Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail.
Appendix A
Immunization Management Issues
Hepatitis B Vaccine Dose and Administration
Recommended vaccine doses vary by product, age of
recipient, and needs of special populations (see Table 2).
Although the antigen contents of vaccines differ, vaccines made by different manufacturers are interchangeable for all
adult schedules.
Hepatitis B vaccine should be administered by intramuscular injection. The deltoid muscle is the recommended site
of administration for adults. Injection into the buttock is associated with decreased immunogenicity
(1--4). Intradermal administration can result in a lower seroconversion rate and final concentration of antibody to hepatitis B surface
antigen (anti-HBsAg) compared with intramuscular administration; limited data are available to assess long-term protection
from this route of administration (5,6).
For intramuscular injection, the needle should be long enough to reach the muscle mass and prevent vaccine from
seeping into subcutaneous tissue, but not so long as to involve underlying nerves and blood vessels or bone
(7). The appropriate needle length for adults is 1"--1½"
(25--38 mm), depending on the recipient's weight (1" [25 mm] for males and
females weighing <60 kg [<130 lbs]; 1"--1½" [25--38 mm] for females weighing 60--90 kg [130--200 lbs] and males
weighing 60--118 kg [130--260 lbs]; and 1½" [38 mm] for females weighing >90 kg [>200 lbs] and males weighing >118 kg
[>260 lbs]). A 22- to 25-gauge needle should be used.*
Hepatitis B vaccine administered by any route or site other than intramuscularly in the deltoid muscle should not
be counted as valid and should be repeated unless serologic testing indicates that an adequate response has been achieved
(see Postvaccination Testing for Serologic
Response).
Hepatitis B vaccine and other vaccines administered during the same visit should be given in different injection sites.
For persons at risk for hemorrhage (e.g., persons with hemophilia), the risk for bleeding after intramuscular
injection can be minimized by using a 23-gauge (or smaller) needle, applying direct pressure to the injection site for 1--2 minutes,
and administering vaccine immediately after infusion of coagulation factor. Subcutaneous administration of vaccine can
be considered for these persons but might result in lower response and increased local reaction.
Hepatitis B vaccine should be stored at 35°F--46°F
(2°C--8oC) and should not be frozen.
A vaccine information statement (VIS) must be provided
to recipients of hepatitis B vaccine. The National
Childhood Vaccine Injury Act of 1986 (42 U.S.C. § 300aa-26)
requires vaccine providers to give a copy of the most current
vaccine-specific VIS to all recipients of vaccines that are included on the National Vaccine Injury Compensation Program
table maintained by the Health Resources and Services Administration (available at
http://www.hrsa.gov). Hepatitis B
vaccine is included on this table. The most current VIS for hepatitis B vaccine is available at
http://www.cdc.gov/nip/publications/vis. Statements in
languages other than English are available from the
Immunization Action Coalition at http://www.immunize.org.
Adverse events should be reported to the Vaccine Adverse Events Reporting System; report forms and assistance
are available from CDC at telephone 1-800-822-7967 or at
http://www.vaers.hhs.gov.
Hepatitis B Immune Globulin (HBIG) Dose and Administration
The standard dose of HBIG is 0.06 mL/kg for all
applications in adults.
HBIG may be administered simultaneously with
hepatitis B vaccine but in a different injection site.
HBIG is administered by intramuscular injection. An appropriate muscle mass (i.e., deltoid or gluteal) should be
chosen in which to deliver the large volumes of HBIG required by using a needle length appropriate for the person's age and
size (7).
HBIG should be stored at 35°F--46°F (2°C--8°C) and should not be frozen.
Unknown or Uncertain Vaccination Status
A reliable vaccination history is defined as a written, dated record (e.g., personal, school, physician, or
immunization registry) of each dose of a complete series.
In the majority of clinical practice settings, providers should accept only written and dated records as evidence
of vaccination. Although vaccinations should not be postponed if records cannot be located, providers
should try to locate missing records by contacting previous health-care providers and asking patients to search for personally held records.
