|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail. Malaria Surveillance --- United States, 1996
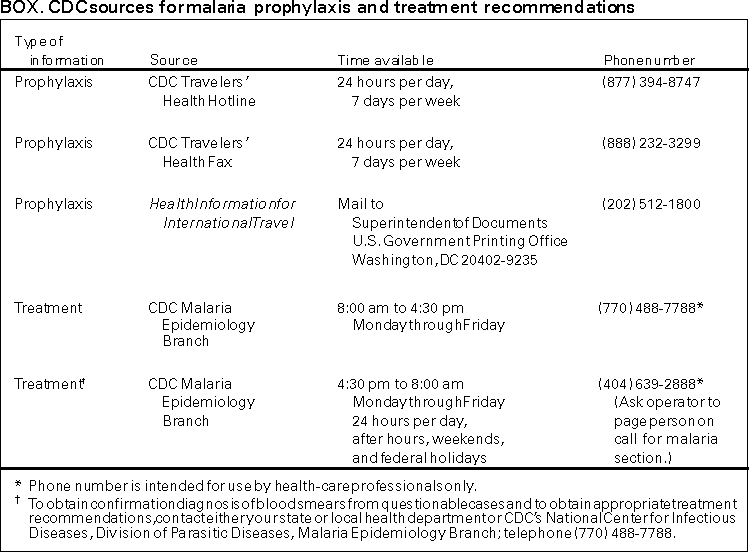
Mary Mungai, M.D., M.P.H., M.Sc.1,2 1Epidemic Intelligence Service, Epidemiology Program Office AbstractProblem/Condition: Malaria is caused by four species of intraerythrocytic protozoa of the genus Plasmodium (i.e., P. falciparum, P. vivax, P. ovale, or P. malariae), which are transmitted by the bite of an infected female Anopheles sp. mosquito. Most malaria infections in the United States occur in persons who have traveled to areas with ongoing transmission. Occasionally, cases occur in the United States through exposure to infected blood products, by congenital transmission, or by local mosquitoborne transmission. National public health surveillance for malaria is conducted to identify episodes of local transmission and to guide prevention recommendations for travelers. Reporting Period Covered: Cases with onset of illness during 1996. Description of System: Malaria cases confirmed by blood smears are reported to local and/or state health departments by healthcare providers and/or laboratory staff. Case investigations are conducted by local and/or state health departments, and reports are transmitted to CDC through the National Malaria Surveillance System (NMSS). Data from NMSS serve as the basis for this report. Results: CDC received reports of 1,392 cases of malaria with onset of symptoms during 1996 among persons in the United States or one of its territories. This number represents an increase of 19.3% from the 1,167 cases reported for 1995. P. vivax, P. falciparum, P. malariae, and P. ovale were identified in 47.4% 37.4%, 5.4%, and 2.0% of cases, respectively. More than one species was present in four patients (0.3% of total). The infecting species was not determined in 104 (7.5%) cases. The number of reported malaria cases acquired in Africa (n=585)increased by 12.7% compared with 1995; cases acquired in Asia increased by 31.9% (n=442); and cases acquired in the Americas increased by 13.0% (n=278). Of 614 U.S. civilians who acquired malaria abroad, 97 (15.8%) had followed a chemoprophylactic drug regimen recommended by CDC for the area where they had traveled. Eleven patients became infected in the United States. Of these 11 cases, three were congenitally acquired; one was acquired by organ transplantation; one was acquired by a blood transfusion; two were acquired through infusion using a heparin lock; and one was acquired by a mosquito bite in a laboratory setting. In three cases, the source of infection was unknown. Five deaths were attributed to malaria. Interpretation: The 19.3% increase in malaria cases in 1996 compared with 1995 resulted primarily from increases in cases acquired in Africa and Asia. This increase could have resulted from local changes in disease transmission, increased travel to these regions, improved reporting from state and local health departments, or a decreased use of effective antimalarial chemoprophylaxis. In most reported cases, U.S. civilians who acquired infection abroad were not on an appropriate chemoprophylaxis regimen for the country where they acquired malaria. Public Health Actions: Additional information was obtained concerning the five fatal cases and the 11 infections acquired in the United States. In 1996, malaria prevention guidelines were updated and distributed to healthcare providers. Persons traveling to a malarious area should take the recommended chemoprophylaxis regimen and use personal protection measures to prevent mosquito bites. Any person who has been to a malarious area and who subsequently develops a fever or influenzalike symptoms should seek medical care immediately; investigation should include a blood smear for malaria. Malaria infections can be fatal if not diagnosed and treated promptly. Recommendations concerning prevention of malaria can be obtained from CDC's Health Information for International Travel.