Srivastava,
MS,1 John S. Moran, MD,1,5 Benjamin Schwartz,
MD,3,5 Trudy V. Murphy, MD1
1Epidemiology and Surveillance Division, National Immunization Program, CDC
2Office of the Chief Science Officer, Office of the Director, CDC
3National Vaccine Program Office, DHHS 4EIS/Career Development Division, Office of Workforce and Career Development, CDC
5Commissioned Corps of the United States Public Health Service
The material in this report originated in the National Immunization Program, Anne Schuchat, MD, Director, Epidemiology and Surveillance Division,
Alison Mawle, PhD, Acting Director; and the Office of the Chief Science Officer, Dixie E. Snider, MD, Chief Science Officer, Immunization Safety Office,
Frank DeStefano, MD, Acting Director.
Corresponding preparer: Karen R. Broder, MD, National Immunization Program, CDC, 1600 Clifton Road, NE, MS E-61, Atlanta, GA 30333.
Telephone: 404-639-8538; Fax: 404-639-2483; E-mail: [email protected].
Summary
During spring 2005, two tetanus toxoid, reduced diphtheria toxoid and acellular pertussis vaccine (Tdap)
products formulated for use in adolescents (and, for one product, use in adults) were licensed in the United States
(BOOSTRIX®, GlaxoSmithKline
Biologicals,Rixensart, Belgium [licensed May 3, 2005, for use in persons aged
10--18 years], and
ADACEL™, sanofi pasteur, Toronto, Ontario, Canada [licensed June 10, 2005, for use in persons aged 11--64
years]). Prelicensure studies demonstrated safety and efficacy against tetanus, diphtheria, and pertussis when Tdap was administered
as a single booster dose to adolescents. To reduce pertussis morbidity in adolescents and maintain the standard of care for
tetanus and diphtheria protection, the Advisory Committee on Immunization Practices (ACIP) recommends that:
1) adolescents aged 11--18 years should receive a single dose of Tdap instead of tetanus and diphtheria toxoids vaccine (Td) for
booster immunization against tetanus, diphtheria, and pertussis if they have completed the recommended childhood diphtheria
and tetanus toxoids and whole cell pertussis vaccine (DTP)/ diphtheria and tetanus toxoids and acellular pertussis vaccine
(DTaP) vaccination series (five doses of pediatric DTP/DTaP
before the seventh birthday; if the fourth dose was administered on
or after the fourth birthday, the fifth dose is not needed) and have not received Td or Tdap. The preferred age for
Tdap vaccination is 11--12 years; 2) adolescents aged 11--18 years who received Td, but not Tdap, are encouraged to receive
a single dose of Tdap to provide protection against pertussis if they have completed the recommended childhood
DTP/DTaP vaccination series. An interval of at least 5 years between Td and Tdap is encouraged to reduce the risk for local and
systemic reactions after Tdap vaccination. However, an interval less than 5 years between Td and Tdap can be used; and 3)
vaccine providers should administer Tdap and tetravalent meningococcal conjugate vaccine
(Menactra®, sanofi pasteur,
Swiftwater, Pennsylvania) to adolescents aged 11--18 years during the same visit if both vaccines are indicated and available.
This statement 1) reviews tetanus, diphtheria and pertussis vaccination policy in the United States, with emphasis on
adolescents; 2) describes the clinical features and epidemiology of pertussis among adolescents; 3) summarizes the immunogenicity,
efficacy, and safety data of the two Tdap vaccines licensed for use among adolescents; and 4) presents recommendations for
tetanus, diphtheria, and pertussis vaccination among adolescents aged 11--18 years.
Introduction
Pertussis, an acute, infectious cough illness, remains endemic in the United States despite routine childhood
pertussis vaccination for more than half a century and high coverage levels in children for more than a decade
(1--4). A primary reason
for the continued circulation of Bordetella
pertussis is that immunity to pertussis wanes approximately 5--10 years
after completion of childhood pertussis vaccination, leaving adolescents and adults susceptible to pertussis
(5--10). Among the diseases for which universal childhood vaccination has been recommended, pertussis is the least well-controlled
reportable bacterial vaccine-preventable disease in the United States
(11,12).
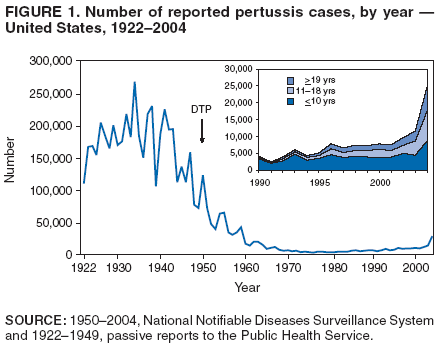
In the United States during 1934--1943, an annual average of 200,752 pertussis cases and 4,034 pertussis-related
deaths were reported (13). After the introduction of childhood pertussis vaccination during the 1940s, the number of
reported pertussis cases declined dramatically, reaching an historic low of 1,010 in 1976
(Figure 1) (1). Since the 1980s, the number
of reported pertussis cases has been steadily increasing, especially among adolescents and adults
(4,14,15). Possible reasons for the increase in reported pertussis cases include a true increase in the burden of disease and an increase in the detection
and reporting of cases; the relative contribution of each of these factors to the increase observed is unclear
(4,14--17).
Childhood Pertussis Vaccination Policy in the United States
Whole cell pertussis vaccines became available during the 1920s
(18), but pediatric diphtheria and tetanus toxoids
and whole cell pertussis vaccine (DTP) was not routinely recommended for children until the 1940s and 1950s
(19,20). In 1991, less reactogenic pediatric acellular pertussis vaccine (diphtheria and tetanus toxoids and acellular pertussis
vaccine [DTaP]) was first licensed for use in children for the fourth and fifth doses of the 5-dose childhood vaccination series in the United
States (21,22), and in 1996, pediatric DTaP was licensed for the first three infant doses
(1). In 1997, the Advisory Committee on Immunization Practices (ACIP) recommended that pediatric DTaP be used routinely instead of pediatric DTP as a
5-dose DTaP schedule at ages 2, 4, 6, 15--18 months and 4--6 years
(1,23); pediatric DTP has not been available in the United
States since 2002 (CDC, unpublished data, 2005).
Childhood and Adolescent Tetanus and Diphtheria Vaccination Policy in
the United States
Vaccination against tetanus and diphtheria has markedly reduced the number of cases and deaths from tetanus
and diphtheria in the United States in all age groups
(24). From 1997 through spring 2005, three vaccine formulations
against tetanus and diphtheria were recommended for use in the United States: pediatric DTaP routinely for children aged
<7 years, pediatric diphtheria and tetanus toxoids vaccine (DT) for children aged <7 years with contraindications or precautions
for pertussis components, and adult tetanus and diphtheria toxoids vaccine (Td) routinely for persons aged
>7 years (1,24) (Appendix A). The formulation of choice for vaccination of persons aged
>7 years has been Td rather than pediatric
DT because the lower diphtheria toxoid antigen content of Td induces an adequate immune response and lower rates of
adverse reactions in adults than pediatric DT
(24--28).
To provide continued protection against tetanus and diphtheria, ACIP recommended a booster dose of Td for adolescents
(24). Before 1995, the adolescent Td booster was recommended at age 14--16 years, approximately 10 years after completion of
the childhood DTP series. In 1995, the first harmonized childhood vaccination schedule endorsed by ACIP, the American Academy
of Pediatrics, and the American Academy of Family Physicians recommended lowering the age for Td administration to 11--12
years, but vaccination at age 14--16 years was also acceptable
(29). In 1996, ACIP, in collaboration with partner
organizations, recommended a routine vaccination visit at age 11--12 years to
reduce adolescent morbidity associated with
vaccine-preventable diseases and to improve vaccine coverage for adolescents
(30). The 1996 ACIP statement emphasized that the recommended age
for Td administration was 11--12 years, if at least 5 years had elapsed since administration of the last pediatric DTP/DTaP dose. Td
also was recommended for older adolescents who missed the Td dose at age 11--12 years. In some states, school attendance laws
continue to require that adolescents receive the Td dose 10 years after the last tetanus and diphtheria toxoids--containing vaccine, rather
than at age 11--12 years (CDC, unpublished data, 2005). After the adolescent Td booster dose, ACIP has recommended Td
boosters every 10 years throughout life
(24,31).
Licensure of Pertussis Vaccines for Use in Adolescents and Adults in
the United States
In spring 2005, two tetanus toxoid, reduced diphtheria toxoid and acellular pertussis vaccine (Tdap) products
were licensed in the United States for use in adolescents (and, for one product, use in adults)
(32,33). The pertussis antigen composition of the adolescent and adult Tdap formulations is similar to pediatric DTaP, but some of the pertussis antigens
are reduced in quantity. The tetanus and diphtheria toxoid composition of Tdap is similar to licensed adult formulations of
Td (Appendix A). No preparation containing pertussis antigens alone is licensed in the United States. Acellular pertussis
vaccines formulated for adolescents and adults have been available for use in other countries, including Canada, Australia, and
several European countries (e.g., France, Austria and Germany)
(10,34--40).
Background: Pertussis
General Clinical Characteristics
Pertussis is an acute respiratory infection caused by
Bordetella pertussis, a fastidious gram-negative coccobacillus.
The organism elaborates toxins that damage respiratory epithelial
tissue and have systemic effects, including promotion
of lymphocytosis (41,42). Other species of
Bordetella, including B. parapertussis,
and less commonly B. bronchiseptica or
B. holmesii, are associated with cough illness; the clinical presentation of
B. parapertussis can be similar to that of
classic pertussis. Illnesses caused by species of
Bordetella other than B. pertussis are not preventable by pertussis vaccines
(43).
Factors that affect the clinical presentation of pertussis
include age, the level of immunity, and use of antimicrobials early
in the course of the illness (44). The usual incubation period for pertussis is 7--10 days (range: 5--21 days)
(20,44,45). Classic pertussis is characterized by three phases of illness:
catarrhal, paroxysmal, and convalescent
(20,44,45). During the catarrhal phase, which generally lasts 1--2 weeks, infected persons experience coryza and an intermittent cough; high fever
is uncommon. The paroxysmal phase usually lasts 4--6 weeks and is characterized by spasmodic cough, posttussive
vomiting, and inspiratory whoop. Absolute lymphocytosis is common in unvaccinated children
(46). Symptoms slowly improve during the convalescent phase, which generally lasts 2--6 weeks, but can last months. Complications can occur during the course
of pertussis, including hypoxia, pneumonia, weight loss, seizures, encephalopathy, and death
(20,41,44,47).
Infants aged <12 months with pertussis are more likely than older age groups to have complications or be
hospitalized during their illness (16,47,48). During 2000--2004, an average of 2,488 cases of pertussis was reported annually
among infants aged <12 months. Among these infants, 63% were hospitalized, and the median duration of hospitalization was 5
days (range: 1--152 days) (CDC, unpublished data, 2005). Two to 3 doses of pediatric DTaP (recommended at ages 2, 4, and
6 months) provide protection against severe pertussis
(16,48,49). Young infants, who can present with symptoms of apnea
and bradycardia without cough, are at highest risk for death from pertussis
(16,47,48). During 1980--2004, a total
of 223 pertussis-related deaths in infants aged <4 months were reported to CDC (of 280 in all age groups)
(48, CDC, unpublished data, 2005). Of the 100 pertussis-related deaths reported during 2000--2004, a total of 90 (90%) were among young
infants aged <4 months and 76 (76%) were among infants aged <2 months (CDC, unpublished data, 2005).
B. pertussis is primarily transmitted from person to person through large respiratory droplets generated by coughing
or sneezing. Persons with pertussis are most infectious during the catarrhal and early paroxysmal phases of illness
(20,50). The disease is highly communicable, with attack rates as high as 80%--90% among nonimmune household contacts
(20,24,44). Adolescents with pertussis can transmit the disease to infants. A study conducted using enhanced pertussis surveillance
during 1999--2002 investigated the source of pertussis among infants aged <12 months. On the basis of parental interview, a
source was identified among 264 (43%) of 616 infant cases. An adolescent (defined in the study as a person aged 10--19 years)
was identified as the source for 43 (7%) of the 616 infants
(51).
Clinical Features and Morbidity Among Adolescents with Pertussis
The spectrum of disease caused by B.
pertussis in adolescents ranges from mild cough illness to classic
pertussis; infection also can be asymptomatic. When presentation is not classic, pertussis can be clinically indistinguishable from
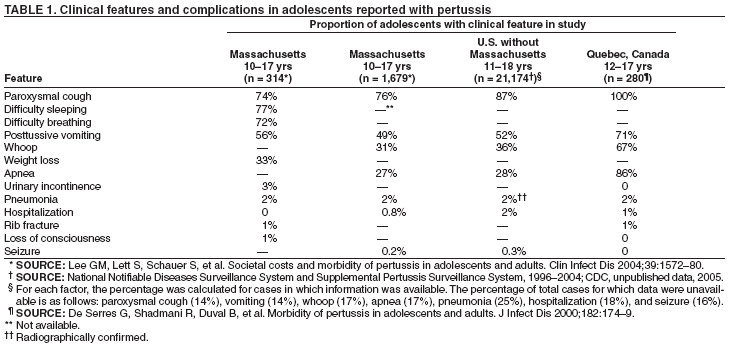
other respiratory illnesses. Adolescentsreportedwith pertussis commonly experience a prolonged cough illness and sometimes
have
complications (Table 1); rates of certain clinical characteristics and complications in these types of studies probably are
higher than among all adolescents with pertussis because the cases with a more classic presentation are more likely to be
diagnosed and reported (52--54; CDC, unpublished data, 2005). Complications and hospitalizations related to pertussis occur in up
to 2% of adolescents reported with pertussis (52,54;
CDC, unpublished data, 2005). Pertussis-related deaths are rarely
reported among adolescents; in the United States during 1990--2004, two pertussis-related deaths among adolescents aged 11--18
years were reported to CDC (one adolescent with malignancy and one adolescent with severe neurologic impairment)
(CDC, unpublished data, 2005). A prolonged cough is a common feature of pertussis in adolescents. A study in Quebec,
Canada, indicated that 97% of adolescents with pertussis coughed for
>3 weeks, and 47% coughed for >9 weeks
(52). Massachusetts surveillance data demonstrated that 38% of adolescents with pertussis reported during 1989--2004 had already been
coughing for >1 month at the time of diagnosis (Massachusetts Department of Public Health [MDPH], unpublished data, 2005).
Adolescents with pertussis often make repeated visits for medical care. Of approximately 7,000 Massachusetts
adolescents with pertussis reported during 1989--2004, 41% had one, 32% had two, and 24% had three or more medical visits
during their illness (MDPH, unpublished data, 2005). Adolescents with pertussis and their household contacts frequently miss
school or work. Of Massachusetts adolescents with pertussis, 83% missed school (mean: 5.5 days; range: 0.4--32 days). In 43%
of households with an affected adolescent, one parent or caretaker missed work (mean: 2.4 days, range:
0.1--25), and in 14% of households, a second parent or caretaker missed work (mean: 1.8 days, range:
0.1--11 days) (54).
Pertussis Diagnosis
Many factors affect the sensitivity, specificity, and interpretation of diagnostic tests for
B. pertussis, including the stage of the disease, antimicrobial administration, previous vaccination, the quality of technique used to collect the specimen,
transport conditions to the testing laboratory, experience of the laboratory, contamination of the sample, and use of
nonstandardized tests (55,56). In addition, tests and specimen collection materials might not be readily available to practicing clinicians.
Isolation of B. pertussis by culture is 100% specific; however, sensitivity of culture varies because fastidious
growth requirements make it difficult to transport and isolate the organism. Although the sensitivity of culture can reach
80%--90% under optimal conditions, in practice, sensitivity typically ranges from 30%--60%
(57). The yield of B. pertussis from
culture declines in specimens taken after 2 or more weeks of cough illness, after antimicrobial treatment, or after previous
pertussis vaccination (58). Within 3 weeks after onset of cough, culture is only 1%--3% sensitive
(59). Although B. pertussis can be isolated in culture as early as 72 hours after plating, it takes 1--2 weeks before a culture result can definitively be
called negative (60). Culture is essential to isolate
B. pertussis for antimicrobial susceptibility testing and for molecular subtyping
of strains.
Direct fluorescent antibody (DFA) tests provide rapid
results (hours), but are generally less sensitive (sensitivity:
10%--50%) than culture. With use of monoclonal reagents, the specificity of DFA should generally be >90%; however, the
interpretation of the test is subjective, and interpretation by an inexperienced microbiologist can result in lower specificity
(61). Because of the limitations of DFA testing, CDC does not recommend its use.
Because of increased sensitivity and shorter turn-around-time, DNA amplification (e.g., polymerase chain reaction
[PCR]) is being used more frequently to detect B.
pertussis. When symptoms of classic pertussis are present (e.g., 2 weeks
of paroxysmal cough), PCR typically is 2--3 times more likely than culture to detect a positive
B. pertussis sample (56,62,63). The interpretation of PCR-positive but culture-negative samples as either true positive or false positive is difficult. No
U.S. Food and Drug Administration (FDA)--licensed PCR test kit and no national standardized protocols, reagents, and
reporting formats are available. Approximately 100 different PCR protocols have been reported. These vary by DNA
purification techniques, PCR primers, reaction conditions, and product detection methods
(63). Laboratories must develop and
validate their own PCR tests. As a result, the analytical sensitivity, accuracy, and quality control of PCR-based
B. pertussis tests might vary widely among laboratories. The majority of laboratory validation studies have not sufficiently established the
predictive value of a positive PCR test to diagnose pertussis
(63). Use of PCR tests with low specificity can result in
unnecessary investigation and treatment of persons with false-positive PCR test results and inappropriate chemoprophylaxis of
their contacts (63). CDC Council of State and Territorial Epidemiologists (CSTE) reporting guidelines support the use of PCR
to confirm the diagnosis of pertussis only when the case also meets the clinical case definition
(>2 weeks of cough with paroxysms, inspiratory "whoop," or posttussive vomiting) (Appendix B)
(64,65).