Persons whose records cannot be located should be considered susceptible and started or continued on the age-appropriate
vaccine schedule.
In settings in which written vaccination records are not accessible (e.g., sexually transmitted disease [STD]
treatment facilities, human immunodeficiency virus [HIV] testing facilities, or correctional facilities), an oral history of completing
a hepatitis B vaccine series can be used to defer hepatitis B vaccination. Persons in these settings who are uncertain
about their vaccination status should be vaccinated. Other methods for assessing vaccination history (e.g., assuming a
person received hepatitis B vaccine to comply with preschool or middle school entry requirements or participation in the
U.S. military) might be considered, but such methods require further research before they can be recommended as
reliable alternatives.
Determining immunity from previous infection through serologic testing is an alternative to vaccination. However,
using serologic testing to assess immunity from vaccination in persons with unknown or uncertain vaccination status can
be problematic (see Prevaccination Serologic Testing for Susceptibility).
Persons who reside in the United States but were vaccinated in other countries should be considered fully vaccinated
if they have written documentation of >3 doses of vaccine administered at recommended minimum
intervals, including the final dose at age
>24 weeks. If they were not vaccinated according to recommended minimum intervals, they should
be revaccinated (see Minimum Dosing Intervals and Management of Persons Who Were Vaccinated Incorrectly).
Persons without written documentation of full vaccination should receive doses to complete the age-appropriate vaccine series.
Interrupted Vaccine Schedules
When the hepatitis B vaccine schedule is interrupted, the vaccine series does not need to be restarted.
If the series is interrupted after the first dose, the second dose should be administered as soon as possible, and the
second and third doses should be separated by an interval of at least 8 weeks.
If only the third dose has been delayed, it should be administered as soon as possible.
Minimum Dosing Intervals and Management of Persons Who Were
Vaccinated Incorrectly
The third dose of vaccine must be administered at least
8 weeks after the second dose and should follow the first dose
by at least 16 weeks; the minimum interval between the first and second doses is 4 weeks.
Inadequate doses of hepatitis B vaccine (see Table 2) or doses received after a shorter-than-recommended dosing
interval should be readministered, using the correct
dosage or schedule.
Accelerated Vaccine Schedules
The Food and Drug Administration has not approved accelerated schedules in which hepatitis B vaccine
is administered more than once in 1 month. If an accelerated schedule (e.g., doses at 0, 7, and 14
days) is used, the patient also should receive a booster dose at least 6 months after the start of the series to promote long-term immunity.
Hemodialysis Patients and Other Immunocompromised Persons
Hepatitis B vaccination is recommended for pre--end-stage renal disease patients before they become dialysis
dependent and for peritoneal and home dialysis patients
because they might require in-center hemodialysis.
Higher hepatitis B vaccine doses are recommended for adult dialysis patients and other immunocompromised persons
(see Table 2).
Serologic testing of hemodialysis patients and other immunocompromised persons is recommended 1--2 months
after administration of the final dose of the primary vaccine series to determine the need for revaccination (see
Postvaccination Testing for Serologic Response). In addition, booster doses of vaccine might be needed (see Booster Doses).