* INTRODUCTIONMalaria is caused by infection with any of four species of Plasmodium (i.e., P. falciparum, P. vivax, P. ovale, and P. malariae) that can infect humans. The infection is transmitted by the bite of an infective female Anopheles sp. mosquito. Malaria infection remains a devastating global problem, with an estimated 300--500 million cases occurring annually. Forty-one percent of the world's population lives in areas where malaria is transmitted (e.g., parts of Africa, Asia, Central America and South America, Hispaniola, the Middle East, and Oceania), and approximately 1.5--2.7 million persons die of malaria each year (1). In previous years, malaria was also endemic throughout much of the continental United States; an estimated 600,000 cases occurred during 1914 (2). During the late 1940s, a combination of improved socioeconomic conditions, water management, vectorcontrol efforts, and case management was successful at interrupting malaria transmission in the United States. Since then, malaria case surveillance has been maintained to detect locally acquired cases that could indicate the reintroduction of transmission and to monitor patterns of antimalarial drug resistance seen among U.S. travelers. Through 1996, most cases of malaria diagnosed in the United States have been imported from regions of the world where malaria transmission is known to occur. Each year, several congenital infections and infections resulting from exposure to blood or blood products are reported in the United States. In addition, a few cases are reported that might have been acquired through local mosquitoborne transmission (3). State and/or local health departments and CDC thoroughly investigate all malaria cases acquired in the United States, and CDC conducts an analysis of all imported cases to detect trends in acquisition. This information has been used to guide malaria prevention recommendations for travelers abroad. For example, an increase in P. falciparum malaria among U.S. travelers to Africa, an area with increasing chloroquineresistance, prompted CDC in 1990 to change the recommended chemoprophylaxis from chloroquine to mefloquine (4). The signs and symptoms of malaria illness are variable, but most patients have fever. Other common symptoms include headache, back pain, chills, increased sweating, myalgia, nausea, vomiting, diarrhea, and cough. The diagnosis of malaria should be considered for any person who has these symptoms and has traveled to an area with known malaria transmission. Malaria should also be considered in the differential diagnosis of persons who have a fever of unknown origin, regardless of their travel history. Untreated P. falciparum infections can progress to coma, renal failure, pulmonary edema, and death. Asymptomatic parasitemia can occur among persons who have been longterm residents of malarious areas. This report summarizes malaria cases reported to CDC with onset of symptoms in 1996. METHODSSources of Data Data regarding malaria cases are reported to both the National Malaria Surveillance System (NMSS) and the National Notifiable Diseases Surveillance System (NNDSS) (5). All nationally notifiable diseases, which includes malaria, are reported to CDC through NNDSS. The numbers of reported cases might differ because of differences in the collection and transmission of data. A comparison was made of cases in 10 states** that reported to NMSS and NNDSS. To determine the completeness of reporting to the two systems and to obtain an estimate of the total number of cases in these 10 states, cases were matched using variables that included state, age (+5 years), sex, race, and date of onset of illness (+1 month). The capture-recapture methodology (6) was used to compare NMSS and NNDSS. NMSS receives more detailed clinical and epidemiologic data regarding each case (e.g., information concerning the area where the infected person has traveled) than NNDSS. This information is needed for programmatic decision making (e.g., CDC takes this information into account when making recommendations for malaria chemoprophylaxis). Cases of blood-smear--confirmed malaria are identified by healthcare providers and/or laboratories. Each slideconfirmed case is reported to local and/or state health departments and to CDC on a uniform case report form that contains clinical, laboratory, and epidemiologic information. CDC staff review all report forms at the time of receipt and request additional information if necessary (e.g., when no recent travel to a malarious country is reported). Reports of other cases are telephoned directly by health-care providers to CDC, usually when assistance with diagnosis or treatment is requested. All cases that have been acquired in the United States are investigated, including all induced and congenital cases and possible introduced or cryptic cases. Information derived from uniform case report forms is entered into a database and analyzed annually. Definition of Terms The following definitions are used in this report:
This report also uses terminology derived from the recommendations of the World Health Organization (7). Definitions of the following terms are included for reference.