Diagnosis of pertussis by serology generally requires demonstration of a substantial change in titer for pertussis
antigens (usually fourfold) when comparing results from acute
(<2 weeks after cough onset) and convalescent sera
(>4 weeks after the acute sample). The results of serologic tests on paired sera generally become available late in the course of illness and
can provide only retrospective diagnosis. A single sample serologic assay with age-specific antibody reference values is used as
a diagnostic test for adolescents and adults in Massachusetts but is not available elsewhere
(66). Other single-sample serologic assays lack standardization and do not clearly differentiate immune responses to pertussis antigens after
recent clinical disease, from more remote disease, or from vaccination
(43). None of these serologic assays, including the Massachusetts assay,
is licensed by FDA for routine diagnostic use in the United States. For these reasons, CDC guidelines for
laboratory confirmation of pertussis cases do not include
serologic testing.
The only pertussis diagnostic tests that the CDC endorses are culture and PCR (when the CDC/CSTE clinical
case definition is also met) (Appendix B). CDC-sponsored studies are underway to evaluate both serology and PCR testing.
CDC guidance on the use of pertussis diagnostics will be updated as results of these studies become available.
Incidence of Pertussis Among Adolescents
Pertussis is reportable in all 50 states and the District of Columbia. State health departments report confirmed and
probable cases of pertussis to CDC through the passive
National Notifiable Diseases Surveillance System (NNDSS);
additional information for pertussis cases is collected through the Supplemental Pertussis Surveillance System (SPSS)
(Appendix B) (4,16). During 2004, a total of 8,897 (34%) of the 25,827 reported U.S. cases occurred among adolescents aged 11--18
years (incidence for adolescents: 30 per 100,000 population); 17 states each reported >100 pertussis cases in adolescents
(12, CDC unpublished data, 2005*). The age distribution of the other pertussis cases reported in 2004 was 3,357 (13%) among
infants aged <1 years, 5,441 (21%) among children aged 1--10 years, and 7,481 (29%) among adults aged
>19 years (the age was unknown for 2.5% of the
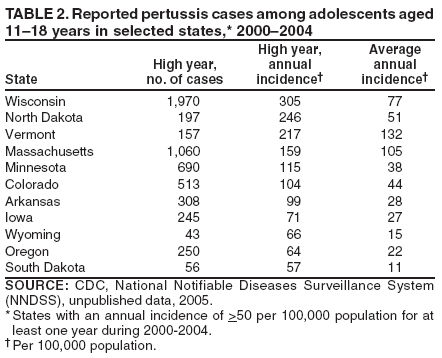
cases).The incidence of pertussis in adolescents varies widely among states and from
year-to-year. During 2000--2004, a total of 11 states had an annual incidence of reported pertussis in adolescents of
>50 per 100,000 population during at least 1 year
(Table 2) (12, CDC, unpublished data, 2005).
Data from enhanced surveillance sites and prospective
studies indicate that the national passive surveillance data
substantially underestimate the burden of pertussis among adolescents. Reliable diagnostic tests are not widely available, and not all
diagnosed cases are reported. Since the 1980s, MDPH has conducted enhanced surveillance for pertussis throughout
Massachusetts. MDPH uses an in-state, standardized serologic assay for pertussis diagnosis in adolescents and adults; educates
health-care providers, public health staff, and the general public about pertussis; and intensifies surveillance around cases, particularly
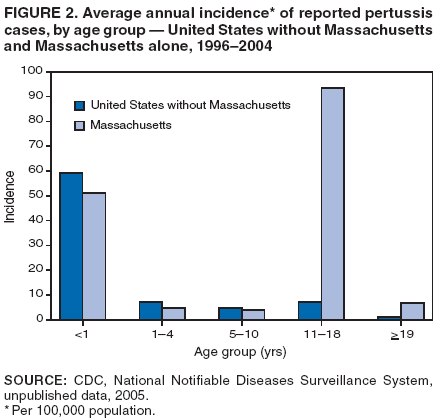
in school settings (17,66; MDPH, unpublished data, 2005). During 1996--2004, the average annual incidence of pertussis
in Massachusetts adolescents aged 11--18 years was 93 per 100,000 population, approximately 13 times greater than the
incidence of 7.3 reported for adolescents in the remainder of the United States
(Figure 2); reported rates among children aged <11
years were comparable between Massachusetts and the remainder of the United States (CDC, unpublished data, 2005).
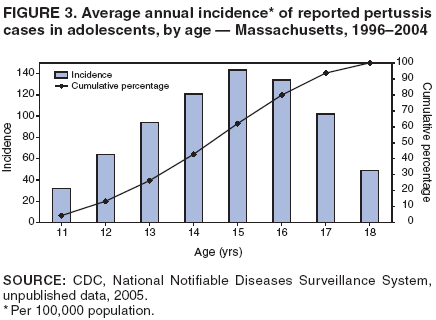
Massachusetts data indicated that 62% of reported pertussis cases in adolescents occurred before age 16 years, and 28% of reported
cases occurred before age 14 years, suggesting that pertussis booster vaccination early in adolescence could have a substantial impact
on the burden of pertussis in adolescents
(Figure 3) (CDC, unpublished data, 2005).
Two prospective studies in the United States have assessed the incidence of pertussis in populations that included
adolescents (67,68). In a Minnesota health maintenance organization during 1995--1996, persons aged 10--49 years were tested
for pertussis if they presented with an acute paroxysmal cough or a persistent cough illness of 7--34 days duration
(67). Cases were laboratory-confirmed using culture, PCR, and/or serology. On the basis of 27 identified cases, the estimated incidence
of laboratory-confirmed pertussis in this study was 507 per 100,000 person-years, and the incidence in adolescents
(estimated 997 per 100,000 person-years) was the highest of the age groups studied
(67). During 1997--2000, a study conducted at
sites in eight states estimated the incidence of pertussis among persons aged 15--64 years enrolled in the control arm of an
acellular pertussis vaccine trial (68). The incidence of pertussis, defined as an acute cough illness of at least 5 days with
laboratory confirmation, by culture, PCR, and/or serology, was 370 per 100,000
person-years. Applying less specific case definitions,
the study suggested approximately 1,000,000 cases of pertussis occur annually among persons aged
>15 years in the United States
(68).
Pertussis Outbreaks Involving Adolescents
High rates of pertussis in adolescents have been reported during community and statewide outbreaks. For example, in
a 1985 outbreak that occurred in a three-county region in semirural central Wisconsin, 32% of 161 cases of pertussis
occurred in adolescents aged 10--19 years for an incidence (using only culture-positive cases, the strictest case definition for
confirmed cases) of 150 per 100,000 population during the 8-month outbreak period
(69). Compared with the incidence of pertussis
in other age groups, the incidence of pertussis in adolescents was second only to that in infants aged <1 year (496 per
100,000 population) (69). In a statewide 1996 outbreak in Vermont, younger adolescents aged 10--14 years accounted for 36% of
280 cases and had the highest incidence (235 per 100,000 population) of all age groups during the outbreak period
(70).
Reported cases of pertussis in adolescents often occur in outbreaks at middle and high schools, where close
interaction occurs among large numbers of students with waning
vaccine-induced immunity to pertussis. Delay in the diagnosis
of pertussis contributes to the spread of pertussis in schools. Although the actual number of pertussis outbreaks in schools
across the United States is unknown, descriptions of pertussis outbreaks in middle and high schools from several states suggest
that these outbreaks are not uncommon. Surveillance data from Massachusetts during 2000--2004 indicated that
approximately 90% of the detected pertussis outbreaks (defined in Massachusetts as five or more cases linked in location and time)
occurred in schools. During this period, 41% of the reported pertussis cases in adolescents aged 11--19 years were identified
through school outbreaks (MDPH, unpublished data, 2005)
(Table 3).
Middle and high school outbreaks of pertussis can disrupt usual school functions and result in substantial public health
and school efforts to educate families, detect and treat cases, and provide chemoprophylaxis to close contacts. For example,
in 2001 in Pike County, Arkansas (population: 11,222), an outbreak of pertussis began among members of a school
football team (71; CDC, unpublished data, 2005). Among the 242 students in the county's middle and high school, 77
cases (attack rate: 32%) occurred, and the school was temporarily closed because of absenteeism. Of the students in the school,
93% had received at least 4 doses of pediatric DTP/DTaP during childhood. Countywide, 140 cases occurred in 109
households; 64% of the cases were reported among adolescents aged 12--18 years
(71; CDC, unpublished data, 2005). In July 2003,
in Fond du Lac County, Wisconsin (population: 97,296), initial detection of a pertussis outbreak occurred primarily
among students who used a high school weight room
(72; Wisconsin Division of Public Health, unpublished data, 2005). Of the
313 pertussis cases detected in the county over the 8-month outbreak period, 220 (70%) occurred among adolescents aged
10--19 years for an incidence of 1,505 per 100,000 population. A total of 92 cases occurred in six middle schools (range: 1--37
cases per school); 76 cases occurred among high school students (69 cases in one high school). An estimated 5,000 courses
of antimicrobials were prescribed during this pertussis outbreak
(72; Wisconsin Division of Public Health, unpublished
data, 2005).
Background: Tetanus and Diphtheria
Tetanus
Tetanus is unique among diseases for which vaccination is routinely recommended in that it is
noncommunicable. Clostridium tetani spores are ubiquitous in the environment and enter the body through nonintact skin. When inoculated
into oxygen-poor sites, such as necrotic tissue that can result from blunt trauma or deep puncture wounds,
C. tetani spores germinate to vegetative bacilli that multiply and elaborate tetanospasmin, a potent neurotoxin. Generalized tetanus
typically presents with trismus (lockjaw), followed by generalized
rigidity caused by painful contractions of the skeletal muscles that
can impair respiratory function. Glottic spasm, respiratory failure, and autonomic instability can result in death
(73). During 1998--2000, the case-fatality ratio for reported tetanus was 18% in the United States
(74).
Following widespread use of tetanus toxoid--containing vaccine during the 1940s, tetanus has become uncommon in the
United States, particularly in children and adolescents
(73,75). During 1990--2004, a total of 624 tetanus cases were reported; 19 (3%)
cases were among adolescents aged 11--18 years
(76; CDC, unpublished data, 2005). A 3-dose primary series of tetanus
toxoid--containing vaccine generally induces protective levels of antibody for tetanus that persist for
>10 years (73). Seroprotective rates
for tetanus, defined as an antitetanus concentration
>0.15 IU/mL (international units/milliliter), were obtained from a
population-based national serosurvey (National Health and Nutritional Examination Survey [NHANES] III) conducted in the United States
during 1988--1994. NHANES III was conducted when Td vaccination was recommended at age 14--16 years, before routine
Td
vaccination at age 11--12 years was implemented. Results
of NHANES III indicated approximately 80% of adolescents
aged 12--19 years had protective antitetanus concentrations
(77).
Neonatal tetanus usually occurs as the result of
C. tetani infection of the umbilical stump of an infant born to a mother
with a maternal antitetanus concentration insufficient to provide protection to the infant
(73). Neonatal tetanus is extremely rare in the United States: three cases were reported during 1990--2004. Two of the cases occurred among children born to
mothers who had no dose or 1 dose of a tetanus toxoid--containing vaccine, and the vaccination history of the third mother
was unknown (78,79; CDC, unpublished data, 2005).
Diphtheria
Respiratory diphtheria is an acute and communicable infectious illness caused by toxigenic strains of
Corynebacterium diphtheriae, and rarely by toxin-producing
C. ulcerans; disease is prevented by vaccination with diphtheria
toxoid--containing vaccines. Respiratory diphtheria is characterized by a
grayish-colored adherent membrane in pharynx, palate, or
nasal mucosa that can obstruct the airway. In addition, toxin-mediated cardiac and neurologic complications can
occur (80,81).
Reports of respiratory diphtheria are rare in the United States in all age groups
(80,82). During 1998--2004, seven cases of respiratory diphtheria were reported to CDC; one of the cases was imported
(11,12). The last culture-confirmed case of respiratory diphtheria in a U.S. adolescent was reported in 1996
(82). Data obtained from the NHANES III
serosurvey during 1988--1994 indicated that the prevalence of immunity to diphtheria, defined as an antidiphtheria concentration
of >0.1 IU/mL, was approximately 80% among adolescents aged 12--19 years
(77).
Exposure to diphtheria remains possible during travel to countries where diphtheria is endemic (information available
at http://www.cdc.gov/travel/diseases/dtp.htm) or from
imported cases. Respiratory diphtheria also can occur following
exposure to toxin-producing strains of C.
ulcerans; some cases have followed contact with dairy animals or consumption
of unpasteurized dairy products (80,83). Adherence to the ACIP-recommended schedule for tetanus and diphtheria
toxoid--containing boosters among adolescents and adults is important to prevent sporadic cases of respiratory
diphtheria. Information about the clinical management of diphtheria,
including use of diphtheria antitoxin, and the public
health response is available at
http://www.cdc.gov/nip/vaccine/dat/default.htm and reviewed elsewhere
(24,80,84).
Tetanus Toxoid, Reduced Diphtheria Toxoid and Acellular Pertussis
Vaccines for Adolescents
Criteria for Tdap Licensure
In the United States, two Tdap products were licensed for use in adolescents and, for one product, use in adults as a
single dose booster immunization against tetanus, diphtheria, and pertussis on the basis of clinical trials
demonstrating immunogenicity not inferior to U.S.- licensed Td or pediatric DTaP products and an overall safety profile
clinically comparable to U.S.-licensed Td products
(85,86). In a noninferiority trial, immunogenicity, efficacy, or safety endpoints
are demonstrated when a new product is at least as good as a comparator on the basis of a predefined and narrow margin for
a clinically acceptable difference between the study groups
(87). The efficacy of the tetanus and diphtheria toxoid component
of each Tdap was based on the immunogenicity of these antigens compared with U.S.-licensed Td using established
serologic correlates of protection (73,81). The percentage of persons achieving seroprotective antitetanus and
antidiphtheria concentrations (>0.1 IU/mL) and the booster response to each of these antigens 1 month postvaccination were evaluated.
In contrast to tetanus and diphtheria, no well-accepted
serologic or laboratory correlate of protection for
pertussis exists (88). A consensus was reached at the 1997 meeting of the Vaccines and Related Biological Products
Advisory Committee that clinical endpoint efficacy studies of acellular pertussis vaccines among adolescents or adults were not
required for Tdap licensure in these age groups. Rather, the efficacy of the pertussis components of Tdap administered to
adolescents and adults could be inferred using a serologic bridge to
infants vaccinated with pediatric DTaP during clinical
endpoint efficacy trials for pertussis (89). For each Tdap product, the immune response (geometric mean antibody
concentration [GMC]) of adolescents to each vaccine pertussis antigen after a single dose of Tdap was compared with the immune response
of infants after three doses of pediatric DTaP that
included the same pertussis components as the Tdap being
assessed (32,33). The
percentage of adolescents with a booster response to vaccine pertussis antigens exceeding a predefined lower limit for
an acceptable booster response also was evaluated.
The safety of Tdap was evaluated by comparing rates of
adverse events after vaccination in persons receiving Tdap
with those receiving Td. The overall safety profile of Tdap also was assessed.
Tdap Product Information
Data on immunogenicity and safety for the Tdap products licensed in the United States for use in adolescents (and, for
one product, use in adults) are presented separately below.
BOOSTRIX®
Indication
BOOSTRIX®, Tetanus Toxoid, Reduced Diphtheria Toxoid and Acellular Pertussis Vaccine, Adsorbed (Tdap)
(GlaxoSmithKline Biologicals [GSK], Rixensart, Belgium), was licensed on
May 3, 2005, for active booster immunization against tetanus,
diphtheria, and pertussis as a single dose in persons aged 10--18 years
(33).
Vaccine Composition
BOOSTRIX® contains the same tetanus toxoid, diphtheria toxoid, and three pertussis antigens (inactivated pertussis
toxin [PT], formaldehyde-treated filamentous hemagglutinin [FHA] and pertactin [69 kiloDalton outer membrane
protein] [PRN]), as those in
INFANRIX® (pediatric DTaP), but
BOOSTRIX® is formulated with reduced quantities of these
antigens (Appendix A). Each antigen is adsorbed onto aluminum hydroxide. Each dose of
BOOSTRIX® (0.5 mL) is formulated
to contain 5 Lf [limit of flocculation unit] tetanus toxoid, 2.5 Lf diphtheria toxoid, 8
µg inactivated PT, 8 µg FHA and 2.5
µg PRN. Each dose of
BOOSTRIX® also contains aluminum hydroxide
(<0.39 mg aluminum) as the adjuvant, 4.5 mg
NaCl, <100 µg residual formaldehyde, and
<100 µg polysorbate 80 (Tween 80) per 0.5--mL dose.
BOOSTRIX® contains no thimerosal or other preservative.
BOOSTRIX® is available in two presentations: a prefilled disposable syringe without a
needle and a single dose vial. The tip cap and rubber plunger of the needleless prefilled
syringe contain dry natural latex rubber; the single dose vial stopper preparation is latex-free
(33).
Immunogenicity and Serologic Bridge to Efficacy for Pertussis
A comparative, observer-blinded, multicenter, randomized controlled clinical trial conducted in the United States
evaluated the immunogenicity of the tetanus, diphtheria, and pertussis antigens in
BOOSTRIX® among adolescents aged 10--18
years (33,85). Adolescents were randomized 3:1 to
receive a single dose of BOOSTRIX® or a single dose of
TdMPHBL (manufactured by the Massachusetts Public Health Biologic Laboratories; contains diphtheria toxoid [2 Lf] and tetanus
toxoid [2 Lf]) (33,85). Serum samples were obtained before and approximately 1 month after vaccination
(85). All assays were performed by GlaxoSmithKline Biologicals in Rixensart, Belgium, using validated methods
(90).
Persons were eligible for enrollment if they were in good health and had completed routine childhood vaccination
against diphtheria, tetanus, and pertussis (approximately 98% of persons had received
>4 doses of pediatric DTP/DTaP). Persons were excluded if they had received the most recent pediatric DTP/DTaP during the preceding 5 years or Td during
the preceding 10 years, had a history of pertussis or household exposure to pertussis during the previous 5 years, had any of
the ACIP contraindications or precautions for pediatric DTP/DTaP
(91), had systemic allergic or neurologic reactions
or thrombocytopenia after a dose of tetanus or diphtheria toxoid--containing vaccine, had an acute illness, had received
blood products or immunoglobulins within 3 months, had any immunodeficiency, had significant underlying disease, had
certain neurologic disorders, or were pregnant
(33,85,92; GSK, unpublished data, 2005).