Prevaccination Serologic Testing for Susceptibility
Vaccination of persons who are immune to hepatitis B virus (HBV) infection because of current or previous
infection or vaccination does not increase the risk for
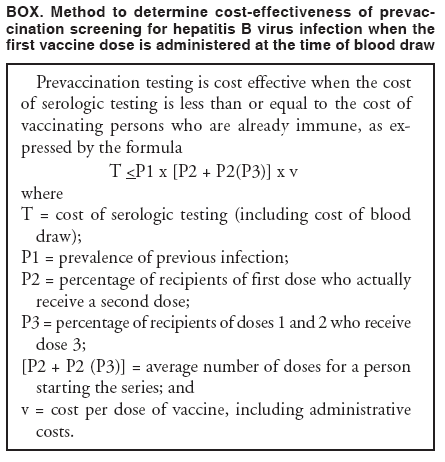
adverse events. However, in adult populations that have expected high rates
of previous HBV infection, prevaccination testing might reduce costs by avoiding vaccination of persons who are
already immune (Box). Prevaccination testing is recommended for all foreign-born persons (including immigrants,
refugees, asylum seekers, and internationally adopted children) born in Africa, Asia, the Pacific Islands, and other regions with
high endemicity of HBV infection (HBsAg prevalence of
>8%) (see Figure 4 and Box, Appendix C); for household, sex,
and needle-sharing contacts of HBsAg-positive persons; and for HIV-infected persons
(8). In addition, testing might be cost effective in adult populations with a prevalence of HBV infection of >20% (e.g., injection-drug
users, incarcerated persons, men who have sex with men; and persons born in countries with intermediate levels
of endemic HBV infection [HBsAg prevalence of 2%--7%] [see Figure 4 and Box 2]). In a study conducted in
correctional facilities, the cost of prevaccination testing was equivalent to vaccination without testing at a threshold prevalence of
HBV infection of 25% (9).
Prevaccination testing can be done with a single test (anti-HBc) or with a panel of tests (e.g., HBsAg and anti-HBs).
The typical interpretation of HBV serologic markers has been described (see Table 1).
When a single test is used, testing for anti-HBc is preferred because it identifies all persons with previous HBV
infection, including persons with chronic HBV infection.
If prevaccination testing for anti-HBs is used to identify immunity after previous HBV infection, HBsAg testing also
must be performed to identify persons with chronic HBV infection. However, for persons who were vaccinated previously
or whose vaccination status is unknown, interpretation of anti-HBs results can be problematic. Postvaccination
anti-HBs concentrations decline over time, and vaccine responders remain protected even when anti-HBs concentrations are
no longer detectable; therefore, a negative anti-HBs result does not necessarily indicate lack of immunity in
vaccinated persons. In addition, an anti-HBs-positive result can occur even for persons who received
>1 dose of vaccine but did not complete the series. However, long-term protection has been
demonstrated only for persons who have completed a
licensed vaccination series and have ever had an anti-HBs concentration of
>10 mIU/mL; persons with an anti-HBs-positive result but who did complete a vaccine schedule might not have long-term protection from HBV
infection.
Serologic testing should not be a barrier to vaccination of susceptible persons, especially in populations that are difficult
to access. The first vaccine dose typically should be administered immediately after collection of the blood sample
for serologic testing.
Postvaccination Testing for Serologic Response
Serologic testing for immunity is not necessary after
routine vaccination of adults.
Testing after vaccination is recommended only for the following persons whose subsequent clinical management
depends on knowledge of their immune status:
--- Health-care workers and public safety workers at high risk for continued percutaneous or mucosal exposure to blood
or body fluids (e.g., acupuncturists, dentists, dental hygienists, emergency medical technicians, first
responders, laboratory technologists/technicians, nurses, nurse practitioners, phlebotomists, physicians, physician assistants,
and students entering these professions), to determine the need for revaccination and to guide postexposure
prophylaxis. Testing persons at low risk for continued mucosal or percutaneous
exposure to blood or body fluids (e.g., public
safety workers and health-care workers without direct patient contact) is not likely to be cost effective. Health-care and
public safety workers who have written documentation of a complete vaccine series but who have never had
postvaccination testing do not need serologic testing for anti-HBs unless they have a percutaneous or mucosal exposure to blood
or body fluids (10).
--- Chronic hemodialysis patients, HIV-infected persons, and other immunocompromised persons
(e.g., hematopoietic stem-cell transplant recipients or persons receiving chemotherapy), to determine the need
for revaccination and the type of follow-up testing.
--- Sex partners of HBsAg-positive persons, to determine the need for revaccination and for other
methods of protection against HBV infection.
Testing should be performed 1--2 months after administration of the last dose of the vaccine series using a method
that allows determination of a protective concentration of anti-HBs
(>10 mIU/mL).