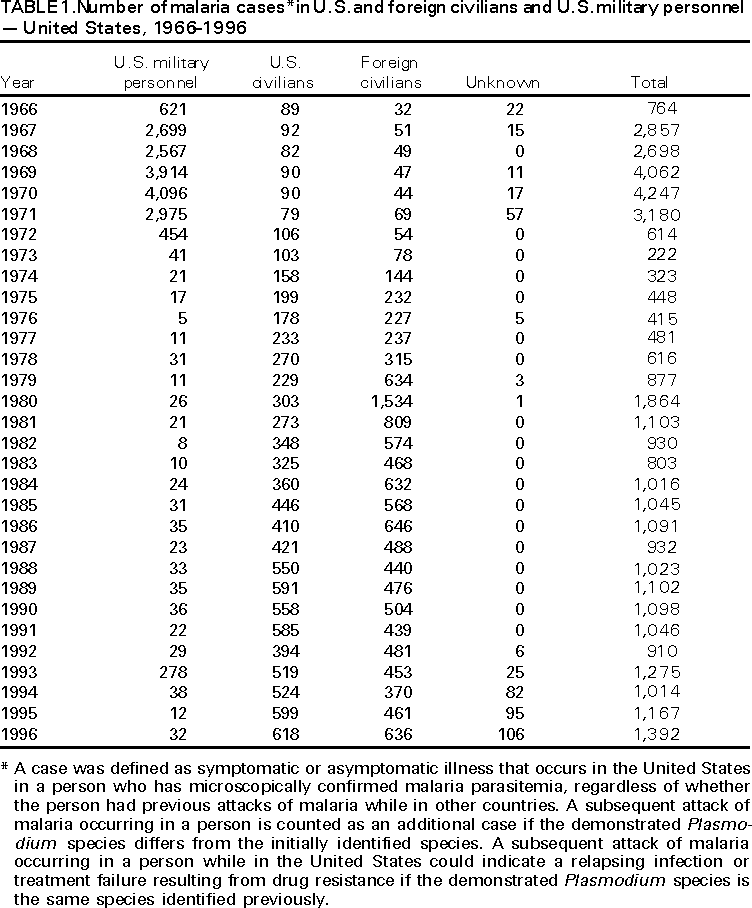
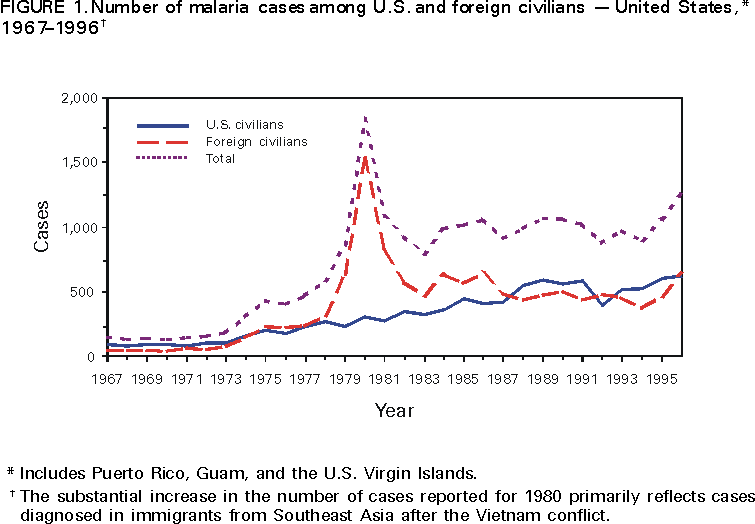
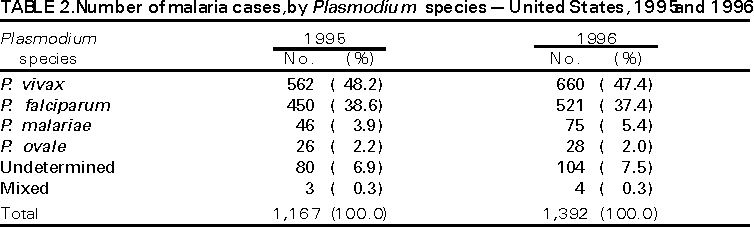
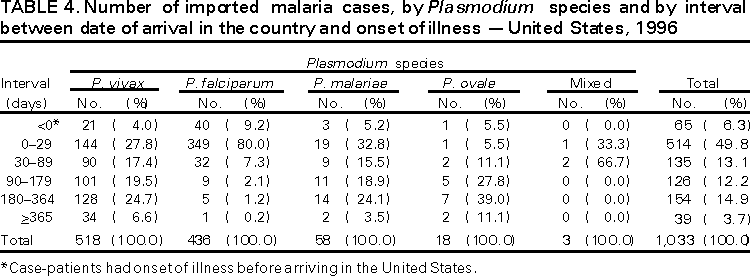
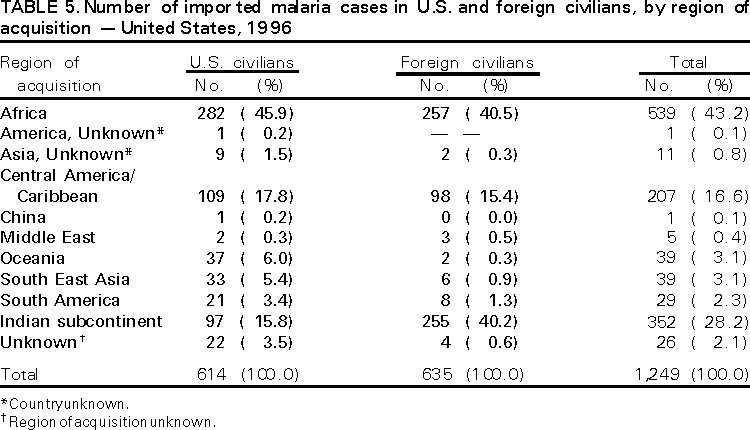
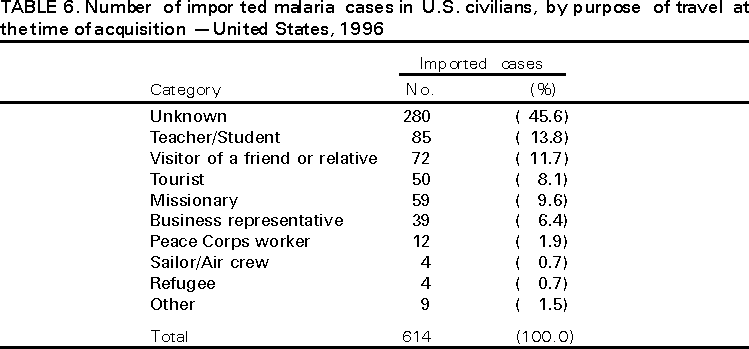
Microscopic Diagnosis of Malaria The early diagnosis of malaria requires that physicians consider malaria in the differential diagnosis of every patient who has fever; the evaluation of such a patient should include taking a comprehensive travel history. If malaria is suspected, a Giemsa-stained smear of the patient's peripheral blood should be examined for parasites. Thick and thin blood smears must be prepared properly because the accuracy of diagnosis depends on the quality of the blood film and the experience of the laboratory personnel.*** (See Appendix for proper procedures for accurately diagnosing malaria). RESULTSGeneral Surveillance During 1996, CDC received reports of 1,392 malaria cases through NMSS that had onset of symptoms among persons in the United States and its territories, representing a 19.3% increase from the 1,167 cases reported for 1995 (8). This incidence is the largest number of reported cases since 1980 and represents the largest number of U.S. civilian cases reported since 1966 (Table 1). Since 1988, with the exception of 1992, malaria among U.S civilians has accounted for most of the cases reported to CDC. In 1996, 618 cases occurred in U.S. civilians compared with 599 cases reported for 1995, whereas the number of cases in foreign civilians increased from 461 cases to 636 (Figure 1). Cases among U.S. military personnel increased from 12 in 1995 to 32 in 1996. In 106 cases, information was not sufficient to determine whether the person was a civilian or in the military. In the comparison of NMSS and NNDSS, 294 cases were reported to NMSS from the 10 selected states, and 505 were reported to NNDSS. Two hundred thirteen cases were reported to both systems. Using both the Chandra Sekar-Deming and Lincoln-Peterson Capture-Recapture methods, the total estimated number of cases in these states was 697 (660, 734, 95% confidence interval), and an estimated 111 cases were missed by both systems. The completeness of reporting to NMSS and NNDSS was 42% and 72%, respectively. Plasmodium Species The infecting species of Plasmodium was identified in 1,288 (92.5%) of the cases reported in 1996. P. vivax and P. falciparum were identified in blood smears from 47.4% and 37.4% of infected persons, respectively (Table 2). The 660 P. vivax cases reported for 1996 represented a 17.4% increase from the 562 cases in 1995, whereas the number of P. falciparum infections increased by 15.8% (from 450 in 1995 to 521 in 1996). Among 1,244 cases in which both the region of acquisition and the infecting species were known, 80.3% of infections acquired in Africa were attributed to P. falciparum, whereas 7.6% were attributed to P. vivax. The converse was true of malaria infections acquired in Asia and the Americas: 83.6% and 81.5% were attributed to P. vivax, and only 10.7% and 13.7% were attributed to P. falciparum, respectively. Region of Acquisition and of Diagnosis Of all reported cases, 99% (n=1,381) were imported. Of 1,337 imported cases in which the region of acquisition was known, most (n=585; 43.7%) were acquired in Africa, whereas 33.1% (n=442) and 20.0% (n=267) were acquired in Asia and the Americas, respectively (Table 3). The highest concentration of cases acquired in Africa (n=406; 69.4%) came from countries in West Africa, whereas most (n=381; 86.2%) of the cases acquired in Asia came from the Indian subcontinent. The other regions where imported cases of malaria were acquired were Central America and Caribbean (17.1%), South America (2.2%) and Oceania (3.1%). Information regarding region of acquisition was missing for 44 (3.2%) of the 1,381 imported cases. In Africa, the number of reported malaria cases acquired (n=585) in 1996 increased by 12.3% compared with 1995; in Asia, the number of cases increased by 31.5% (n=442) in 1996 compared with 1995. Cases from the Americas increased by 8.5% (n=267) in 1996 compared with 1995. In the United States, the five areas reporting the highest number of malaria cases were California (n=350), New York City (n=292), Florida (n=113), New York (n=92), and Virginia (n=53) (Figure 2). Florida, which ranked fifth in number of cases in 1995, ranked third in 1996, an increase of 73.8% (from 65 cases in 1995 to 113 cases in 1996). New York City, which began reporting cases to CDC in 1993, reported a 23% increase in cases in 1996 compared with 1995. This increase in the reported number of cases might be a result of