Tetanus and Diphtheria
Immune responses to tetanus and diphtheria toxoids were compared between the
BOOSTRIX® (range: 2,463--2,516
persons) and TdMPHBL (range: 814--834 persons) groups. One month postvaccination, the antitetanus seroprotective
(>0.1 IU/mL) and booster response rates in adolescents who had received a single dose of
BOOSTRIX® were noninferior to those who
received TdMPHBL. All adolescents had seroprotective antitetanus levels
>0.1 IU/mL 1 month after vaccination with either
BOOSTRIX® (95% confidence interval [CI] = 99.8%--100%) or
TdMPHBL (95% CI = 99.6%--100%). The booster response rate to
tetanus†
in the BOOSTRIX® group was 89.7% (95% CI = 88.4%--90.8%), compared with 92.5% (95%
CI = 90.5%--94.2%) in the TdMPHBL group
(33,92).
One month postvaccination, the antidiphtheria seroprotective
(>0.1 IU/mL) and booster response rates among
adolescents who received a single dose of
BOOSTRIX® were noninferior to those of adolescents who received
TdMPHBL. Among adolescents, 99.9% had seroprotective antidiphtheria levels
>0.1 IU/mL 1 month postvaccination with either
BOOSTRIX® (95% CI = 99.7%--100%) or
TdMPHBL (95% CI = 99.3%--100%). The booster response rate to
diphtheria† in the
BOOSTRIX® group was 90.6% (95% CI = 89.4%--91.7%), compared with 95.9% (95% CI = 94.4%--97.2%) in
the TdMPHBL group (33,92).
Pertussis
The efficacy of the pertussis components of
BOOSTRIX® was evaluated by comparing the immune responses
of adolescents vaccinated with a single dose of
BOOSTRIX® with the immune responses of infants vaccinated with 3 doses
of INFANRIX®. These infants were a subset of those vaccinated with
INFANRIX® in a German vaccine efficacy trial during
the 1990s (33,93).
BOOSTRIX® has the same three pertussis antigens as
INFANRIX® but in reduced quantities
(Appendix A). In the infant trial, the efficacy of 3 doses of
INFANRIX® against World Health Organization (WHO)-defined
typical pertussis (>21 days of paroxysmal cough with confirmation of
B. pertussis infection by culture and/or serologic testing)
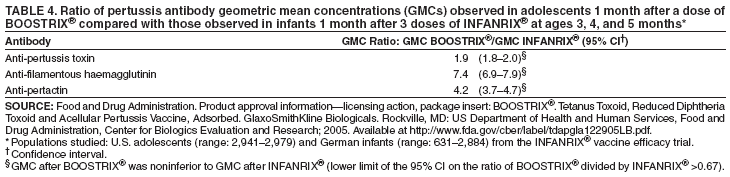
was 89% (95% CI = 77%--95%) (33,93). The anti-PT, anti-FHA, and anti-PRN GMCs of adolescents
1 month after a single dose of
BOOSTRIX® were noninferior to those of infants after 3 doses of
INFANRIX® (Table 4)
(33,85,92).
Booster response rates to the pertussis
antigens§ contained in
BOOSTRIX® (anti-PT, anti-FHA, and anti-PRN)
among adolescents (range: 2,677--2,752 persons) 1 month after
administration of BOOSTRIX® met prespecified criteria for
an acceptable response. Booster response rates to pertussis
antigens were anti-PT, 84.5% (95% CI = 83.0%--85.9%);
anti-FHA, 95.1% (95% CI = 94.2%--95.9%), and anti-PRN, 95.4% (95% CI = 94.5%--96.1%)
(33,92).
Safety
The primary safety study, conducted in the United States, was a randomized, observer-blinded, controlled study in
which 3,080 adolescents aged 10--18 years received a single dose of
BOOSTRIX®, and 1,034 received
TdMPHBL (see BOOSTRIX® Immunogenicity and Serologic Bridge to Efficacy for Pertussis for inclusion and exclusion criteria). Data on solicited local
and systemic adverse events were collected using standardized diaries for the day of vaccination and the next 14 consecutive
days (i.e., within 15 days following vaccination). Unsolicited and serious adverse events were collected for 6 months
following vaccination. No immediate events (within 30 minutes of vaccination) were reported in either vaccination group
(33,85,92).
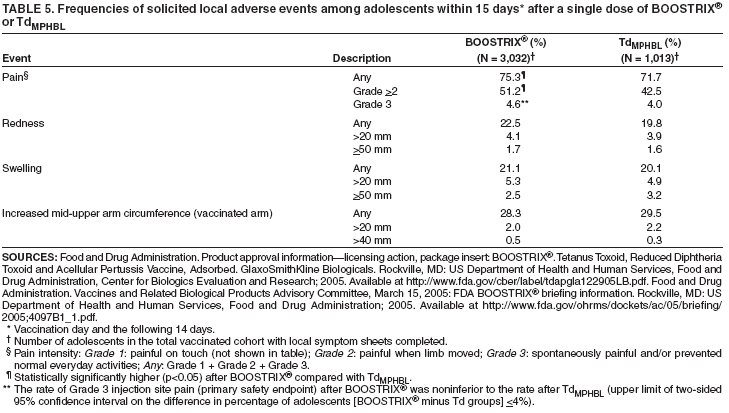
Solicited Local Adverse Events
Pain at the injection site was the most frequently reported solicited local adverse event in adolescents vaccinated
with BOOSTRIX® or
TdMPHBL. Within 15 days after vaccination, 75.3% of persons in the
BOOSTRIX® group and 71.7% of persons in the
TdMPHBL group reported pain of "any"
intensity (Table 5). The rates of any pain and grade 2 or 3
pain combined (but not grade 3 alone) were significantly higher (p<0.05) in BOOSTRIX® recipients compared with
TdMPHBL recipients (Table 5). However, the rates of grade 3 pain (primary safety endpoint) were similar in each group, and
the noninferiority criterion was met for
BOOSTRIX® compared with
TdMPHBL. No significant differences in the rates of
other solicited local adverse events (redness, swelling, and increase in arm circumference above baseline) were
observed between the two study groups
(33,85,92).
Two adolescents in the study reported "large injection-site swelling" after vaccination (predefined as any local swelling with
a diameter >100 mm and/or increased circumference of the injected limb >50 mm above baseline measurements
and/or any diffuse swelling that interfered with or prevented normal everyday activities). Both persons had onset of symptoms within
3 days of vaccination. One person who had received
BOOSTRIX® reported grade 3 pain (Table 5) with functional
impairment. This person was evaluated and treated with antimicrobials with symptom resolution within 3 days without sequelae.
The second person, who had received
TdMPHBL, reported grade 1 pain and did not seek medical attention. The duration
of symptoms was unknown, but symptoms resolved without sequelae
(85,90,92). No cases of whole-arm swelling were
reported in either vaccine group (GSK, unpublished
data, 2005).
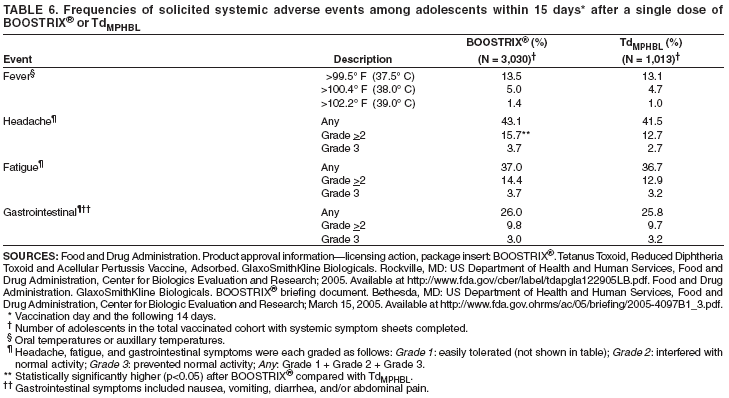
Solicited Systemic Adverse Events
The most frequently reported solicited systemic adverse events within 15 days following vaccination with
BOOSTRIX® or TdMPHBL were headache and
fatigue(Table 6). A statistically significantly higher rate of grade 2 or grade 3 headache
combined (but not grade 3 alone) (Table 6) was reported in the BOOSTRIX® group (15.7%), compared with the
TdMPHBL group (12.7%). The proportion of adolescents reporting fever
>100.4° F
(38.0° C) (5.0% for
BOOSTRIX® and 4.7% for
TdMPHBL), fatigue, and gastrointestinal systemic events were comparable in both groups
(33,85,92).
Serious Adverse Events
In the primary U.S. safety study, no serious adverse events (SAEs) occurred within 1 month postvaccination with
either BOOSTRIX® or
TdMPHBL. During the next 5 months of monitoring, SAEs were reported among 14 (0.4%) of the
3,005 adolescents vaccinated with
BOOSTRIX® and two (0.2%) of the 1,003 adolescents vaccinated with
TdMPHBL. No SAEs that were of potential autoimmune origin, new
onset and chronic in nature, or related to vaccination, as
determined by the investigators, were reported
(33,85,90,92). No seizures, cases of Guillain-Barré syndrome, or
physician-diagnosed Arthus reactions were reported
(33,85,90; GSK, unpublished data, 2005).
Simultaneous Administration with other Vaccines
Safety and immunogenicity of simultaneous administration of
BOOSTRIX® with other vaccines were not evaluated
during prelicensure studies (33).
ADACEL™
Indication
ADACEL™, Tetanus Toxoid, Reduced Diphtheria Toxoid and Acellular Pertussis Vaccine, Adsorbed (Tdap) (sanofi
pasteur, Toronto, Ontario, Canada) was licensed on June 10,
2005, for active booster immunization against tetanus, diphtheria, and
pertussis as a single dose in persons aged 11--64 years
(32).
Vaccine Composition
ADACEL™ contains the same tetanus toxoid, diphtheria toxoid, and five pertussis antigens as those in
DAPTACEL® (pediatric DTaP), but
ADACEL™ is formulated with reduced quantities of diphtheria toxoid and detoxified PT
(Appendix A). Each antigen is adsorbed onto aluminum phosphate. Each dose of
ADACEL™ (0.5 mL) is formulated to contain 5
Lf tetanus toxoid, 2 Lf diphtheria toxoid, 2.5
µg detoxified PT, 5 µg FHA, 3
µg PRN, and 5 µg fimbriae types 2 and 3
(FIM). Each dose of ADACEL™ also contains aluminum phosphate (0.33 mg aluminum) as the adjuvant,
<5 µg residual formaldehyde, <50 ng residual glutaraldehyde, and 3.3 mg
2-phenoxyethanol (not as a preservative) per 0.5--mL
dose. ADACEL™ contains no thimerosal.
ADACEL™ is available in single dose vials that are latex-free
(32).
Immunogenicity and Serologic Bridge to Efficacy for Pertussis
A comparative, observer-blinded, multicenter, randomized controlled clinical trial conducted in the United States
evaluated the immunogenicity of the tetanus, diphtheria, and pertussis antigens in
ADACEL™ among adolescents aged 11--17
years; adults aged 18--64 years were also studied and results are reported elsewhere
(32,86). Adolescents were randomized 3:2 to receive a single dose of
ADACEL™ or a single dose of
Tdsp (manufactured by sanofi pasteur; contains tetanus toxoid [5
Lf] and diphtheria toxoid [2 Lf]) (32,86). Sera from a subset of persons were obtained before and approximately
1 month after vaccination (32). All assays were performed at the immunology laboratories of sanofi pasteur in Toronto, Ontario, Canada
or Swiftwater, Pennsylvania, using validated methods
(86,94).
Persons were eligible for enrollment if they were in good health; completion of the childhood DTP/DTaP vaccination
series was not required. Persons were excluded if they had
received a tetanus, diphtheria, or pertussis vaccine within 5 years; had
a diagnosis of pertussis within 2 years; had an allergy
or sensitivity to any vaccine component; had a previous reaction to
a tetanus, diphtheria or pertussis vaccine, including
encephalopathy within 7 days or seizures within 3 days; had an
acute respiratory illness on the day of enrollment; had daily use of oral, nonsteroidal
anti-inflammatory drugs; had received blood products or immunoglobulins within
3 months; had any immunodeficiency; had significant
underlying disease; had neurologic impairment; or were pregnant
(32,94; sanofi pasteur, unpublished data, 2005).
Tetanus and Diphtheria
Immune responses to tetanus and diphtheria toxoids were compared between the
ADACEL™ (N = 527) and
Tdsp (range: 515--516 persons) groups. One month postvaccination, the antitetanus seroprotective
(>0.1 IU/mL) and booster response rates among adolescents who received
ADACEL™ were noninferior to those who received
Tdsp. All adolescents (95% CI = 99.3%--100% for both groups) had seroprotective antitetanus levels
>0.1 IU/mL 1 month after vaccination with
either ADACEL™ or Tdsp. The booster response rate to
tetanus¶ in the
ADACEL™ group was 91.7% (95% CI =
89.0%--93.9%) and 91.3% (95% CI = 88.5%--93.6%) in the
Tdsp group (32,86,94). One month postvaccination, the
antidiphtheria seroprotective (>0.1 IU/mL) and booster
response rates among adolescents who received a single dose of
ADACEL™ were noninferior to those who received
Tdsp. Among adolescents, 99.8% (95% CI = 98.9%--100%) had protective
antidiphtheria levels >0.1 IU/mL 1 month after vaccination with either
ADACEL™ or Tdsp. The booster
response rate to diphtheria¶ in
the ADACEL™ group was 95.1% (95% CI = 92.9%--96.8%) and 95.0% (95% CI = 92.7%--96.7%) in the
Tdsp group (32,86,94).
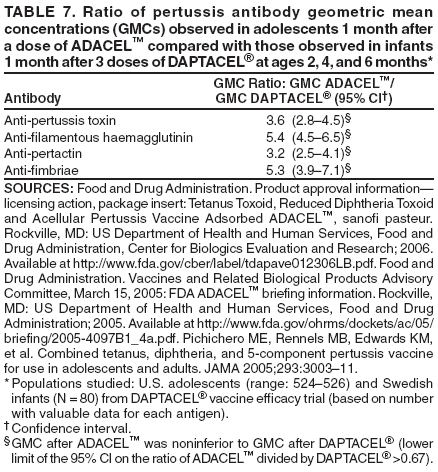
Pertussis
The efficacy of the pertussis components of
ADACEL™ was evaluated by comparing the immune responses of
adolescents vaccinated with a single dose of
ADACEL™ with the immune responses of infants vaccinated with 3 doses of
DAPTACEL® in a Swedish vaccine efficacy trial during the 1990s
(32,95). ADACEL™ and
DAPTACEL® contain the same five
pertussis antigens, except ADACEL™ contains one fourth the quantity of detoxified PT in
DAPTACEL® (96) (Appendix A). In
the Swedish trial, efficacy of 3 doses of DAPTACEL® against WHO-defined pertussis
(>21 days of paroxysmal cough with confirmation of
B. pertussis infection by culture and/or serologic testing or an epidemiologic link to a household member
with culture-confirmed pertussis) was 85% (95% CI = 80%--89%)
(29,87). The anti-PT, anti-FHA, anti-PRN, and
anti-FIM GMCs of adolescents 1 month after a single dose of
ADACEL™ were noninferior to those of
infants following three doses of
DAPTACEL® (32,94)
(Table 7).
Booster response rates to the pertussis antigens** contained in
ADACEL™ (anti-PT, anti-FHA, anti-PRN,
anti-FIM) among adolescents (range: 524--526 persons) 1 month following administration of
ADACEL™ met prespecified criteria
for an acceptable response. Booster response rates to pertussis antigens were anti-PT, 92.0% (95% CI = 89.3%--94.2%);
anti-FHA, 85.6% (95% CI = 82.3%--88.4%); anti-PRN, 94.5% (95% CI = 92.2%--96.3%); and anti-FIM 94.9% (95% CI
= 92.6%--96.6%) (32,94).
Safety
The primary adolescent safety study, conducted in the United States, was a randomized, observer-blinded, controlled
study in which 1,184 adolescents aged 11--17 years received a single dose of
ADACEL™ and 792 received
Tdsp (see ADACEL™ Immunogenicity and Serologic Bridge to Efficacy for
Pertussisfor inclusion and exclusion criteria)
(32). Adults aged 18--64 years were also studied; those results are reported elsewhere
(32). Data on solicited local and systemic adverse events
were collected using standardized diaries for the day of vaccination and the next 14 consecutive days (i.e., within 15 days
following vaccination) (32).
Immediate Events
Eleven adolescents experienced immediate events within 30 minutes of vaccination
(ADACEL™, six persons [0.5%] and
Tdsp, five persons [0.6%]); all events resolved without sequelae. Immediate events included dizziness, syncope, or
vasovagal reactions and pain and erythema at the injection site. No anaphylaxis was reported
(86,94,96).
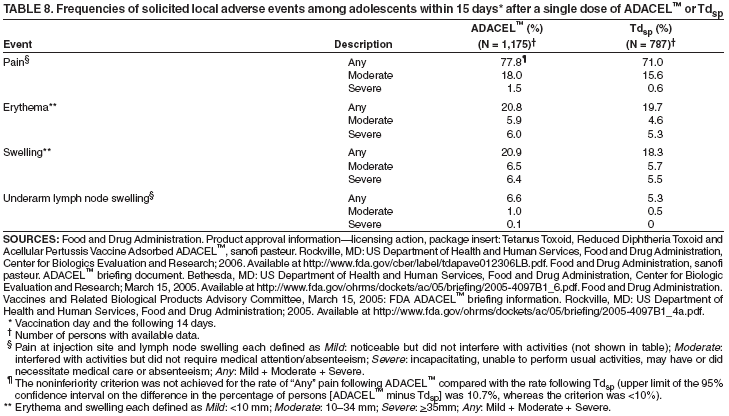
Solicited Local Adverse Events
Pain at the injection site was the most frequently reported solicited local adverse event among adolescents in
both vaccination groups (Table 8). Within 15 days following vaccination, reports of pain of "any" intensity were more
common among adolescents vaccinated with ADACEL™ (77.8%) than among those vaccinated with
Tdsp (71.0%). The noninferiority criterion was not achieved for the rate of any pain following
ADACEL™ compared with the rate following
Tdsp. Rates of moderate/severe pain, erythema, and swelling following
ADACEL™ were comparable to the rates following
Tdsp (32,86,94). No cases of whole-arm swelling were reported in either vaccine group
(94).