Persons found to have anti-HBs concentrations of
>10 mIU/mL after the primary vaccine series are considered to
be immune.
--- Immunocompetent persons have long-term protection and do not need further periodic testing to assess
anti-HBs levels.
--- Immunocompromised persons might need annual testing to assess anti-HBs concentrations (see Booster Doses).
Persons found to have anti-HBs concentrations of <10 mIU/mL after the primary vaccine series should be
revaccinated. Administration of 3 doses on an appropriate schedule (see Box 5), followed by anti-HBs testing
1--2 months after the third dose, usually is more practical than serologic testing after 1 or more doses of vaccine.
Persons who do not have a protective concentration of anti-HBs after revaccination should be tested for HBsAg.
--- If the HBsAg test result is positive, the person should receive appropriate management, and any household, sex,
or needle-sharing contacts should be identified and vaccinated (see Appendix C).
--- Persons who test negative for HBsAg should be considered susceptible to HBV infection and should be
counseled about precautions to prevent HBV infection and the need to obtain HBIG postexposure prophylaxis for any known
or likely parenteral exposure to HBsAg-positive blood
(10).
Booster Doses
Booster doses are not recommended for persons with normal immune status who were vaccinated as infants,
children, adolescents, or adults. Serologic testing is not recommended to assess antibody concentrations in any age group, except
in certain circumstances (see Postvaccination Testing for Serologic Response).
For hemodialysis patients, the need for booster doses should be assessed by annual anti-HBs testing. A booster dose
should be administered when anti-HBs levels decline
to <10 mIU/mL.
For other immunocompromised persons (e.g.,
HIV-infected persons, hematopoietic stem-cell transplant
recipients, and persons receiving chemotherapy), the need for booster doses has not been determined. When anti-HBs levels decline
to <10 mIU/mL, annual anti-HBs testing and booster doses should be considered for persons with an ongoing risk
for exposure.
References
Shaw FE Jr, Guess HA, Roets JM, et al. Effect of anatomic injection site, age and smoking on the immune response to hepatitis B
vaccination. Vaccine 1989;7:425--30.
Weber DJ, Rutala WA, Samsa GP, Santimaw JE, Lemon SM. Obesity as a predictor of poor antibody response to hepatitis B plasma vaccine.
JAMA 1985;254:3187--9.
Ukena T, Esber H, Bessette R, Parks T, Crocker B, Shaw FE Jr. Site of injection and response to hepatitis B vaccine. N Engl J Med 1985;
313:579--80.
Bryan JP, Sjogren MH, MacArthy P, Cox E, Legters LJ, Perine PL. Persistence of antibody to hepatitis B surface antigen after low-dose,
intradermal hepatitis B immunization and response to a booster dose. Vaccine 1992;10:33--8.
Coberly JS, Townsend T, Repke J, Fields H, Margolis H, Halsey NA. Suboptimal response following intradermal hepatitis B vaccine in
infants. Vaccine 1994;12:984--7.
CDC. General recommendations on immunization 2006: recommendations of the Advisory Committee on Immunization Practices
(ACIP). MMWR. In press.
Use of trade names and commercial sources is for identification only and does not imply endorsement by the U.S. Department of
Health and Human Services.References to non-CDC sites on the Internet are
provided as a service to MMWR readers and do not constitute or imply
endorsement of these organizations or their programs by CDC or the U.S.
Department of Health and Human Services. CDC is not responsible for the content
of pages found at these sites. URL addresses listed in MMWR were current as of
the date of publication.
Disclaimer
All MMWR HTML versions of articles are electronic conversions from ASCII text
into HTML. This conversion may have resulted in character translation or format errors in the HTML version.
Users should not rely on this HTML document, but are referred to the electronic PDF version and/or
the original MMWR paper copy for the official text, figures, and tables.
An original paper copy of this issue can be obtained from the Superintendent of Documents,
U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800.
Contact GPO for current prices.
**Questions or messages regarding errors in formatting should be addressed to
[email protected].