increased international travel, improved access to health care, or more sensitive surveillance for both Florida and New York City. Interval Between Arrival and Illness Both the interval between the date of arrival in the United States and onset of illness, and the identification of the infecting Plasmodium species were known for 1,033 (74.8%) of the imported cases of malaria (Table 4). Symptoms began after arrival in the United States for 968 (93.7%) of these cases. Clinical malaria developed within 1 month after arrival in 349 (80.0%) of the 436 P. falciparum cases and in 144 (27.8%) of the 518 P. vivax cases (Table 4). Only 39 (3.8%) of the 1,033 persons became ill >1 year after returning to the United States. An additional 65 persons reported becoming ill before arriving in the United States. Imported Malaria Cases Imported Malaria in Military Personnel Thirty-two cases of imported malaria in U.S. military personnel were reported for 1996. Eight of these cases occurred in personnel of the U.S. Army; seven cases, U.S. Air Force; three cases, U.S. Marine Corps; and three cases, U.S. Navy. In 11 cases, the branch of the military was unknown. Of the 28 case-patients for whom information on use of chemoprophylaxis was available, eight persons did not use any chemoprophylaxis. Imported Malaria in Civilians A total of 1,249 imported malaria cases were reported among civilians. Of these, 614 (49.2%) cases occurred among U.S. residents, and 635 (50.8%) occurred among residents of other countries (Table 5). Of the 614 imported malaria cases in U.S. civilians, 282 (45.9%) had been acquired in Africa, approximately the same number reported in 1995. The Central American and Caribbean region accounted for 109 (17.8%) cases of imported malaria in U.S. civilians, whereas travel to the Indian subcontinent accounted for an additional 97 (15.8%) cases. Of the 635 imported cases among foreign civilians, most cases were acquired in either Africa (n=257; 40.5%) or the Indian subcontinent (n=255; 40.2%). Use of Antimalarial Chemoprophylaxis Use of Chemoprophylaxis Among U.S. Civilians. Information concerning the use of chemoprophylaxis was known for 559 (91.0%) of the 614 U.S. civilians who had imported malaria. Of these 559 persons, 313 (56.0%) had not taken any chemoprophylaxis, and 149 (26.7%) had not taken a drug recommended by CDC for the area visited. Only 97 (17.3%) U.S. civilians had taken a medication recommended by CDC (9). Seventy-five of these patients had taken mefloquine weekly; 10 had taken doxycycline daily; and 12 who had traveled only in areas where chloroquine-resistant malaria has not been documented had taken chloroquine weekly. Of the 149 patients taking a nonrecommended drug, information on the type of chemoprophylaxis used was known for 112. Of these 112 persons, 63 (56.3%) reported taking chloroquine during travel to an area where chloroquine resistance had been documented. Malaria Infection After Use of Recommended Prophylaxis. A total of 111 patients (97 U.S. civilians, five persons in the U.S. military, four foreigners, and five persons with missing information) developed malaria after taking a recommended antimalarial drug. Although the length of time before symptom onset for all 111 cases was determined, the infecting species could not be determined for nine cases. Cases of P. vivax or P. ovale. Of the 111 patients who developed malaria after using recommended chemoprophylaxis, 72 cases (64.9%) were caused by P. vivax (n=66) or P. ovale (n=6). Malaria case surveillance reports indicated that 10 (13.9%) of these patients were noncompliant with their antimalarials. Fifty-three (73.6%) cases of P. vivax or P. ovale occurred >45 days after the case-patients arrived in the United States. These cases were consistent with relapsing infections and, thus, do not indicate prophylaxis failures. Because of insufficient information regarding 12 cases of P. vivax malaria, it could not be determined whether these cases were relapsing infections. Onset of symptoms in these cases began before the persons returned to the United States. Seven cases of P. vivax occurred within 45 days after the patient returned to the United States. Of these case-patients, none was among the 10 who were known to be noncompliant with the antimalarial chemoprophylaxis. Region of acquisition varied widely for these seven cases (one from Central America, one from South America, one from India, two from Oceania, one from Southeast Asia, and one from Africa), and serum drug levels could not be checked for any of these patients because blood samples were not available. The most likely explanations for these cases are either inappropriate