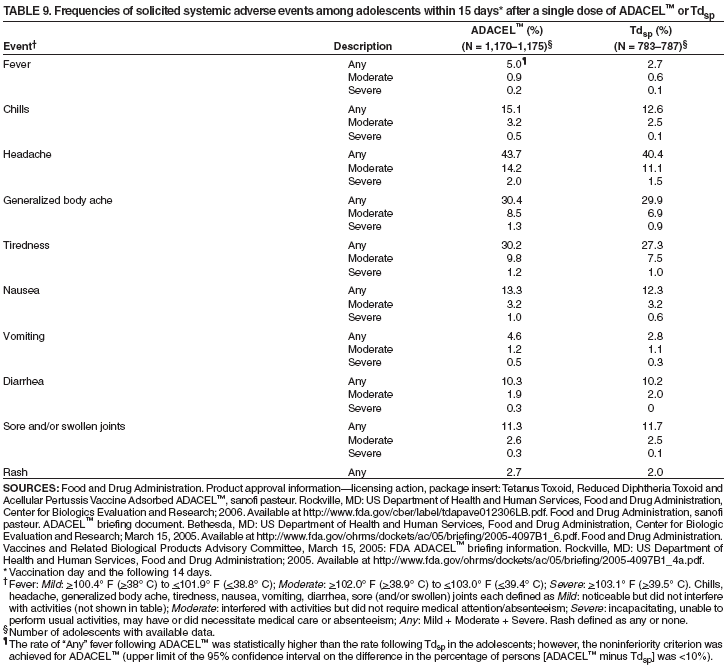
Solicited Systemic Adverse Events
The most frequently reported solicited systemic adverse events within the 15 days following vaccination were
headache, generalized body aches, and tiredness
(Table 9). The proportion of adolescents reporting fever
>100.4° F (>38° C)
following vaccination was statistically significantly higher among adolescents vaccinated with
ADACEL™ (5.0%) than
Tdsp (2.7%), but noninferiority criterion for
ADACEL™ was achieved. The rates of the other solicited systemic adverse events were
comparable between the ADACEL™ and
Tdsp groups (32,94).
Serious Adverse Events
In the primary adolescent safety study, SAEs within 6 months after vaccination were reported among 11 (0.9%) of
the 1,184 adolescents aged 11--17 years vaccinated with
ADACEL™ and eight (1.0%) of the 792 adolescents vaccinated
with Tdsp. Two adolescents (one
ADACEL™ recipient and one Tdsp
recipient) reported seizure events after vaccination;
both persons had a history of seizure disorder. SAEs in adolescents were reported by the study investigators to be unrelated to
the study vaccine (94).
The safety of ADACEL™ among adults also was studied. In the primary adult safety study, SAEs within 6 months
after vaccination were reported among 33 (1.9%) of the 1,752 adults aged 18--64 years vaccinated with
ADACEL™ and 11 (1.9%) of the 573 adults vaccinated with
Tdsp. Two of these SAEs were neuropathic events in
ADACEL™ recipients and were assessed by the investigators as possibly related to the study vaccine; in both cases, the symptoms resolved completely
over several days (32,86,94,96). No physician-diagnosed Arthus reactions or cases of Guillain-Barré syndrome were reported in
any adolescent or adult (32,86,96; sanofi pasteur, unpublished data, 2005).
Simultaneous Administration with Other Vaccines
Hepatitis B Vaccine
Safety and immunogenicity of
ADACEL™ co-administered with hepatitis B vaccine (Recombivax
HB®, Merck and Co., Inc., White House Station, New Jersey) was evaluated in adolescents aged 11--14 years using methods similar to the
primary ADACEL™ studies. Adolescents were randomized to one of two groups. In one group,
ADACEL™ and hepatitis B vaccine were administered simultaneously in different arms (simultaneous group; N = 206). In the other group,
ADACEL™ was administered first, followed by hepatitis B vaccine 4--6 weeks later (sequential group; N = 204)
(32; sanofi pasteur, unpublished data, 2005). No interference was
observed in the immune responses to any of the vaccine antigens
when ADACEL™ and hepatitis B vaccine were administered simultaneously or
sequentially†† (32).
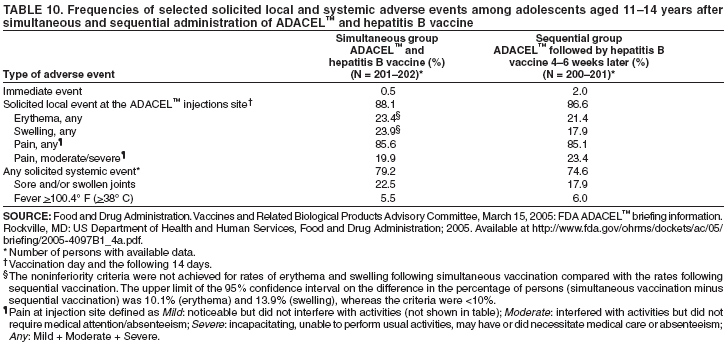
Adverse events were solicited only after
ADACEL™ vaccination (not hepatitis B vaccination)
(86). Within 15 days of vaccination, the reported rates of injection site pain (at the
ADACEL™ site) and fever were comparable when
ADACEL™ and hepatitis B vaccine were administered simultaneously or sequentially
(Table 10). However, rates of erythema and
swelling at the ADACEL™ injection site were higher in the simultaneous group than the sequential group, and noninferiority
criteria for simultaneous vaccination were not achieved (Table 10)
(86). Swollen and/or sore joints were reported in 22.5% of
persons in the simultaneous group and 17.9% of persons in the sequential group. Most joint complaints were mild in intensity and
the mean duration was 1.8 days (86).
Trivalent Inactivated Influenza Vaccine
Safety and immunogenicity of
ADACEL™ co-administered with trivalent inactivated influenza vaccine ([TIV]
Fluzone®, sanofi pasteur, Swiftwater, Pennsylvania) was evaluated in adults aged 19--64 years using methods similar to the
primary ADACEL™ studies (32). The immunogenicity data are presented elsewhere
(32). The adults were randomized to one of
two groups. In one group, ADACEL™ and TIV were administered simultaneously in different arms (simultaneous group; N
= 359). In the other group, TIV was administered first, followed by
ADACEL™ 4--6 weeks later (sequential group; N =
361) (32; sanofi pasteur, unpublished data, 2005).
Adverse events were solicited only after
ADACEL™ vaccination (not TIV)
(86). Within 15 days of vaccination, rates of erythema, swelling, and fever were comparable in both vaccination groups.
However, the rate of pain at the
ADACEL™ injection site was higher in the simultaneous group (66.6%) than the sequential
group (60.8%), and did not meet the noninferiority criterion (upper limit of the 95% CI on the difference in percentage of
persons [the rate following simultaneous vaccination minus the rate following sequential vaccination] was 13.0%, and the
criterion was <10%) (86).
Other Vaccines
Safety and immunogenicity of simultaneous administration of
ADACEL™ with other vaccines were not evaluated
during prelicensure studies (32).
Studies of Adolescent Acellular Pertussis Vaccine Impact
Clinical Efficacy Trial
The efficacy against pertussis of an adolescent and adult acellular pertussis (ap) vaccine with the same pertussis
antigens included in BOOSTRIX® (without tetanus and diphtheria toxoids) was evaluated in 2,781 adolescents and adults in
a prospective, randomized trial (68). Results of this study were not considered as part of Tdap licensure in the United States
(see Criteria for Tdap Licensure). Persons aged 15--64 years were randomized to receive one dose of ap vaccine or hepatitis
A vaccine (Havrix®, GlaxoSmithKline Biologicals, Rixensart, Belgium). The primary outcome measure was confirmed
pertussis, defined by a cough illness lasting
>5 days with laboratory evidence of B.
pertussis infection by culture, PCR, and/or
serologic testing results (acute and convalescent). Nine
persons in the hepatitis A vaccine control group and one
person in the ap vaccine group had confirmed pertussis during the study period; vaccine efficacy against confirmed pertussis was 92% (95% CI =
32%--99%) (68).
Economic Studies
The societal costs of pertussis are important, and universally vaccinating adolescents against pertussis is likely to be
cost effective. In one study, the economic impact of pertussis among Massachusetts adolescents aged 10--17 years was
evaluated using the state's enhanced pertussis surveillance system
(54). The mean medical cost per adolescent case of pertussis was
an estimated $201 and $256 for mild and severe cases of cough illness, respectively (in 2004 dollars), excluding the cost
of providing antimicrobials to close contacts of the
case-adolescents (53,54). The largest proportion of this cost was for
medical office visits and antimicrobial therapy
(54). When indirect, nonmedical costs (e.g., missed time from work for parents
of adolescents) were included, total societal cost of an adolescent case of pertussis was $361 and $416 for mild and severe
cough illness, respectively (in 2004 dollars)
(53,54).
Two U.S. economic studies have compared adolescent vaccination with other pertussis vaccination strategies
(53,97). Both studies identified a single dose of Tdap during adolescence as the most cost-effective strategy, under
different assumptions about pertussis incidence, waning immunity, vaccine efficacy, vaccine coverage, and infant transmission. In
the first study, a cost-benefit analysis was conducted to compare seven adolescent and/or adult pertussis
vaccination strategies during a 10-year interval (2001--2010), using a single dose of a Tdap. In this analysis, the incidence
of pertussis among adolescents and adults was estimated from prospective studies to be 450--507 cases per 100,000 population.
Strategies included vaccinating all adolescents aged 10--19 years, vaccinating all persons aged
>10 years (i.e., universal adolescent
and adult vaccination), vaccinating adolescents and adults aged
>15 years that were the primary care-takers of infants,
and four other adult vaccination strategies. Among these strategies, vaccinating all adolescents was identified as the most
cost-effective strategy. Universal adolescent Tdap vaccination was cost-saving to society when the Tdap vaccine and program costs were
<$37 (2002 dollars) per adolescent vaccinated
(97).
In a second study, six adolescent and/or adult Tdap vaccination strategies were compared by modeling health outcomes
over the course of a lifetime for hypothetical cohort of 4 million adolescents
(53). Incidence rates of pertussis among
adolescents and adults were estimated from Massachusetts surveillance data; baseline estimates were 155 and 11 per 100,000
population for adolescents and adults, respectively. The six strategies included no adolescent or adult vaccination, one-time
adolescent vaccination at age 11 years, one-time adult vaccination, adult vaccination with decennial Tdap boosters, adolescent and
adult vaccination with decennial Tdap boosters, and postpartum vaccination. The study assumed an incremental increase in
Tdap price of $15 compared with Td, with a Tdap vaccination cost of $25 per person vaccinated. Universal adolescent
vaccination was the most cost-effective strategy. Vaccinating all adolescents once would cost $1,100 per pertussis case prevented
or $20,000 per quality adjusted life year (QALY) saved, both in 2004 dollars. By contrast with the cost-benefit
analysis (97), which estimated the incidence of pertussis in adolescents to be approximately 3 times higher, Tdap vaccination was
not cost-saving under the second study's baseline assumptions
(53). In a sensitivity analysis, results from the second study
found
that if the incidence of adolescent and adult pertussis was four times the base-case estimates, universal adolescent
Tdap vaccination would be cost-saving to society
(53).
Other Tetanus and Diphtheria Toxoids Vaccine Preparations for Adolescents
Four Td (Tetanus and Diphtheria Toxoids, Adsorbed for Adult Use) vaccines are licensed in the United States
for active immunization against tetanus and diphtheria among persons aged
>7 years (98--101). Two tetanus toxoid vaccines
(TT) also are licensed for use in this age group
(102,103). Of the two TT products, one is adsorbed and is licensed for use
in situations in which the combined antigen preparation (Td) is not indicated
(102). The second TT preparation is a fluid vaccine (not adsorbed) and is indicated only for booster doses, not for primary immunization
(103). Although TT is licensed in the United States for persons aged
>7 years, Td has been preferred for routine use to provide dual protection against
tetanus and diphtheria (24) (Appendix A).
Safety Considerations for Adolescent Vaccination with Tdap or Td
Prelicensure Tdap studies support the safety of these vaccines
(32,33). However, sample sizes were insufficient to
detect rare adverse events, a limitation of prelicensure trials. Enrollment criteria excluded persons who had received vaccines
containing tetanus toxoid, diphtheria toxoid, or pertussis components during the preceding 5 or 10 years
(85,86,92,94). In addition, persons with certain neurologic conditions or events following pediatric DTP/DTaP vaccination were excluded from
these studies (85,92,94). Therefore, in making recommendations on the spacing and administration sequence of vaccines
containing tetanus toxoid, diphtheria toxoid, and/or pertussis components and on vaccination of adolescents with a history of
certain neurologic conditions or adverse events after vaccination, ACIP considered data from a range of pre- and postlicensure
studies of Tdap and other vaccines containing these components. Safety data being collected from the Vaccine Adverse
Event Reporting System (VAERS) and postlicensure studies will facilitate detection of potential adverse reactions
following widespread use of Tdap in adolescents (see Reporting of Adverse Events after Vaccination)
(104,105).
Spacing and Administration Sequence of Vaccines Containing Tetanus
Toxoid, Diphtheria Toxoid, and Pertussis Antigens
Historically, moderate and severe local reactions following tetanus and diphtheria toxoid--containing vaccines have
been associated with older, less purified vaccines, larger doses of toxoid, and frequent dosing at short intervals
(106--111). In addition, high pre-existing antibody titers to tetanus or diphtheria toxoids in children, adolescents, and adults primed
with these antigens might be associated with increased rates of local reactions to booster doses of tetanus or diphtheria
toxoid--containing vaccines (26,108,111,112). Two adverse events of particular clinical interest have been associated with
vaccines containing tetanus toxoid, diphtheria toxoid, and/or pertussis antigens, extensive limb swelling (ELS), and Arthus reactions.
Extensive Limb Swelling
ELS reactions have been described following doses of pediatric DTaP and other vaccines
(28,91,113--117). In retrospective analyses, 2%--3% of children receiving the fourth or fifth booster doses of pediatric DTaP experienced extensive
proximal limb swelling; swelling is usually greatest by 48 hours after vaccination
(28,118). ELS is generally not disabling, is not
often brought to medical attention, and resolves without complication within 4--7 days
(118). ELS has been reported to VAERS almost as frequently following Td as following
pediatric DTaP; among adolescents, the majority of reported cases of ELS
have involved either Td or hepatitis B vaccine
(117). The pathogenesis of ELS is not well understood; this reaction has
not consistently been related to the content of tetanus toxoids, diphtheria toxoids, pertussis antigens, or aluminum adjuvants
in vaccines (28,118,119). Whether children who experience ELS after receipt of pediatric DTaP are at
increased risk for ELS after receipt of Tdap is unknown.
Because these reactions typically resolve without sequelae, ACIP does not consider a
history of ELS following pediatric DTaP or any other vaccine to be a precaution or contraindication for pediatric DTaP
(91,113).
Arthus Reactions
Arthus reactions (type III hypersensitivity reactions) are rarely reported after vaccination and can occur after tetanus
toxoid--containing or diphtheria toxoid--containing vaccines
(24,111,120--124; CDC, unpublished data, 2005). An Arthus
reaction is a local vasculitis associated with deposition of
immune complexes and activation of complement. Immune complexes
form in the setting of high local concentration of vaccine antigens and high circulating antibody concentration
(111,120,121,125). Arthus reactions are characterized by
severe pain, swelling, induration, edema, hemorrhage, and
occasionally by necrosis. These symptoms and signs usually occur 4--12 hours after vaccination; by contrast, anaphylaxis (immediate type
I hypersensitivity reactions) usually occur within minutes of vaccination. As with ELS, Arthus reactions usually resolve
without sequelae. ACIP has recommended that persons who experienced an
Arthus reaction after a dose of tetanus
toxoid--containing vaccine should not receive Td more frequently than every 10 years, even for tetanus prophylaxis as part of wound
management (24).
Interval between Td and Tdap
ACIP has recommended a 10-year interval for routine
administration of Td and a 5-year minimum interval between the
last pediatric DTaP and the adolescent Td dose
(24,30). Administration of Td at short intervals might increase the risk for adverse
events (108,109). Prelicensure clinical trials of Tdap excluded persons who had received doses of a diphtheria or
tetanus toxoid--containing vaccine during the preceding 5
or 10 years (see BOOSTRIX® and
ADACEL™ sections on Immunogenicity
and Serologic Bridge to Efficacy for Pertussisfor exclusion criteria) (90,94,96). Although administering Td more often than every 10 years (5 years for
a tetanus-prone wound) is not necessary to provide protection against tetanus or diphtheria, administering a dose of Tdap less than
5 years after Td could provide a health benefit by protecting against pertussis.
The safety of administering a dose of Tdap at intervals less than 5 years after pediatric DTP/DTaP or Td was evaluated
in Canada following the country's licensure of Tdap
(ADACEL™) (126). The largest Canadian study was a
nonrandomized, open-label study of 7,001 students aged
7--19 years residing in Prince Edward Island. This study assessed the rates of
adverse events after Tdap and compared reactogenicity of Tdap administered at year intervals of 2--9 years (eight cohorts) versus
>10 years after the last tetanus and diphtheria toxoid--containing vaccine (Td, or pediatric DTP or DTaP). A year interval
was defined as the integer year +0.5 years (e.g., the 2-year interval was defined as >18 months to
<30 months). Vaccination history for type of pertussis vaccine(s) received (pediatric DTP and DTaP) also was
assessed. The number of persons assigned to cohorts ranged from 464 in the 2-year to 925 in the 8-year cohorts. Among the persons in the 2-year cohort, 214
(46%) received the last tetanus and diphtheria toxoid--containing vaccine 18--23 months before Tdap. Adverse event diary cards
were returned for 85% of study participants with a known interval; 90% of persons in the 2-year interval cohort provided
safety data (126).
Four SAEs were reported in the Prince Edward Island study; none were assessed by the investigators to be related to
vaccine. No Arthus reaction was reported. Rates of reported
severe local adverse reactions, fever, and any pain were not increased
in persons who received Tdap at intervals less than 10 years. Rates of local reactions were not increased among persons
who received 5 doses of pediatric DTP, with or without Td (intervals of 2--3 years or 8--9 years). Rates of any erythema and
any swelling were reported more frequently in cohorts that had received at least 1 or 2 doses of pediatric DTaP (intervals of
4--7 years), suggesting that increased rates of local reactions might occur more commonly among adolescents who
received pediatric DTaP vaccines, compared with those who received a 5-dose pediatric DTP series. Limb swelling (>100
mm) was reported in 0.2% of participants and was unrelated to the interval since the last tetanus and diphtheria
toxoid--containing vaccine (126).