dosing or noncompliance. No evidence existed that would indicate the emergence of a new area of chloroquine-resistant P. vivax. The remaining 39 cases of malaria reported among persons who had taken a recommended antimalarial drug for chemoprophylaxis included 26 cases of P. falciparum, 4 cases of P. malariae, and 9 cases in which the infecting species was not identified. Cases of P. falciparum. Twenty-three of the 26 P. falciparum cases were acquired in Africa, whereas the other three cases were acquired in Asia. In 13 (50.0%) of the case-patients, noncompliance with recommended antimalarials was reported. The remaining 13 cases of P. falciparum that were acquired while the patient was reported to have used appropriate chemoprophylaxis varied in region of acquisition. Ten were acquired in Africa (seven in West Africa, two in East Africa, and one in southern Africa), whereas the other three were acquired in Asia (one each in Thailand, India, and Indonesia). Serum drug levels of the antimalarials were unavailable for these patients. The most likely explanations for these cases are either inappropriate dosing or noncompliance. Purpose of Travel. The purpose of travel to malarious areas was reported for 325 (52.9%) of the 614 U.S. civilians with imported malaria (Table 6). Of the cases among U.S. civilians, the largest percentage (13.8%) traveled to teach or study, and the second and third largest (11.7% and 9.6%) traveled to visit a friend or relative or to do missionary work. Malaria Acquired in the United States Congenital Malaria Three cases of congenital malaria were reported in 1996. Case 1. On November 30, 1996, a full-term male infant was delivered by spontaneous vaginal delivery in Washington, D.C. His mother had immigrated to the United States from Nicaragua 2 months before delivery. She reported beginning malaria chemoprophylaxis in Nicaragua when she was 5 months pregnant but had stopped taking the medication after arriving in the United States. When she was 8 months pregnant, she had been hospitalized with fever and was diagnosed and treated for malaria. The species was reported as "most likely P. vivax"; the therapy she received was not known. On the day before delivery, she was diagnosed with P. falciparum malaria and was treated with chloroquine after delivery. On December 8, 1996, the infant was hospitalized because of a 1-day history of fever, vomiting, lethargy, and refusal to feed. His physical examination and laboratory tests (cerebrospinal fluid analysis, white blood cell count, hemoglobin, and blood and urine cultures) were normal. The infant received no antimicrobial therapy and was discharged after 24 hours with a diagnosis of viral gastroenteritis. On December 16, the infant was readmitted with a persistent fever of 101 F (38 C) and splenomegaly. His peripheral blood smears demonstrated the presence of P. falciparum rings (parasitemia <0.5%). He rapidly defervescenced after chloroquine therapy was initiated. Case 2. A female infant was born in October 1996 in California. Her mother had traveled to Mexico for 2 weeks when she was 8 months pregnant and had not used malaria chemoprophylaxis during her travel. While in Mexico, she had been diagnosed and treated for malaria, but the species and therapy received were not known nor was it known if she received further evaluation or treatment after her return to the United States. On December 5, 1996, the infant, aged 7 weeks, was hospitalized with a 1-week history of fever. Her blood smears demonstrated P. vivax malaria; evaluation of the mother's blood smears revealed Plasmodium parasites of an undetermined species, although she was asymptomatic. The baby was treated successfully with mefloquine; the therapy received by the mother was not known. Case 3. In December 1995, a full-term female infant was delivered by spontaneous vaginal delivery in New York City. The mother had immigrated to the United States from India when she was 7 months pregnant. She had not had a malaria-like illness during her pregnancy and reported that her last episode of malaria-like symptoms, which remitted without treatment, had been 2 years earlier. On January 24, 1996, the infant, aged 1 month, was hospitalized with a 1-day history of fever and chills. Examination of her blood smears indicated P. vivax. She responded well to chloroquine therapy. The mother's blood smears did not demonstrate malaria parasites, and she was discharged without treatment. Upon receiving the surveillance report of this case, CDC contacted the hospital to advise that the mother should receive treatment, but she could not be contacted. Cryptic Malaria Four cases of cryptic malaria were reported in 1996. Case 1. On July 22, 1996, a man aged 40 years who was homeless and unemployed was admitted to a hospital with a 1-week history of fever, vomiting, and headache. The patient lived in Florida. CDC confirmed the presence of P. vivax (parasitemia <1%) in his blood smears. He recovered after treatment with quinine and sulfadoxine-pyrimethamine. The patient had never traveled outside of the United States; in the previous 3 years, his only travel had been to New York and Georgia. Although he had a history of intravenous heroin use 20 years earlier, he had no recent history of parenteral drug use nor did the examining physician find any evidence of drug abuse. The patient had never received blood or blood products. Case 2. On July 30, 1996, a man aged 45 years who lived in Florida was admitted to a hospital with a 4-day history of fever. CDC confirmed the diagnosis of P. vivax parasitemia. The patient was treated successfully with chloroquine and primaquine. The patient, who was homeless, was employed as a house painter. He lived approximately 1 mile away from Case 1. He had never traveled outside of Florida and had no other known risk factors for malaria. The local and state health departments, with assistance from CDC, conducted an investigation to determine a potential source of infection for both cases. An entomologic assessment of the areas where both patients lived was conducted. Breeding sites and adult Anopheles mosquitoes were found near the first patient's shelter. Epidemiologic investigation did not reveal other cases of malaria in the vicinity of the two cases. Although both cases were presumed to have been locally acquired mosquitoborne infections, they were classified as cryptic cases because a source of infection could not be identified. Case 3. On May 22, 1996, a man aged 53 years was hospitalized in Georgia with a 12-day history of fever, chills, fatigue, and myalgias. CDC confirmed the diagnosis of P. vivax parasites in his blood smears. He was treated successfully with chloroquine and primaquine. The patient was born on the Texas-Mexico border, more than 500 miles from the nearest malarious area in Mexico. He was a farmworker in southwest Georgia and had lived in the United States for more than 10 years. He had returned to Mexico once (in August 1993) since emigration, where he traveled no further than 70 miles from the Texas border, which is more than 400 miles away from the malarious areas in Mexico. The patient reported never having had a blood transfusion or having used parenteral drugs. He said that during May and June 1996, he had spent nights at a mobile-home park and at a small encampment of trailers contiguous to the farm. The state health department conducted an investigation to determine a potential source of the patient's infection. Anopheles quadrimaculatus larvae and adults were found in the vicinity of the two sites where the patient had spent nights around the time of his illness. The epidemiologic investigation indicated that large populations of migrant laborers from malarious areas of Mexico and Central America worked in the area where the patient acquired his infection. However, because a source of infection could not be identified, the case was classified as cryptic. Case 4. On April 28, 1996, a man aged 65 years was evaluated at a hospital in Georgia; he had a 6-day history of fever. CDC confirmed the diagnosis of P. vivax parasitemia in his blood smears. He responded well to treatment with chloroquine and primaquine. The patient had no history of recent travel outside of the United States, transfusion with blood or blood products, or parenteral drug use. However, he did work as an entomologist in a laboratory where he routinely handled infected anopheline mosquitoes, and before his infection, he had been working with A. stephensi that were infected with a strain of P. vivax from Thailand. He reported having been bitten by several mosquitos in the laboratory. He had no previous history of malaria. Although this infection was believed to have been acquired through mosquitoborne transmission in the laboratory, it was classified as cryptic because it could not be linked epidemiologically to other cases. Induced Malaria Four cases of induced malaria were reported in 1996: one acquired by organ transplantation; one by blood transfusion; and two nosocomial infections acquired through infusions using a heparin lock. Case 1. A woman aged 33 years who had immigrated to New York City from Nigeria in 1991 developed end-stage renal disease of unknown etiology. On November 29, 1996, she underwent a renal transplant; the patient did not receive blood