A study was conducted in Germany to evaluate the safety of Tdap
(BOOSTRIX®) in persons aged 9--13 years
who received a 5-dose all acellular pertussis vaccine schedule
(5 doses of INFANRIX®, N = 193 or 4 doses of
INFANRIX® plus another acellular pertussis vaccine, N = 126); the interval from the fifth to sixth dose of the acellular pertussis vaccines
ranged from approximately 5--6 years (GSK, unpublished data, 2005). Within 15 days after vaccination, any pain (63.6%),
erythema (51.7%), and swelling (41.4%) were frequently
reported symptoms, but the rate of "large injection site swelling"
(see BOOSTRIX®, solicited local adverse events for definition) was low (0.9%). Following their sixth consecutive dose of
an acellular pertussis vaccine, persons reported more pain, less redness, and less swelling compared with their fifth dose
of pediatric DTaP(INFANRIX®) (127).
Two smaller Canadian postlicensure safety studies in
adolescents also showed acceptable safety when Tdap
(ADACEL™) was administered at intervals less than 5 years after tetanus and diphtheria toxoid--containing vaccines
(128,129). Taken together, these three Canadian studies support the safety of using Tdap after Td at intervals less than 5 years. The largest
study suggests intervals as short as approximately 2 years are acceptably safe
(126).
Simultaneous and Nonsimultaneous Vaccination with Tdap/Td and
Diphtheria-Containing Tetravalent Meningococcal Conjugate Vaccine
Tdap, Td, and tetravalent meningococcal conjugate vaccine ([MCV4]
Menactra®, sanofi pasteur, Swiftwater,
Pennsylvania) contain diphtheria toxoid
(32,33,130,131). Each of these vaccines is licensed for use in adolescents, but MCV4 is
not indicated for active immunization against diphtheria
(131). During 2005, MCV4 was recommended for routine use
among adolescents (130,132). In MCV4, the diphtheria toxoid (approximately 48
µg) serves as the carrier protein that
improves immune responses to meningococcal antigens. Precise comparisons cannot be made between the quantity of diphtheria
toxoid in the vaccines; however, the amount in a dose of MCV4 is estimated to be comparable with the average quantity in a dose
of pediatric DTaP (133).
No prelicensure studies of simultaneous or sequential vaccination with Tdap and MCV4 were done. None of the persons
in the Canadian safety studies described above had received MCV4. Persons who recently received one
diphtheria toxoid--containing vaccine might have increased rates of adverse reactions after a subsequent diphtheria
toxoid--containing vaccine when diphtheria antibody
titers remain elevated from the previous vaccination
(26,108,111,112). The diphtheria GMCs were comparable or lower following Tdap compared
with Td§§; therefore, results
of a co-administration trial of Td and MCV4 might be informative to infer the effect of co-administration of Tdap and MCV4. A randomized, controlled prelicensure
trial assessed the safety of simultaneous versus sequential administration of Td and MCV4.
In this co-administration trial, administration of Td
(approximately 8 µg of diphtheria toxoid) with MCV4 first,
then placebo 28 days later (simultaneous group), or administration of Td with placebo first, then MCV4 28 days later
(sequential group) was studied among 1,021 healthy adolescents aged 11--17 years
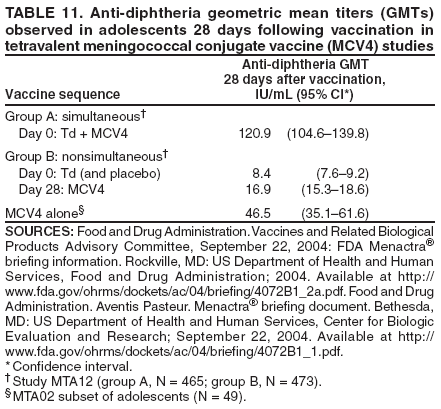
(Table 11) (89,131,133). Serum samples from a
subset of adolescents vaccinated with MCV4 from a different clinical trial were used for comparison.
Administration of MCV4 first followed by Td was not studied. Both simultaneous and sequential administration of Td and MCV4 induced
immune responses to all antigens. One month postvaccination, the immune responses to diphtheria toxoid were higher when
MCV4 was administered simultaneously with Td (GMT 120.9 IU/mL) than when Td was administered with placebo (GMT 8.4
IU/mL). Adolescents vaccinated with MCV4 alone also had high antidiphtheria responses 1 month following vaccination
(GMT 46.5 IU/mL) (Table 11) (89,131,133).
Adverse events on vaccination day and during the following 7 days were assessed among adolescents in the simultaneous
and sequential groups. The overall rates of solicited local reactions were similar for the two groups: 58.0% reported local
reactions at the MCV4 injection site in the simultaneous group versus 57.0% in the sequential group, and 74.7%
reported local reactions at the Td injection site in the simultaneous group versus 73.3% in the sequential group. Pain was the
most frequently reported reaction and pain rates were similar between groups; severe pain was uncommon (<1% of persons).
Fever >99.5° F (>37.5° C) and high fever
>104° F (>40° C) were reported in
<5% and <0.5% of persons, respectively
(133--135). The safety of simultaneous vaccination of MCV4 with Tdap and sequential administration of Tdap first followed by MCV4
1 month later has been inferred from results of this study.
When Tdap or Td is administered after MCV4, rates of
adverse reactions might be higher than when the dose
is administered before MCV4 because pre-existing diphtheria antibody levels might be
higher (26,108,111,112,133,135). Rates of adverse reactions were assessed in a small prelicensure study for MCV4 among 76 adolescents aged 15--17 years who received 2
doses of MCV4 spaced 3 years apart. After the second dose of MCV4, no SAEs, fever
>102.2° F (>39° C), or severe local reactions
were reported with the exception of one person, who
reported severe pain at the injection site that lasted for 1 day (sanofi
pasteur, unpublished data, 2005). No other available data exist on the safety of intervals between MCV4 and other diphtheria
toxoid--containing vaccines. Postlicensure studies to provide additional information are under way
(104,105).
Neurologic and Systemic Events Associated with Vaccines with
Pertussis Components or Tetanus Toxoid--Containing Vaccines
Vaccines with Pertussis Components
Concerns about the possible role of vaccines with pertussis components in causing neurologic reactions or
exacerbating underlying neurologic conditions are long-standing
(20,136). ACIP recommendations to defer pertussis vaccines in
infants with suspected or evolving neurologic disease, including seizures, have been based primarily on concerns that
neurologic events after vaccination (with whole cell preparations in particular) might interfere with the subsequent evaluation of
the infant's neurologic status (1,136).
In 1991, the Institute of Medicine (IOM) concluded that evidence favored acceptance of a causal relation between
pediatric DTP and acute encephalopathy; the IOM has not evaluated associations between pediatric DTaP and neurologic events
(123). Pediatric DTaP is contraindicated for children with a history of encephalopathy not attributable to another identifiable
cause occurring within 7 days after pediatric
DTP/DTaP vaccination. Though active surveillance in Canada during 1993--2002
failed to ascertain any acute encephalopathy cases causally related to whole cell or acellular pertussis vaccines among a
population administered 6.5 million doses of pertussis vaccines
(137), research conducted in Japan during the introduction of
acellular pertussis vaccines yielded rates of 1.0--1.3 attributable encephalopathy cases within 7 days of vaccination per 10 million
doses (138).
ACIP has recommended that infants with evolving neurologic conditions should not be vaccinated with pediatric
DTaP until a treatment regimen has been established and the condition has stabilized
(1). Concerns about vaccinating adolescents with progressive or uncontrolled underlying neurologic disease must be weighed against the potential for morbidity
from pertussis. Adolescents with severe neurologic conditions might be at risk for severe pertussis
(48; CDC, unpublished data, 2005). ACIP does not consider a history of
well-controlled seizures in the vaccinee or a family history of
seizures (febrile or afebrile) or other neurologic disorder to be a contraindication or precaution to vaccination with pertussis components
(1).
ACIP has recommended that vaccine providers and parents evaluate the risks for and benefits of administering
subsequent doses of vaccines with pertussis components to young children who experienced these events after pediatric
DTP/DTaP: temperature >105° F
(>40.5° C) within 48 hours after pediatric DTP/DTaP, not attributable to another cause; collapse
or shock-like state (hypotonic hyporesponsive episode) within 48 hours after pediatric DTP/DTaP; persistent crying lasting
>3 hours, occurring within 48 hours after pediatric DTP/DTaP; or convulsions with or without fever, occurring within 3
days after pediatric DTP/DTaP. All of these events were documented more frequently following whole cell pertussis vaccines
than they have been following acellular vaccines
(1,139--142). VAERS data have documented decreased reports of fever and
other systemic events in infants and children following pediatric DTaP in comparison with pediatric DTP
(143). These events either do not occur in adolescents or are of less clinical concern in this age group than in infants and children (e.g., febrile
seizures and hypotonic-hyporesponsive episodes). Taken together, this information supports administering Tdap to adolescents with
a history of the events listed above after pediatric DTaP/DTP.
Tetanus Toxoid--Containing Vaccines
ACIP has recommended that Guillain-Barré syndrome
occurring <6 weeks after receipt of a tetanus toxoid--containing
vaccine is a precaution for subsequent tetanus
toxoid--containing vaccines (91). IOM concluded that evidence favored acceptance of
a causal relation between tetanus toxoid--containing vaccines and Guillain-Barré syndrome
(123). Evidence is based primarily on a
well-documented case report (123,144). However, a subsequent analysis of active surveillance data in both adult and
pediatric populations failed to demonstrate an association between
receipt of a tetanus toxoid--containing vaccine and onset of
Guillain-Barré syndrome within 6 weeks following vaccination
(145).
IOM also has concluded that evidence from case reports and uncontrolled studies involving tetanus
toxoid--containing vaccines favored a causal relation between tetanus
toxoid--containing vaccines and brachial neuritis.
Brachial neuritis is considered to be a compensable event through the Vaccine Injury Compensation Program
(123). However, ACIP does not consider a history of brachial neuritis to be a precaution or contraindication for administration of tetanus
toxoid--containing vaccines; brachial neuritis is usually self-limited
(91,143,146).
Considerations for Vaccinating Pregnant Adolescents with Td or Tdap
ACIP has recommended Td routinely for pregnant women who received the last tetanus toxoid--containing vaccine
>10 years earlier. This recommendation is primarily to prevent neonatal tetanus
(24,31). In women adequately vaccinated
against tetanus, passive transfer of antibodies across the placenta during pregnancy protects their newborns from neonatal
tetanus (147--149). During 1999, a global maternal and neonatal tetanus elimination goal was recommended by the WHO,
the United Nations Children's Fund, and the United Nations Population Fund
(150).
As with tetanus, antibodies to pertussis antigens are passively transferred during pregnancy
(151,152); however, serologic correlates of protection against pertussis are not known
(88). Whether or not passive transfer of maternal antibodies
to pertussis antigens protects neonates against pertussis is also unclear
(88,153).
All licensed Td and Tdap vaccines are categorized as Pregnancy Category C agents by
FDA.¶¶ Pregnant women were excluded from prelicensure trials, and no animal reproduction studies have been conducted for Td or Tdap
(32,33,98--101). Td has been used extensively in pregnant women worldwide, and no evidence indicates use of tetanus and diphtheria
toxoids administered during pregnancy are teratogenic
(24,154,155).
Summary of the Rationale for Adolescent Tdap Recommendations
The availability of Tdap, the first pertussis vaccines formulated for use in adolescents and adults in the United States,
offers a new opportunity to reduce the burden of pertussis in this country. The primary objective of vaccinating adolescents
with Tdap is to protect the vaccinated adolescent against pertussis while maintaining the standard of care for protection
against tetanus and diphtheria. A secondary objective of adolescent Tdap vaccination is to reduce the reservoir of pertussis within
the U.S. population at large and potentially reduce the incidence of pertussis in other age groups, including infants who have
the highest risk for complications from pertussis
(16,48). The extent to which the secondary objective can be achieved
through adolescent vaccination is unknown.
The decision to recommend routine Tdap vaccination for adolescents is based on evidence regarding the burden of
pertussis among adolescents; negative effects of pertussis outbreaks involving adolescents on the community and the public
health system; studies suggesting use of Tdap among adolescents will likely be safe, effective, and economical; and the
established infrastructure for adolescent vaccination
(30,32,33,52--54,68).
To protect against pertussis, Tdap will be introduced into an adolescent vaccination schedule that already includes two
other tetanus and/or diphtheria toxoid--containing vaccines, Td, and MCV4
(23,130). Frequent doses of tetanus and
diphtheria toxoid--containing vaccines can be associated with
increased local and systemic reactogenicity
(108,109). ACIP has considered issues related to spacing and administration sequence of these three vaccines to develop recommendations for Tdap use
in adolescents.
Recommendations for Use of Tdap and Td Among Adolescents
The following sections present recommendations for use of Tdap and Td among adolescents aged 11--18 years
and include routine Tdap vaccination, contraindications and precautions, and special situations (Appendix C).
1) Adolescents aged 11--18 years should receive a single dose of Tdap instead of Td for booster
immunization against tetanus, diphtheria, and pertussis if they have completed the recommended childhood
DTP/DTaP vaccination series*** and have not received Td or Tdap. The preferred age for Tdap vaccination is 11--12
years; routinely administering Tdap to young adolescents will reduce the morbidity associated with pertussis
in adolescents.
2) Adolescents aged 11--18 years who received Td, but not Tdap, are encouraged to receive a single dose of Tdap
to provide protection against pertussis if they have completed the recommended childhood DTP/DTaP
vaccination series.*** An interval of at least 5 years between Td and Tdap is encouraged to reduce the risk for local
and
systemic reactions after Tdap vaccination. However, an interval less than 5 years between Td and Tdap can
be used. The benefit of using Tdap at a shorter interval to protect against pertussis generally
outweighs the risk for local and systemic reactions
after vaccination in settings with increased risk for pertussis or its complications
(See Pertussis Outbreaks and Other Settings with Increased Risk for Pertussis or its Complications [section 3-C]).
3) Vaccine providers should administer Tdap and tetravalent meningococcal conjugate vaccine
([MCV4] Menactra®) (which both contain diphtheria toxoid) to adolescents aged 11--18 years during the same visit if
both vaccines are indicated and available
(130,132).
1-B. Dosage and Administration
The dose of Tdap is 0.5 mL, administered intramuscularly (IM), preferably into the deltoid muscle.
1-C. Simultaneous Vaccination with Tdap and Other Vaccines
If two or more vaccines are indicated, they should be administered during the same visit (i.e.,
simultaneous vaccination). Each vaccine should be administered using a separate syringe at a different anatomic site. Some
experts recommend administering no more than two injections per muscle, separated by at least one inch.
Administering all indicated vaccines during a single visit increases the likelihood that adolescents will receive
each of the vaccines on schedule (91). Vaccine providers should administer MCV4 and Tdap (or Td) during the same
visit if both vaccines are indicated and
available.MCV4 contains diphtheria toxoid as a carrier protein
(131) (see Safety Considerations for Adolescent Vaccination with Tdap or Td).
1-D. Interchangeable Use of Tdap Vaccines
A single dose of either Tdap product
(BOOSTRIX® or
ADACEL™) can be administered to adolescents regardless
of the type or manufacturer of pediatric DTP/DTaP used for childhood vaccination.
1-E. Preventing Adverse Events
Syncope can occur after vaccination, might be more common among adolescents and young adults than
among other age groups, and has rarely resulted in serious injury
(91,156,157). Certain experts suggest a 15--20
minute observation period following vaccination
(91,158). If syncope occurs, patients should be observed until
symptoms resolve.
The potential for administration errors involving tetanus toxoid--containing vaccines and other products is
well documented (159--161). For example, Td and TT have been inadvertently administered instead of
tuberculin purified protein derivative (PPD)
(159). Attention to proper vaccination technique, including use of an
appropriate needle length andstandard routes of administration (i.e., IM for Tdap) might minimize the risk for adverse
events (91). Adverse events associated with inadvertent vaccine administration can be reported to the Vaccine Adverse
Event Reporting System (VAERS) (see Reporting of Adverse Events after Vaccination).
1-F. Record Keeping
Health-care providers who administer vaccines are required to keep permanent vaccination records of
vaccines covered under the National Childhood Vaccine Injury Act in the vaccinee's medical record; ACIP has
recommended that this practice include all vaccines
(91). Because documentation of tetanus toxoid--containing
vaccine administration is frequently required for school or camp entry and as part of wound management,
encouraging adolescents to maintain a personal vaccination record is important to minimize administration of
unnecessary vaccinations. Vaccine providers can record the type of the vaccine, manufacturer, anatomic site, route, and date
of administration and name of the administering facility on the personal record.
2. Contraindications and Precautions for Use of Tdap and Td Among
Adolescents Aged 11--18 Years
2-A. Contraindications
Tdap or Td is contraindicated for persons with a history of serious allergic reaction (i.e., anaphylaxis) to
any component of the vaccine. Because of the importance of tetanus vaccination, persons with a history of
anaphylaxis to components included in all Tdap and Td vaccines should be referred to an allergist to determine whether
they have a specific allergy to tetanus toxoid, can be desensitized to tetanus toxoid, and can safely
receive TT vaccinations.
Tdap is contraindicated for adolescents with a history of encephalopathy (e.g., coma or prolonged seizures)
not attributable to an identifiable cause within 7 days of administration of a vaccine with pertussis components.
This contraindication is for the pertussis components and these persons should receive Td instead of Tdap.
2-B. Precautions and Reasons to Defer Tdap and/or Td
A precaution is a condition in a vaccine recipient that might increase the risk for a serious reaction
(91). The following are precautions for Tdap and/or Td. In these situations, vaccine providers should evaluate the risks for
and benefits of administering Tdap or Td.
Guillain-Barré syndrome <6 weeks after a previous dose of a tetanus toxoid--containing vaccine. If a decision is
made to continue vaccination with tetanus toxoid, Tdap is preferred to Td if otherwise indicated.
Progressive neurologic disorder, including progressive encephalopathy, or uncontrolled epilepsy,
until the condition has stabilized. These precautions are for pertussis
components.††† If a decision is made to provide
protection against pertussis, Tdap is preferred if otherwise indicated. If a decision is made to withhold pertussis
vaccination, Td can be used instead of Tdap.
Tdap or Td vaccination should generally be deferred during the following situations.
Moderate or severe acute illness with or without fever. Defer Tdap or Td vaccination until the acute illness resolves.
History of an Arthus reaction following a previous dose of a tetanus toxoid--containing and/or diphtheria
toxoid--containing vaccine, including MCV4 (see Safety Considerations for Adolescent Vaccination with Tdap or
Td section for a description of an Arthus reaction). Vaccine providers should carefully review the medical history
to verify the diagnosis of an Arthus reaction, and can consult with an allergist or immunologist. If an Arthus
reaction was likely, vaccine providers should consider deferring Tdap or Td vaccination until at least 10 years have
elapsed since the last tetanus toxoid--containing and/or diphtheria
toxoid--containing vaccine was received. If the
Arthus reaction was associated with a vaccine that contained diphtheria toxoid without tetanus toxoid (e.g.,
MCV4), deferring Tdap or Td might leave the adolescent inadequately protected against tetanus. In this situation, if the
last tetanus toxoid--containing vaccine was >10 years earlier, vaccine providers can obtain a serum antitetanus level
to evaluate the need for tetanus vaccination (antitetanus levels >0.1 IU/mL are considered protective) or
administer TT.
2-C. Not Contraindications or Precautions
The following conditions are not contraindications or precautions for Tdap or Td, and adolescents with
these conditions can receive a dose of Tdap or Td if otherwise indicated. The conditions in italics are precautions
for pediatric DTP/DTaP but are not contraindications or precautions for Tdap vaccination in adolescents
(1).
Temperature >105° F
(>40.5° C) within 48 hours after pediatric DTP/DTaP not attributable to
another cause;
Collapse or shock-like state (hypotonic hyporesponsive episode) within 48 hours after pediatric DTP/DTaP;
Persistent crying lasting >3 hours, occurring within 48 hours after pediatric DTP/DTaP;
Convulsions with or without fever, occurring within 3 days after pediatric DTP/DTaP;
History of an extensive limb swelling reaction following pediatric DTP/DTaP or Td that was not an Arthus
reaction (see Safety Considerations for Adolescent Vaccination with Tdap or Td section for descriptions of ELS and
Arthus reactions);
Stable neurologic disorder including well-controlled
seizures, a history of seizure disorder that has resolved,
and cerebral palsy;
Brachial neuritis;
Latex allergies other than anaphylactic allergies (e.g., a history of contact allergy to latex gloves)
(162). The tip and rubber plunger of the
BOOSTRIX® needleless syringe contain latex. The
BOOSTRIX® single dose vial and
ADACEL™preparations contain no latex. Some Td products contain latex (consult package inserts for details);
Breastfeeding;
Immunosuppression, including persons with human
immunodeficiency virus (HIV). The immunogenicity of Tdap
in persons with immunosuppression has not been studied and could be
suboptimal;
Intercurrent minor illness; and
Use of antimicrobials.
3. Special Situations for Use of Tdap and Td
3-A. General Principles
This section addresses special situations for Tdap and Td use. As with the routine situations, only a single dose of
Tdap should be administered to an adolescent aged 11--18 years. For most, but not all, of the special situations, Tdap is
preferred to Td. In some special situations or when contraindications or precautions are present, Td rather than Tdap might
be indicated. The dose of Td is 0.5 mL, administered IM.
Tdap (or Td) and MCV4 should be administered at the same visit during special situations if both vaccines
are indicated and available, although this might not always be feasible (e.g., wound management).
Simultaneous administration of Tdap (or Td) and MCV4 and an interval of at least 5 years between Td and Tdap can reduce
the risk for local and systemic reactions. In certain special situations listed below, the benefit of protection against
disease probably outweighs this risk.
3-B. Nonsimultaneous Vaccination with Tdap and Other Vaccines, Including MCV4
ACIP has recommended that inactivated vaccines can be administered at any time before or after a
different inactivated or live vaccine (i.e., nonsimultaneous vaccination), unless a contraindication exists
(91). Simultaneous administration of Tdap (or Td) and MCV4 (which all contain diphtheria toxoid) during the same visit is
preferred when both Tdap (or Td) and MCV4 are indicated. If simultaneous vaccination is not feasible (e.g., a vaccine is
not available), MCV4 and Tdap (or Td) can be administered
using any sequence. Persons who recently received
one diphtheria toxoid--containing vaccine might have increased rates of adverse reactions after a subsequent
diphtheria toxoid--containing vaccine when diphtheria antibody titers remain elevated from the previous
vaccination (26,108,111,112) (see Safety Considerations for Adolescent Vaccination with Tdap or Td section for a discussion
of nonsimultaneous vaccination).
3-C. Pertussis Outbreaks and Other Settings with
Increased Risk for Pertussis or its Complications
Vaccine providers can administer Tdap to adolescents aged 11--18 years at an interval less than 5 years after
Td, particularly when the benefit of providing protection against pertussis is likely to be increased. The safety of
an interval as short as approximately 2 years between Td and Tdap is supported by a
Canadian study among children and adolescents (see Spacing and Sequence Administration of Vaccines Containing Tetanus Toxoid,
Diphtheria Toxoid, and Pertussis Antigens)
(126).
The benefit of using Tdap at an interval less than 5 years after Td is likely to be increased among adolescents
when the adolescent is at increased risk for acquiring pertussis (e.g., during outbreaks or periods of increased
pertussis activity in the community). Postexposure chemoprophylaxis and other pertussis control guidelines are
described elsewhere (64,158,163). The benefit of using a shorter interval also might be increased for adolescents
with severe underlying medical conditions (e.g., chronic pulmonary disease or neurologic disorders) because
these adolescents might be at increased risk for
pertussis-related complications.
Infants aged <12 months are at highest risk for pertussis-related complications and hospitalizations compared
with older age groups; young infants have the highest risk for death from pertussis. Administering Tdap at an interval
less than 5 years after Td to an adolescent who has or anticipates having close contact with an infant aged <12
months might reduce the risk for transmitting pertussis to the
infant. Infants should be vaccinated on time with
pediatric DTaP (1,23).
3-D. Lack of Availability of Tdap or MCV4
If Tdap and MCV4 are both indicated but only one vaccine is available, the available vaccine generally should
be administered. When Tdap is indicated but not available, vaccine providers should administer Td or temporarily
defer Tdap/Td vaccination. Td should be administered to provide protection against tetanus and diphtheria if
the adolescent received the last pediatric DTP/DTaP/DT or Td >10 years earlier. Recommendations for use of
Tdap among adolescents who already received Td would apply to these adolescents when Tdap becomes available
(see Routine Tdap Vaccination [section 1-A]). Tdap/Td vaccination can be deferred temporarily if the
adolescent completed the childhood DTP/DTaP vaccination series***, received the last pediatric DTP/DTaP/DT or Td
<10 years earlier, and is likely to return for follow-up. If the vaccine provider defers Td in order to administer Tdap
when it becomes available, a system to recall the adolescent should be maintained. The adolescent also can be referred
to another facility for Tdap administration.
3-E. Tetanus Prophylaxis in Wound Management
ACIP has recommended administering tetanus toxoid--containing vaccine and tetanus immune globulin (TIG)
as part of standard wound management to prevent tetanus
(Table 13) (24). Tdap is preferred to Td for adolescents
aged 11--18 years who were vaccinated against tetanus >5 years earlier, require a tetanus toxoid--containing vaccine as
part of wound management, and have not previously received Tdap. Adolescents who have completed the 3-dose
primary tetanus vaccination series and have received a tetanus toxoid--containing vaccine <5 years earlier are protected
against tetanus and do not require a tetanus toxoid--containing vaccine as part of wound management. Although
MCV4 and Tdap (or Td) should be administered at the same visit during routine situations if both vaccines are indicated,
this might not be feasible for wound management.
A thorough attempt must be made to determine whether an adolescent has completed the 3-dose primary
tetanus vaccination series. Persons with unknown or uncertain tetanus vaccination histories should be considered to have
had no previous doses of a tetanus toxoid--containing vaccine (see Adolescents with History of Incomplete
Pediatric DTP/DTaP/DT or Td Vaccination [section 3-H]). Persons who have not completed the primary series might
require a tetanus toxoid--containing vaccine and passive immunization with TIG at the time of wound management
(Table 13). When both TIG and a tetanus toxoid--containing vaccine are indicated, each product should be
administered using a separate syringe at different anatomic sites
(24).
Adolescents with a history of an Arthus reaction after a previous dose of a tetanus toxoid--containing
vaccine should not receive a tetanus toxoid--containing
vaccine until >10 years after the most recent dose, even if they have
a wound that is neither clean nor minor (Table 13). If the Arthus reaction was associated with a vaccine that
contained diphtheria toxoid without tetanus toxoid (e.g., MCV4), deferring Tdap or Td might leave the
adolescent inadequately protected against tetanus and
TT should be administered. In all circumstances, the decision
to administer TIG is based on the primary vaccination history for tetanus
(Table 13).
3-F. History of Pertussis
Adolescents aged 11--18 years who have a history of pertussis generally should receive Tdap according to the
routine recommendations. This practice is preferred because duration of protection induced by pertussis is
unknown (waning immunity might begin as early as 7 years after infection) and because the diagnosis of pertussis can
be difficult to confirm, particularly with test results other than positive culture for
B. pertussis (164). Administering pertussis vaccines to persons with a history of pertussis presents no theoretical safety concern.
3-G. Adolescents with History of Incomplete Pertussis Vaccination (Received Pediatric DT or Td
Instead of Pediatric DTP/DTaP)
Adolescents who received pediatric DT or Td vaccination instead of one or more doses of pediatric DTP/DTaP
in the series during childhood should generally receive a single dose of Tdap to provide protection against pertussis
if they completed the recommended childhood vaccination series for tetanus and
diphtheria§§§ and have
no contraindications to the pertussis components. In routine situations, an interval of at least 5 years between Td
and Tdap is encouraged (see Routine Tdap Vaccination [section 1-A]).
3-H. Adolescents with History of Incomplete Pediatric DTP/DTaP/DT or Td Vaccination
Adolescents aged 11--18 years who have never been vaccinated against tetanus, diphtheria, or pertussis (no doses
of pediatric DTP/DTaP/DT or Td) shouldreceive a series of three tetanus and diphtheria
toxoid--containing vaccinations. The preferred schedule is a single Tdap dose, followed by a dose of Td
>4 weeks after the Tdap dose, and a second dose of Td 6--12 months after the earlier Td dose. Tdap can be substituted for any one of the three
Td doses in the series.
Adolescents who received other incomplete vaccination schedules for tetanus and diphtheria should be
vaccinated with Tdap and/or Td according to guidance for catch-up vaccination (Appendix D). A single dose of Tdap can
be used to substitute for any one of the Td doses in the series.
In situations in which the adolescent probably has received vaccination against tetanus and diphtheria but
cannot produce records, vaccine providers can obtain serologic testing for antibodies to tetanus and diphtheria to
avoid unnecessary vaccination. If antitetanus and antidiphtheria levels are each
>0.1 IU/mL, previous vaccination with tetanus and diphtheria
toxoid--containing vaccines is likely and a single dose of Tdap is indicated; this Tdap
dose counts as the adolescent booster dose.
3-I. Children Aged 7--10 Years with Incomplete Pediatric DTP/DTaP Vaccination History
Neither Tdap vaccine is licensed for use in children aged <10 years
(32,33). Children aged 7--10 years who
never received a pediatric DTP/DTaP/DT dose or a Td dose generally should receive 3
doses of Td¶¶¶: dose 2
is administered >4 weeks after dose 1 and dose 3 is administered 6--12 months after dose 2. Children aged 7--10
years who received other incomplete vaccination schedules against tetanus, diphtheria, and pertussis should be
vaccinated according to catch-up guidance (Appendix E). When these children become adolescents (aged 11--18 years),
they should receive Tdap according to the routine recommendations and interval guidance used for adolescents
who completed the childhood DTP/DTaP series (see Routine Tdap Vaccination [section 1-A]).
In situations in which the child probably has received
vaccination against tetanus and diphtheria but
cannot produce records, vaccine providers can obtain serologic testing for antibodies to tetanus and diphtheria to
avoid unnecessary vaccination. If antitetanus and antidiphtheria levels are each
>0.1 IU/mL, previous vaccination with tetanus and diphtheria toxoid--containing vaccines is likely. In this situation, Td vaccination can be deferred
until the child is aged 11--12 years and eligible to receive Tdap.
3-J. Inadvertent Administration of Tdap or Pediatric DTaP
To help prevent inadvertent administration of Tdap when pediatric DTaP is indicated or pediatric DTaP when
Tdap is indicated, vaccine providers should review product labels before administering these vaccines; the packaging
might appear similar. Tdap is not indicated for children aged <10 years. Tdap contains lower amounts of diphtheria
toxoid and lower amounts of some pertussis antigens compared with pediatric DTaP. Studies of the immune responses
to Tdap among infants have not been conducted. Pediatric
DTaP is not indicated for persons aged >7 years;
the increased diphtheria toxoid content is associated
with higher rates of adverse reactions in older persons
(24--28).
Guidance on the best approach to vaccination following inadvertent administration of Tdap or pediatric DTaP
is based primarily on expert opinion. The family should be informed of any inadvertent vaccine
administration. Adverse events associated with inadvertent vaccine administration can be reported to VAERS (see Reporting
of Adverse Events after Vaccination). If Tdap is inadvertently administered instead of pediatric DTaP to a child aged
<7 years as any one of the first three doses of the
tetanus-diphtheria-pertussis vaccination series, the Tdap dose
should not be counted as valid, and a replacement dose of pediatric DTaP should be administered. If the
inadvertent administration is discovered while the child is in the office, the pediatric DTaP can be administered during the
same visit. If the child has left the office, some experts suggest administering the replacement dose of pediatric
DTaP within approximately 72 hours, or administering it 4 weeks later to optimize the child's immune response to
the antigens in pediatric DTaP. This practice helps
ensure that the child stays on the primary series schedule and
has adequate protection against diphtheria and pertussis. However, the replacement dose of pediatric DTaP can
be administered as soon as feasible at any interval after the inadvertent Tdap dose. The remaining doses of the
pediatric DTaP series should be administered on the routine schedule, with at least a 4 week interval between
the replacement dose of pediatric DTaP and the next dose of pediatric DTaP. For example, if an 8-week-old
infant inadvertently received a dose of Tdap instead
of the first dose of pediatric DTaP and does not receive a
replacement dose of pediatric DTaP within about 72 hours, a replacement dose of pediatric DTaP can be administered 4
weeks after the inadvertent Tdap dose (age 12 weeks). The routine schedule of pediatric DTaP can then be
resumed 4 weeks after the pediatric DTaP replacement dose (age 16 weeks) with the other recommended vaccines
(1,23).
If Tdap is inadvertently administered as the fourth or the fifth dose in the tetanus-diphtheria-pertussis
vaccination series to a child aged <7 years, the Tdap dose should be counted as valid and does not need to be repeated; the
child who received Tdap as a fourth dose should complete the pediatric DTaP schedule
(23). The routine adolescent Tdap vaccination recommendations would apply when this child becomes an adolescent. For example, a child
who inadvertently receives Tdap at age 5 years instead
of the fifth dose of pediatric DTaP should receive a second dose
of Tdap at age 11--12 years.
If Tdap or pediatric DTaP is inadvertently administered
to a child aged 7-9 years instead of Td as part of
catch-up vaccination or for wound management, this dose can be counted as the adolescent Tdap dose, or the child can
later receive an adolescent booster dose of Tdap according to the interval guidance used for Td to Tdap (see Routine
Tdap Vaccination [section 1-A] and Pertussis Outbreaks and Other Settings with Increased Risk for Pertussis or
its Complications [section 3-C]). In either case, the child should receive a dose of vaccine containing tetanus
and
diphtheria toxoids no longer than 10 years after the inadvertent Tdap or pediatric DTaP dose or according to
the guidance for catch-up vaccination (Appendix E).
If pediatric DTaP is inadvertently administered to an adolescent aged
11--18 years, the dose should be counted as the adolescent Tdap booster. The adolescent should receive the next dose of a vaccine containing tetanus and
diphtheria toxoids 10 years after the inadvertent pediatric DTaP dose or according to the guidance for catch-up
vaccination (Appendix D).
3-K. Vaccination during Pregnancy
As with other inactivated vaccines and toxoids
(91,165), pregnancy is not considered a contraindication for
Tdap vaccination. Guidance on the use of Tdap during pregnancy to protect against pertussis is under consideration
by ACIP. Pregnant adolescents who received the last tetanus toxoid--containing vaccine <10 years previously
should generally receive Tdap after delivery, if otherwise indicated (see Post-Partum Vaccination [section 3-L]).
To prevent neonatal tetanus, pregnant adolescents who received the last tetanus toxoid--containing vaccine
>10 years previously should generally receive Td in preference to Tdap. ACIP has recommended that pregnant women receive
Td if the last tetanus toxoid--containing vaccine was administered >10 years previously
(24,31,91,165). If Td is indicated, vaccinating during the second or third trimester is preferred when feasible to minimize a perception of an association
of vaccine with adverse pregnancy outcomes, which are more common during the first trimester. A pregnant
adolescent who has not received the 3-dose primary
tetanus vaccination series should begin this series during pregnancy, using
Td. (see Adolescents with History of Incomplete Pediatric DTP/DTaP/DT or Td Vaccination [section 3-H]).
Because of lack of data on the use of Tdap in pregnant women, both Tdap manufacturers have established
pregnancy registries. Health-care providers are encouraged to report Tdap vaccination during pregnancy to the following
registries: BOOSTRIX® to GlaxoSmithKline Biologicals at 1-888-825-5249 and
ADACEL™ to sanofi pasteur at
1-800-822-2463 (1-800-VACCINE) (32,33).
3-L. Post-Partum Vaccination
Adolescents aged 11--18 years, including those who are breastfeeding, should receive a single dose of Tdap as soon
as feasible in the postpartum period, according to the routine Tdap recommendations and
interval guidance (see Routine Tdap Vaccination [section 1-A] and Pertussis Outbreaks and Other Settings with Increased Risk
for Pertussis or its Complications [section 3-C]). For adolescent mothers who have not already received
Tdap, vaccinating the mother with Tdap during the postpartum period might reduce the risk for pertussis transmission to
the infant. Protection of the mother against pertussis requires an estimated 1 to 2 weeks after vaccination.