or blood products at the time of the transplant. On December 14, she developed fever. Intraerythrocytic organisms, initially identified as P. falciparum, were identified on blood smears. Microscopic examination at CDC identified the species as P. ovale. She responded well to treatment with chloroquine and primaquine. The patient reported having had malaria during her childhood in Nigeria but had not traveled out of the United States since emigrating. She had never had a blood transfusion or used intravenous drugs. The kidney donor was the patient's brother, who had come directly from Nigeria. At the time of his arrival in the United States, he reportedly was not feeling well, but the nature of his illness was unknown. He had not been evaluated for malaria before the kidney donation, and it was not known whether he was tested after his sister was diagnosed. Case 2. A man aged 70 years who had Waldenström macroglobulinemia was hospitalized in Missouri on November 27, 1996; he had a 2-day history of fever. Peripheral blood smears showed intraerythrocytic parasites suspected to be either Plasmodium or Babesia. Despite treatment with oral quinine and clindamycin, the patient developed respiratory and renal failure and died on November 30. The patient had not traveled outside of the United States since the 1940s but had been transfused with seven units of packed red blood cells in 1996 (two in May, two in June, and three in November). The presence of P. falciparum parasites in the patient's blood smears (6% parasitemia) was confirmed at CDC. Stored sera from all seven donors were tested for antimalarial antibodies at CDC using the indirect fluorescent antibody (IFA) test. One of the November donors, an Army reservist (at a basic training installation) whose blood was collected by a civilian blood center, had elevated titers of 1:16,384 to P. falciparum; 1:256 to both P. malariae and P. ovale; and 1:64 to P. vivax. Blood smears obtained from this donor in March 1997 revealed rare P. falciparum rings, and DNA of the same species was detected by polymerase chain reaction of the whole blood. The donor reported no febrile illness around the time of the blood donation. He had immigrated to the United States from Nigeria in April 1996. He was treated with oral quinine and doxycycline. Case 3. On February 11, 1996, a man aged 84 years who had multiple medical problems, including congestive heart failure, syncope, and bradycardia was admitted to a hospital in Florida with a 12-day history of fever and chills. P. vivax parasites were identified on blood films that had been obtained for a complete blood count (CBC) on admission. Microscopic diagnosis was confirmed at CDC. He responded well to treatment with chloroquine. The patient's most recent travel outside of the United States was approximately 15 years previously on a cruise ship to the Bahamas. He had no other risk factors for malaria. However, during January 22--24, he had been hospitalized for bradycardia and had been placed in a room adjacent to a patient with imported P. vivax malaria acquired in Bolivia. During his hospitalization, he had four venipunctures, and intravenous medications were administered through a heparin lock. Case 4. On January 20, 1996, a woman with chronic obstructive pulmonary disease was admitted to the same hospital in Florida as Case 3. The patient, aged 60 years, was admitted with respiratory congestion and shortness of breath. She had a fever of 101 F (38 C) on admission but was subsequently afebrile throughout her hospitalization. In addition, during her hospitalization, she had multiple venipunctures and was administered intravenous drugs through a heparin lock. The patient improved and was discharged on January 26. On February 12, she was readmitted with a 2-day history of fever and chills. CDC confirmed the diagnosis of P. vivax parasites on blood films that had been obtained for CBC on admission. She was treated successfully with chloroquine. The patient had no risk factors for malaria, but during her initial hospitalization during January 20--26, she had also stayed in a room adjacent to the patient with imported P. vivax malaria from Bolivia (as had the patient in Case 3). The local health department, assisted by the state, conducted an epidemiologic investigation of Cases 3 and 4 to determine the source of the infections. None of the health-care workers at the hospital had been ill with malaria-like symptoms. The room of the patient with imported malaria was between the rooms where the other two patients stayed. The windows in these rooms had screens, and the windows were never opened. Intravenous drugs were administered