3-M. Older Adolescents and Adults Aged >18 Years
To maintain protection against tetanus and diphtheria, ACIP has recommended decennial Td boosters for
adults beginning 10 years after the adolescent dose
(24,30). The safety and efficacy of Tdap
(ADACEL™ ) as a single dose booster immunization against tetanus, diphtheria, and pertussis has been demonstrated for persons aged 19--64
years (32). In October 2005, ACIP recommended a single dose of Tdap
(ADACEL™)for adults aged 19--64 years
who have not received Tdap; recommendations for the use of Tdap among adults will be published
separately.****
Reporting of Adverse Events After Vaccination
As with any newly licensed vaccine, surveillance for rare adverse events associated with administration of Tdap
is important for assessing its safety in large-scale use. The
National Childhood Vaccine Injury Act of 1986 requires
health-care providers to report specific adverse events that follow tetanus, diphtheria, or pertussis vaccination (http://vaers.hhs.gov/reportable.htm). All clinically significant adverse events should be reported to VAERS, even if causal relation to vaccination
is not certain. VAERS reporting forms and information are available electronically at
http://www.vaers.hhs.gov/ or by
telephone, (800) 822-7967. Web-based reporting is available and providers are encouraged to report electronically at
https://secure.vaers.org/VaersDataEntryintro.htm to promote better timeliness and quality of safety data.
Safety surveillance for adolescent Tdap, MCV4, and other vaccines is being conducted on an ongoing basis in
cooperation with FDA. Previously published safety data for Td and for tetravalent meningococcal polyscaccharide vaccine will
provide some of the basis for comparison with postlicensure safety surveillance for Tdap and MCV4, respectively
(130,166).
Vaccine Injury Compensation
The National Vaccine Injury Compensation Program (VICP), established by the National Childhood Vaccine
Injury Act of 1986, is a system under which compensation can be paid on behalf of a person thought to have been
injured or to have died as a result of receiving a vaccine covered by the program. Anyone receiving a covered vaccine,
regardless of age, can file a petition under VICP. The program is intended as an alternative to civil litigation under the traditional tort system because
negligence need not be proven.
The Act establishes 1) a Vaccine Injury Table that lists the vaccines covered by the program; 2) the injuries, disabilities,
and conditions (including death) for which compensation might be paid without proof of causation; and 3) the period
after vaccination during which the first symptom or substantial aggravation of the injury must appear. Persons might
be compensated for an injury listed in the table or one that can be demonstrated to result from administration of a listed
vaccine. All tetanus toxoid--containing vaccines and vaccines with pertussis components (e.g., Tdap, Td, and pediatric DTaP)
are covered under the Act. Additional information about the program is available at
http://www.hrsa.gov/osp/vicp or by calling
1-800-338-2382.
Areas for Future Research Related to Tdap and Adolescents
With recent licensure and introduction of Tdap for adolescents, close monitoring of pertussis disease trends and
vaccine safety will be high priorities for public health organizations and health-care providers. Active surveillance sites
in Massachusetts and Minnesota, supported by CDC, are being established to provide additional data on the burden of
pertussis in adolescents and other age groups and the impact of adolescent Tdap vaccination recommendations. Postlicensure studies
and surveillance activities are planned or under way to
evaluate
changes in the incidence of pertussis;
physicians' uptake of Tdap;
safety and immunogenicity of simultaneous and nonsimultaneous administration of Tdap and MCV4 in
adolescents (104,105); and
the prevalence of and risk factors for ELS in adolescents, including studies of adolescents who were vaccinated with 5
doses of pediatric DTaP series (during 2008, the first birth cohort for which an all-pediatric DTaP 5-dose schedule
was recommended will turn 11 years of age and become
eligible for adolescent vaccination with Tdap).
Research is needed to evaluate and define
immunologic correlates of protection for pertussis;
improved diagnostic tests for pertussis;
methods to enhance coverage and delivery of Tdap to adolescents; and
safety and effectiveness of repeated Tdap doses.
Acknowledgements
This report was prepared in collaboration with the Advisory Committee on Immunization Practices Pertussis Working Group.
We acknowledge our U.S. Food and Drug Administration colleagues, Theresa Finn, PhD, and Ann T. Schwartz, MD, for their review of
the Tdap product information and our Massachusetts Department of Public Health colleagues, Susan M. Lett, MD, Arquimedes
Areche, MPH, Nancy Harrington, Kirsten Buckley, MPH, Jill Northrup, MPH, Linda Han, MD, Dara Spatz Friedman, PhD, and
Stephanie Schauer, PhD, for providing data from Massachusetts used in this report. We also acknowledge the contributions of the
following consultants who provided technical expertise used in the report: William L. Atkinson, MD, Jeffery
P. Davis, MD, Michael D. Decker, MD, Leonard R. Friedland, MD, Daniel B. Fishbein, MD, Scott A. Halperin, MD, Kashif Iqbal, MPH, Tanya Johnson, MPH, Grace
M. Lee, MD, Lucia Lee, MD, Monika Naus, MD, Ismael R. Oretga-Sanchez, PhD, Larry
K. Pickering, MD, Renee Renfus, MD, Nancy Rosenstein, MD, Joel Ward, MD, and Donna Weaver, MN. We also recognize the contributions of many other consultants
from academia, state health departments, federal agencies, and industry who are not listed individually in this document.
* Incidence throughout this report was calculated using confirmed and probable cases reported to the NNDSS and population estimates from U.S.
Census Bureau, available at http://www.census.gov.
† Booster response: In persons with prevaccination antibody concentration <0.1 IU/mL, postvaccination antibody concentration
>0.4 IU/mL. In persons with prevaccination antibody concentration
>0.1 IU/mL, an increase of at least four times the prevaccination antibody concentration.
§ Booster responses: In initially seronegative persons (<5 EU/mL [ELISA units per milliliter], postvaccination antibody concentrations
>20 EU/mL. In initially seropositive persons with prevaccination antibody concentrations
>5 EU/mL and <20 EU/mL, an increase of at least four times the prevaccination
antibody concentration. In initially seropositive persons with a prevaccination antibody concentration of
>20 EU/mL, an increase at least two times the
prevaccination antibody concentration.
¶ Booster response was defined as a fourfold rise in antibody concentration, if the prevaccination antibody concentration was equal to or below the cut-off
value, and a two-fold rise in antibody concentration if the prevaccination antibody concentration was above the cut-off value. The cut-off value for tetanus was
2.7 IU/mL. The cut-off value for diphtheria was 2.56 IU/mL.
** A booster response for each antigen was defined as a fourfold rise in antibody concentration, if the prevaccination antibody concentration was
equal to or below the cut-off value, and a twofold rise in antibody concentration if the prevaccination antibody concentration was above the cut-off value. The
cut-off values for pertussis antigens were 85 EU/mL for pertussis toxin, 170 EU/mL for filamentous haemagglutinin, 115 EU/mL for pertactin, and 285
EU/mL for fimbriae.
†† An antihepatitis B surface antigen level
>10 mIU/mL was considered seroprotective.
§§ One month after vaccination, the antidiphtheria GMCs were
ADACEL™ 8.5 IU/mL (95% confidence interval [CI] =7.6--9.5) compared with
Tdsp 7.1 IU/mL (95% CI = 6.4--7.8) and
BOOSTRIX® 7.4 IU/mL (95% CI = 7.1--7.6) compared with
TdMPHBL14.0 IU/mL (95% CI = 13.2--14.9);
the antidiphtheria seroprotective and booster response rates in the adolescents vaccinated with Tdap
(ADACEL™ and
BOOSTRIX®) were noninferior to the those vaccinated with Td (see sections on Immunogenicity and Serologic Bridge to Pertussis Efficacy).
¶¶ U.S. Food and Drug Administration Pregnancy Category C: Animal studies have documented an adverse effect and no adequate and
well-controlled studies in pregnant women have been conducted or no animal studies and no adequate and well-controlled studies in pregnant women have been conducted
*** Five doses of pediatric DTP/DTaP before the seventh birthday; if the fourth dose was administered on or after the fourth birthday, the fifth dose
is not needed.
††† These conditions are precautions for use of Tdap among adolescents but are contraindications for use of pediatric DTaP among infants and children.
§§§ Five doses of pediatric DTP/DTaP/DT before the seventh birthday; if the fourth dose was administered on or after the fourth birthday, the fifth
dose is not needed. Children who began the tetanus and diphtheria vaccination series at age
>7 years required 3 doses of Td to complete the primary series.
¶¶¶ A single dose of
BOOSTRIX® Tdap is licensed for persons aged 10 years and can be used instead of Td for one of the doses in children aged 10
years; if BOOSTRIX® is administered early to a child aged 10 years, the dose counts as the adolescent Tdap dose usually administered at age 11--12 years.
Jenkinson D. Duration of effectiveness of pertussis vaccine: evidence from a 10 year community study. BMJ 1988;296:612--4.
Lambert H. Epidemiology of a small pertussis outbreak in Kent County, Michigan. Public Health Rep 1965;80:365--9.
Liese JG, Stojanov S, Peters A, et al. Duration of efficacy after primary immunization with Biken Acellular Pertussis Vaccine [Abstract G-2050].
In: Programs and Abstracts of the 43rd Interscience Conference on Antimicrobial Agents and Chemotherapy, Chicago, IL, September 14--17, 2003.
Olin P, Gustafsson L, Barreto L, et al. Declining pertussis incidence in Sweden following the introduction of acellular pertussis vaccine.
Vaccine 2003;21:2015--21.
Salmaso S, Mastrantonio P, Tozzi AE, et al. Sustained efficacy during the first 6 years of life of 3-component acellular pertussis
vaccines administered in infancy: the Italian experience. Pediatrics 2001;108:E81.
Tan T, Trindade E, Skowronski D. Epidemiology of pertussis. Pediatr Infect Dis J 2005;24:S10--S18.
CDC. Annual summary 1979: reported morbidity and mortality in the United States. MMWR 1980;28(54):12--7.
Farizo KM, Cochi SL, Zell ER, Brink EW, Wassilak SG, Patriarca PA. Epidemiological features of pertussis in the United States, 1980--1989.
Clin Infect Dis 1992;14:708--19.
Guris D, Strebel PM, Bardenheier B, et al. Changing epidemiology of pertussis in the United States: increasing reported incidence among
adolescents and adults, 1990--1996. Clin Infect Dis 1999;28:1230--7.
Tanaka M, Vitek CR, Pascual FB, Bisgard KM, Tate JE, Murphy TV. Trends in pertussis among infants in the United States, 1980--1999.
JAMA 2003;290:2968--75.
Yih WK, Lett SM, des Vignes FN, Garrison KM, Sipe PL, Marchant CD. The increasing incidence of pertussis in Massachusetts adolescents
and adults, 1989--1998. J Infect Dis 2000;182:1409--16.
Lapin LH. Whooping cough. 1st ed. Springfield, IL: Charles C.
Thomas; 1943.
American Academy of Pediatrics. Report of the Committee on Immunization and Therapeutic Procedures for Acute Infectious Diseases of
the American Academy of Pediatrics; 8th ed. In: Miller J, ed. Evanstown, IL: American Academy of Pediatrics; 1951.
Gordon J, Hood R. Whooping cough and its epidemiological anomalies. Am J Med Sci 1951;222:333--61.
Ipsen Jr J. Immunization of adults against diphtheria and tetanus.
N Engl J Med 1954;251:459--66.
Lloyd JC, Haber P, Mootrey GT, Braun MM, Rhodes PH, Chen RT. Adverse event reporting rates following tetanus-diphtheria and tetanus
toxoid vaccinations: data from the Vaccine Adverse Event Reporting System (VAERS), 1991--1997. Vaccine 2003;21:3746--50.
Macko MB, Powell CE. Comparison of the morbidity of tetanus toxoid boosters with tetanus-diphtheria toxoid boosters. Ann Emerg
Med 1985;14:33--5.
Rennels MB, Deloria MA, Pichichero ME, et al. Extensive swelling after booster doses of acellular pertussis-tetanus-diphtheria vaccine.
Pediatrics 2000;105:12.
Food and Drug Administration. Product approval information---licensing action, package insert: Tetanus Toxoid, Reduced Diphtheria Toxoid
and Acellular Pertussis Vaccine Adsorbed
ADACEL™. Sanofi pasteur. Rockville, MD: US Department of Health and Human Services, Food and
Drug Administration, Center for Biologics Evaluation and Research; 2006. Available at
http://www.fda.gov/cber/label/tdapave012306LB.pdf.
Food and Drug Administration. Product approval information---licensing action, package insert: BOOSTRIX®. Tetanus Toxoid, Reduced Diphtheria Toxoid and Acellular Pertussis Vaccine, Adsorbed. GlaxoSmithKline Biologicals. Rockville, MD: US Department of Health and
Human Services, Food and Drug Administration, Center for Biologics Evaluation and Research; 2005. Available at
http://www.fda.gov/cber/label/tdapgla122905LB.pdf.
Gilberg S, Njamkepo E, Du C, et al. Evidence of
Bordetella pertussis infection in adults presenting with persistent cough in a french area with very
high whole-cell vaccine coverage. J Infect Dis 2002;186:415--8.
Halperin SA. Canadian experience with implementation of an acellular pertussis vaccine booster-dose program in adolescents: implications for
the United States. Pediatr Infect Dis J 2005;24(Suppl 6):S141--S146.
National Health and Medical Research Council. The Australian Immunization Handbook. 8th ed. Canberra: Australian Government
Publishing Service; 2003.
Public Health Agency of Canada. An Advisory Committee Statement
(ACS), National Advisory Committee on Immunization (NACI):
statement on Adult/Adolescent Formulation of Combined Acellular Pertussis, Tetanus, and Diphtheria Vaccine. Canada Communicable Disease
Report 2000;26(ACS-1).
Public Health Agency of Canada. An Advisory Committee Statement
(ACS), National Advisory Committee on Immunization (NACI):
Prevention of Pertussis in Adolescents and Adults. Canada Communicable Disease Report 2003;29(ACS-5).
Tan T, Halperin S, Cherry JD, et al. Pertussis Immunization in the Global Pertussis Initiative North American Region: recommended strategies
and implementation considerations. Pediatr Infect Dis J 2005;24:S83--S86.
von Konig C, Campins-Marti M, Finn A, Guiso N, Mertsola J, Liese JG. Pertussis Immunization in the Global Pertussis Initiative
European Region: recommended strategies and implementation considerations. Pediatr Infect Dis J 2005;24:S87--S92.
Cherry J, Heinnger U. Pertussis and other
Bordetella infections. In: Feigin R, Cherry J, Demmler G, et al., eds. Textbook of Pediatric
Infectious Diseases. 5th ed. Philadelphia, PA: Saunders Co.; 2004.
Hewlett EL. A commentary on the pathogenesis of pertussis. Clin Infect Dis 1999;28(Suppl 2):S94--S98.
Mattoo S, Cherry JD. Molecular pathogenesis, epidemiology, and clinical manifestations of respiratory infections due to
Bordetella pertussis and other
Bordetella subspecies. Clin Microbiol Rev 2005;18:326--82.
Cherry JD. Epidemiological, clinical, and laboratory aspects of pertussis in adults. Clin Infect Dis 1999;28(Suppl 2):S112--S117.
Heininger U, Klich K, Stehr K, Cherry JD. Clinical findings in
Bordetella pertussis infections: results of a prospective multicenter surveillance
study. Pediatrics 1997;100:10.
Halperin SA, Wang EL, Law B, et al. Epidemiological features of pertussis in hospitalized patens in Canada, 1991--1997: Report of
the immunization monitoring program--Ace (IMPACT). Clin Infect Dis 1999;28:1238--43.
Vitek CR, Pascual FB, Baughman AL, Murphy TV. Increase in deaths from pertussis among young infants in the United States in the
1990s. Pediatr Infect Dis J 2003;22:628--34.
Preziosi M, Halloran M. Effects of pertussis vaccination on disease: vaccine efficacy in reducing clinical severity. Clin Infect Dis 2003;37:772--9.
Thomas M. Epidemiology of pertussis. Rev Infect Dis 1989;11:255--62.
Bisgard KM, Pascual FB, Ehresmann KR, et al. Infant pertussis: who was the source? Pediatr Infect Dis J 2004;23:985--9.
De Serres G, Shadmani R, Duval B, et al. Morbidity of pertussis in adolescents and adults. J Infect Dis 2000;182:174--9.
Lee GM, LeBaron C, Murphy TV, Lett S, Schauer S, Lieu TA. Pertussis in adolescents and adults: should we vaccinate? Pediatrics
2005;115:1675--84.
Lee GM, Lett S, Schauer S, et al. Societal costs and morbidity of pertussis in adolescents and adults. Clin Infect Dis 2004;39:1572--80.
Cherry JD, Grimprel E, Guiso N, Heininger U, Mertsola J. Defining pertussis epidemiology: clinical, microbiologic and serologic
perspectives. Pediatr Infect Dis J 2005;24:S25--S34.
Lind-Brandberg L, Welinder-Olsson C, Laggergard T, Taranger J, Trollfors B, Zackrisson G. Evaluation of PCR for diagnosis of
Bordetella pertussis and Bordetella
parapertussis infections. J Clin Microbiol 2005;36:679--83.
Young S, Anderson G, Mitchell P. Laboratory observations during an outbreak of pertussis. Clinical Microbiology Newsletter 1987;9:176--9.
van der Zee A, Agterberg C, Peeters M, Mooi F, Schellekens J. A clinical validation of
Bordetella pertussis and Bordetella
parapertussis polymerase chain reaction: comparison with culture and serology using samples from patients with suspected whooping cough from a highly
immunized population. J Infect Dis 1996;174:89--96.
Viljanen MK, Ruuskanen O, Granberg C, Salmi T. Serological diagnosis of pertussis: IgM, IgA and IgG antibodies against
Bordetella pertussis measured by Enzyme-linked immunosorbent assay (ELISA). Scandinavian Journal of Infectious Diseases 1982;14:117--22.
Hallander HO. Microbiological and serological diagnosis of pertussis. Clin Infect Dis 1999;28(Suppl 2):S99--S106.
Loeffelholz MJ, Thompson CJ, Long KS, Gilchrist MJ. Comparison of PCR, culture, and direct fluorescent-antibody testing for detection
of Bordetella pertussis. J Clin Microbiol 1999;37:2872--6.
He Q, Viljanen MK, Arvilommi H, Aittanen B, Mertsola J. Whooping cough caused by
Bordetella pertussis and Bordetella
parapertussis in an immunized population. JAMA 1998;280:635--7.
Lievano FA, Reynolds MA, Waring AL, et al. Issues associated with and recommendations for using PCR to detect outbreaks of pertussis. J
Clin Microbiol 2002;40:2801--5.
CDC. Guidelines for the control of pertussis outbreaks. Atlanta, GA: CDC; 2000.
Council of State and Territorial Epidemiologists. CSTE Position Statement 1997-ID-9: Public health surveillance, control and prevention
of pertussis. Atlanta, GA: Council of State and Territorial Epidemiologists; 1997.
Marchant CD, Loughlin AM, Lett SM, et al. Pertussis in Massachusetts, 1981--1991: incidence, serologic diagnosis, and vaccine effectiveness.
J Infect Dis 1994;169:1297--305.
Strebel P, Nordin J, Edwards K, et al. Population-based incidence of pertussis among adolescents and adults, Minnesota, 1995--1996. J Infect
Dis 2001;183:1353--9.
Ward JI, Cherry JD, Chang SJ, et al. Efficacy of an acellular pertussis vaccine among adolescents and adults. N Engl J Med 2005;353:1555--63.
Patriarca PA, Stellfeld M, Bielik RJ, Wassilak SG, Davis JP. Outbreaks of pertussis in the United States: the Wisconsin experience. Tokai J Exp
Clin Med 1988;13(Suppl):117--23.
Poel A, Ortega-Sanchez I, Tiwari T, Holmes T. Burden of disease and cost of a pertussis outbreak in a rural setting. Presented at the 40th
annual meeting of the Infectious Disease Society of America, Chicago, IL, October 24--27, 2002.
Sortir MJ, Cappazzo DL, Schmidt CE, et al. A Resource and labor intensive county-wide outbreak of pertussis, Wisconsin, 2003: high impact
on the adolescent population [Abstract]. In: Abstracts of the 39th National Immunization Conference, Washington, DC, March 21--24, 2005.
Heath CJ, Zusman J, Sherman L. Tetanus in the United States, 1950--1960. Am J Public Health 1964;54:769--79.
Srivastava P, Brown K, Chen J, Kretsinger K, Roper MH. Trends in tetanus epidemiology in the United States, 1972--2001. 39th
National Immunization Conference, Washington, DC, March 21--24, 2005.
McQuillan G, Kruszon-Moran D, Deforest A, Chu S, Wharton M. Serologic immunity to diphtheria and tetanus in the United States. Ann
Intern Med 2002;136:660--6.
Food and Drug Administration. Vaccines and Related Biological Products Advisory Committee, March 15, 2005: FDA BOOSTRIX® briefing information. Rockville, MD: US Department of Health and Human Services, Food and Drug Administration; 2005. Available at
http://www.fda.gov/ohrms/dockets/ac/05/briefing/2005-4097B1_1.pdf.
Food and Drug Administration. Vaccines and Related Biological Products Advisory Committee, March 15, 2005: FDA ADACEL™ briefing information. Rockville, MD: US Department of Health and Human Services, Food and Drug Administration; 2005. Available at
http://www.fda.gov/ohrms/dockets/ac/05/briefing/2005-4097B1_4a.pdf.
Food and Drug Administration. International Conference on Harmonization: Guidance on Statistical Principles for Clinical Trials. Federal
Register 1998;63(179):1--16.
Cherry J, Gornbein J, Heininger U, Stehr K. A search for serologic correlates of immunity to
Bordetella pertussis cough illnesses.
Vaccine 1998;16:1901--6.
Food and Drug Administration. GlaxoSmithKline Biologicals.
BOOSTRIX® briefing document. Bethesda, MD: US Department of Health
and Human Services, Food and Drug Administration, Center for Biologic Evaluation and Research; March 15, 2005. Available at
http://www.fda.gov.ohrms/ac/05/briefing/2005-4097B1_3.pdf.
Pichichero ME, Casey JR. Acellular pertussis vaccines for adolescents. Pediatr Infect Dis J 2005;24:S117--S26.
Schmitt HJ, von Konig CH, Neiss A, et al. Efficacy of acellular pertussis vaccine in early childhood after household exposure. JAMA
1996;275:37--41.
Pichichero ME, Rennels MB, Edwards KM, et al. Combined tetanus, diphtheria, and 5-component pertussis vaccine for use in adolescents
and adults. JAMA 2005;293:3003--11.
Gustafsson L, Hallander HO, Olin P, Reizenstein E, Storsaeter J. A controlled trial of a two-component acellular, a five- component acellular, and
a whole-cell pertussis vaccine [published erratum appears in N Engl J Med 1996 May 2; 334(18):1207]. N Engl J Medicine 1996;334:349--55.
Food and Drug Administration. Sanofi pasteur.
ADACEL™ briefing document. Bethesda, MD: US Department of Health and Human
Services, Food and Drug Administration, Center for Biologic Evaluation and Research; March 15, 2005. Available at
http://www.fda.gov/ohrms/dockets/ac/05/briefing/2005-4097B1_6.pdf.
Purdy KW, Hay JW, Botteman MF, Ward JI. Evaluation of strategies for use of acellular pertussis vaccine in adolescents and adults: a
cost-benefit analysis. Clin Infect Dis 2004;39:20--8.
Tetanus and Diphtheria Toxoids Adsorbed For Adult Use [package insert]. Massachusetts Public Health Biologic Laboratories, Boston, MA; 2000.
Tetanus and Diphtheria Toxoids Adsorbed For Adult Use [package insert]. Sanofi pasteur, Swiftwater, PA; 1996.
DECAVAC™. Tetanus and Diphtheria Toxoids Adsorbed For Adult Use [package insert]. Sanofi pasteur, Swiftwater, PA; 2005.
TENIVAC™. Tetanus and Diphtheria Toxoids Adsorbed For Adult Use [package insert]. Sanofi pasteur, Toronto Ontario Canada; 2005.
Tetanus Toxoid for Booster Use Only [package insert]. Sanofi pasteur, Swiftwater, PA; 2002.
Food and Drug Administration. Product approval information---licensing action, approval letter: BOOSTRIX®. Rockville, MD: US
Department of Health and Human Services, Food and Drug Administration, Center for Biologics Evaluation and Research; 2005. Available at
http://www.fda.gov/cber/approvltr/tdapgla050305L.htm.
Food and Drug Administration. Product approval
information---licensing action, approval letter: ADACEL™. Rockville, MD: US Department
of Health and Human Services, Food and Drug Administration, Center for Biologics Evaluation and Research; 2005. Available at
http://www.fda.gov/cber/approvltr/tdapave061005L.htm.
Bjorkholm B, Granstrom M, Wahl M, Hedstrom CE, Hagberg L. Adverse reactions and immunogenicity in adults to regular and increased
dosage of diphtheria vaccine. Eur J Clin Microbiol 1987;6:637--40.
Edsall G, Altman JS, Gaspar AJ. Combined tetanus-diphtheria immunization of adults: use of small doses of diphtheria toxoid. Am J Public
Health 1954;44:1537--45.
Edsall G, Elliott MW, Peebles TC, Eldred MC. Excessive use of tetanus toxoid boosters. JAMA 1967;202:111--3.
Galazka AM, Robertson SE. Immunization against diphtheria with special emphasis on immunization of adults. Vaccine 1996;14:845--57.
Pappenheimer A Jr., Edsall G, Lawrence H, Banton H. A study of reactions following administration of crude and purified diphtheria toxoid in
an adult population. Am J Hyg 1950;52:357--70.
Relyveld EH, Bizzini B, Gupta RK. Rational approaches to reduce adverse reactions in man to vaccines containing tetanus and diphtheria
toxoids. Vaccine 1998;16:1016--23.
James G, Longshore W Jr., Hendry J. Diphtheria immunization studies of students in an urban high school. Am J Hyg 1951;53:178--201.
Halperin SA, Scheifele D, Mills E, et al. Nature, evolution, and appraisal of adverse events and antibody response associated with the
fifth consecutive dose of a five-component acellular pertussis-based combination vaccine. Vaccine 2003;21:2298--306.
Liese JG, Stojanov S, Zink TH, et al. Safety and immunogenicity of Biken acellular pertussis vaccine in combination with diphtheria and
tetanus toxoid as a fifth dose at four to six years of age. Munich Vaccine Study Group. Pediatr Infect Dis J 2001;20:981--8.
Scheifele DW, Halperin SA, Ferguson AC. Assessment of injection site reactions to an acellular pertussis-based combination vaccine,
including novel use of skin tests with vaccine antigens. Vaccine 2001;19:4720--6.
Woo EJ, Burwen DR, Gatumu SN, Ball R. Extensive limb swelling after immunization: reports to the Vaccine Adverse Event Reporting
System. Clin Infect Dis 2003;37:351--8.
Rennels MB. Extensive swelling reactions occurring after booster doses of diphtheria-tetanus-acellular pertussis vaccines. Semin Pediatr Infect
Dis 2003;14:196--8.
Jefferson T, Rudin M, Di Pietrantonj C. Adverse events after immunisation with aluminium-containing DTP vaccines: systematic review of
the evidence. Lancet Infect Dis 2004;4:84--90.
Froehlich H, Verma R. Arthus reaction to recombinant hepatitis B virus vaccine. Clin Infect Dis 2001;33:906--8.
Moylett EH, Hanson IC. Mechanistic actions of the risks and adverse events associated with vaccine administration. J Allergy Clin
Immunol 2004;114:1010--20.
Nikkels A, Nikkels-Tassoudji N, Pierard G. Cutaneous adverse reactions following anti-infective vaccinations. Am J Clin Dermatol 2005;6:79--87.
Stratton KR, Howe CJ, Johnston RB Jr. Adverse events associated with childhood vaccines other than pertussis and rubella. Summary of a
report from the Institute of Medicine. JAMA 1994;271:1602--5.
Terr AI. Immune-Complex Allergic Diseases. In: Parslow TG, Stites DP, Terr AI, Imboden JB, eds. Medical immunology. 10th ed. Lange
Medical Books/McGraw0Hill Companies Inc.; 2001.
Ponvert C, Scheinmann P. Vaccine allergy and pseudo-allergy. Eur J Dermatol 2003;13:10--5.
Halperin S, Sweet L, Baxendale D. How soon after prior tetanus-diphtheria vaccination can one give an adult-formulation
tetanus-diphtheria pertussis vaccine? Pediatr Infect Dis J 2006 (in press).
Friedland LR. Evaluation of Safety of Reduced Antigen Content Tetanus-Diphtheria-Acellular Pertussis (Tdap) Vaccine in Adolescents as a
6th consecutive dose of acellular-pertussis containing vaccine. 45th Interscience Conference on Antimicrobial Agents and Chemotherapy,
Washington, DC, December 16--19, 2005.
David ST, Hemsley C, Pasquali PE, Larke B, Buxton JA, Lior LY. Enhanced surveillance for vaccine-associated adverse events: dTap catch-up
of high school students in Yukon. Can Commun Dis Rep 2005;31:117--26.
Public Health Agency of Canada. An Advisory Committee Statement
(ACS), National Advisory Committee on Immunization (NACI):
interval between administration of vaccines against diphtheria, tetanus, and pertussis. Canada Communicable Disease Report 2005;31(ACS-8 and
9):17--24.
Food and Drug Administration. Aventis Pasteur. Menactra® briefing document. Bethesda, MD: US Department of Health and Human
Services, Center for Biologic Evaluation and Research; September 22, 2004. Available at
http://www.fda.gov/ohrms/dockets/ac/04/briefing/4072B1_1.pdf.
Pichichero ME, Blatter MM, Kennedy WA, Hedrick J, Descamps D, Friedland LR. Acellular pertussis vaccine booster combined with
diphtheria and tetanus toxoids for adolescents. Pediatrics 2006 (in press).
Food and Drug Administration. Vaccines and Related Biological Products Advisory Committee, September 22, 2004: FDA Menactra® briefing information. Rockville, MD: US Department of Health and Human Services, Food and Drug Administration; 2004. Available at
http://www.fda.gov/ohrms/dockets/ac/04/briefing/4072B1_2a.pdf.
Moore DL, Le Saux N, Scheifele D, Halperin SA. Lack of evidence of encephalopathy related to pertussis vaccine: active surveillance by
IMPACT, Canada, 1993--2002. Pediatr Infect Dis J 2004;23:568--71.
Kuno-Sakai H, Kimura M. Safety and efficacy of acellular pertussis vaccine in Japan, evaluated by 23 years of its use for routine
immunization. Pediatr Int 2004;46:650--5.
Braun MM, Mootrey GT, Salive ME, Chen RT, Ellenberg SS. Infant immunization with acellular pertussis vaccines in the United
States: assessment of the first two years' data from the Vaccine Adverse Event Reporting System (VAERS). Pediatrics 2000;106:E51.
DuVernoy TS, Braun MM. Hypotonic-hyporesponsive episodes reported to the Vaccine Adverse Event Reporting System (VAERS),
1996--1998. Pediatrics 2000;106:E52.
Le Saux N, Barrowman NJ, Moore DL, Whiting S, Scheifele D, Halperin S. Decrease in hospital admissions for febrile seizures and reports
of hypotonic-hyporesponsive episodes presenting to hospital emergency departments since switching to acellular pertussis vaccine in Canada: a
report from IMPACT. Pediatrics 2003;112:e348.
Rosenthal S, Chen R, Hadler S. The safety of acellular pertussis vaccine vs whole-cell pertussis vaccine. A postmarketing assessment. Arch
Pediatr Adolesc Med 1996;150:457--60.
CDC. Guide to contraindications, 2003. Atlanta, GA: CDC; 2003.
Pollard JD, Selby G. Relapsing neuropathy due to tetanus toxoid. Report of a case. J Neurol Sci 1978;37:113--25.
Tuttle J, Chen RT, Rantala H, Cherry JD, Rhodes PH, Hadler S. The risk of Guillain-Barre syndrome after tetanus-toxoid-containing vaccines
in adults and children in the United States. Am J Public Health 1997;87:2045--8.
Fenichel G. Assessment: neurologic risk of immunization: report of the Therapeutics and Technology Assessment Subcommittee of the
American Academy of Neurology. Neurology 1999;52:1546--52.
Maclennan R, Schofield FD, Pittman M, Hardegree MC, Barile MF. Immunization against neonatal tetanus in New Guinea. Antitoxin response
of pregnant women to adjuvant and plain toxoids. Bull World Health Organ 1965;32:683--97.
Newell KW, Duenas LA, LeBlanc DR, Garces ON. The use of toxoid for the prevention of tetanus neonatorum. Final report of a double-blind
controlled field trial. Bull World Health Organ 1966;35:863--71.
Schofield FD, Tucker VM, Westbrook GR. Neonatal tetanus in New Guinea. Effect of active immunization in pregnancy. Br Med
J 1961;5255:785--9.
United Nations Children's Fund, World Health Organization, and United Nations Population Fund. Maternal and Neonatal Tetanus
Elimination by 2005: Strategies for Achieving and Maintaining Elimination, November 2000 (WHO/V&B/02.09). Geneva, Switzerland: World
Health Organization; 2002.
Healy CM, Munoz FM, Rench MA, Halasa NB, Edwards KM, Baker CJ. Prevalence of pertussis antibodies in maternal delivery, cord, and
infant serum. J Infect Dis 2004;190:335--40.
Van Savage J, Decker MD, Edwards KM, Sell SH, Karzon DT. Natural history of pertussis antibody in the infant and effect on vaccine response.
J Infect Dis 1990;161:487--92.
Van Rie A, Wendelboe AM, Englund JA. Role of maternal pertussis antibodies in infants. Pediatr Infect Dis J 2005;24:S62--S65.
Czeizel A, Rockenbauer M. Tetanus toxoid and congenital abnomalities. Int J Gynaecol Obstet 1999;64:253--8.
Silveira CM, Caceres VM, Dutra MG, Lopes-Camelo J, Castilla EE. Safety of tetanus toxoid in pregnant women: a hospital-based
case-control study of congenital anomalies. Bull World Health Organ 1995;73:605--8.
Braun MM, Patriarca PA, Ellenberg SS. Syncope after immunization. Arch Pediatr Adolesc Med 1997;151:255--9.
Woo E, Ball R, Braun R. Fatal syncope-related fall after immunization. Arch Pediatr Adolesc Med 2005;159:1083.
American Academy of Pediatrics. In: Pickering LK, ed. Red book: 2003 Report of the Committee on Infectious Diseases. 26th ed. Elk
Grove Village, IL: American Academy of Pediatrics; 2003.
Graham DR, Dan BB, Bertagnoll P, Dixon RE. Cutaneous inflammation caused by inadvertent intradermal administration of DTP instead
of PPD. Am J Public Health 1981;71:1040--3.
Institute for Safe Medication Practices. Hazard Alert! Confusion between tetanus diphtheria toxoid (Td) and tuberculin purified protein
derivative (PPD) led to unnecessary treatment. Huntingdon Valley, PA: Institute for Safe Medication Practices; 2003.
Russell M, Pool V, Kelso JM, Tomazic-Jezic VJ. Vaccination of persons allergic to latex: a review of safety data in the Vaccine Adverse
Event Reporting System (VAERS). Vaccine 2004;23:664--7.
Wendelboe AM, Van Rie A, Salmaso S, Englund JA. Duration of immunity against pertussis after natural infection or vaccination. Pediatr
Infect Dis J 2005;24:S58--S61.
Ball R, Braun MM, Mootrey GT. Safety data on meningococcal polysaccharide vaccine from the Vaccine Adverse Event Reporting System.
Clin Infect Dis 2001;32:1273--80.
Use of trade names and commercial sources is for identification only and does not imply endorsement by the U.S. Department of
Health and Human Services.References to non-CDC sites on the Internet are
provided as a service to MMWR readers and do not constitute or imply
endorsement of these organizations or their programs by CDC or the U.S.
Department of Health and Human Services. CDC is not responsible for the content
of pages found at these sites. URL addresses listed in MMWR were current as of
the date of publication.
All MMWR HTML versions of articles are electronic conversions from ASCII text
into HTML. This conversion may have resulted in character translation or format errors in the HTML version.
Users should not rely on this HTML document, but are referred to the electronic PDF version and/or
the original MMWR paper copy for the official text, figures, and tables.
An original paper copy of this issue can be obtained from the Superintendent of Documents,
U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800.
Contact GPO for current prices.
**Questions or messages regarding errors in formatting should be addressed to
[email protected].