by the same health-care worker to all three patients via an intravenous line for the index case-patient and via heparin locks for the other two case-patients. Hospital workers routinely used 10 cc vials of heparinized solution to flush heparin locks and occasionally used the same vial for two or more patients. Although this practice could not be directly linked to the three cases, it seemed the most plausible explanation for their infections. After the investigation, the hospital routinely began using single-dose vials for flushing intravenous devices. Deaths Attributed to Malaria Five deaths attributed to malaria were reported in 1996. Case 1. On January 26, 1996, a woman aged 53 years who had emigrated from Somalia on January 25 was evaluated at a hospital emergency room in California because of fever. She was discharged with a diagnosis of a viral syndrome; information regarding whether she received any treatment was unknown. When she returned to the hospital 4 days later, she was semicomatose, had acute renal failure, and respiratory distress. Blood smears taken on the day of her emergency room visit 4 days earlier were examined; P. falciparum ring forms (15% parasitemia) were found. Intravenous quinidine and exchange transfusion were initiated. Although parasitemia cleared and her renal function improved, she never regained consciousness and died on February 8. Case 2. On March 31, 1996, a male pilot aged 57 years was admitted to a hospital in Florida 1 week after having returned from a trip to several countries in sub-Saharan Africa (Kenya, South Africa, and Nigeria). The patient had used no malaria chemoprophylaxis during his travels. His family reported that he had a 5-day history of fever, lethargy, and jaundice. On admission, he was comatose, had generalized seizures, hemolytic anemia, metabolic acidosis, acute renal failure, hypotension, and hypoglycemia. CDC confirmed the diagnosis of P. falciparum parasites in his blood smears. Therapy was initiated with intravenous quinidine; preparations were being made for exchange blood transfusion when he died 1 day after admission. Case 3. On August 25, 1996, a boy aged 10 years who had emigrated from Guinea, West Africa, 8 days previously was evaluated in an emergency room of a hospital in New York City because of a 2-day history of fever, chills, headache, and generalized seizures. On examination, he was found to have hemolytic anemia and altered mental status. CDC confirmed the diagnosis of P. falciparum rings in his blood smears. He died in the emergency room before therapy could be initiated. Case 4. On October 21, 1996, a woman aged 32 years was admitted to a hospital in New York City. Her complaints and the findings of her physical examination on admission were unknown. Her blood smears revealed P. falciparum parasites. Attempts to obtain information related to her therapy and the succession of events leading to her death were unsuccessful because her hospital record remains closed because of litigation. Case 5. Case 2, an induced case described previously, was a fatal case that was induced through blood transfusion at a hospital in Missouri. DISCUSSIONA total of 1,392 cases of malaria were reported to CDC for 1996, representing a 19.3% increase from the 1,167 cases reported for 1995. This increase primarily resulted from an increase in cases acquired in Africa and Asia that might have resulted from improved reporting, increased international travel, changing patterns of travel (i.e., emigration from malarious areas or "adventure tourism"), or a decreased use of effective antimalarial chemoprophylaxis. Some limitations of the matching process used for the comparison of NMSS and NNDSS included
Despite these limitations, the comparison demonstrated that substantial numbers of cases are not being captured by one or both systems. More cases are being reported to NNDSS; one contributing factor appears to be that some state health departments only report to NNDSS and not to NMSS. The NNDSS and NMSS surveillance systems are currently assessing the feasibility of developing an integrated approach for electronically reporting malaria case data from the states and territories to CDC. The objectives of this effort are to decrease reporting burden in the states, streamline reporting of data to CDC, and achieve more consistency in the format of data reported to CDC. One reason for conducting malaria surveillance is to monitor the emergence of drug resistance and the consequent failure of chemoprophylaxis; however, more than 80% of imported malaria cases among U.S. civilians occurred in persons who were either not taking or taking nonrecommended prophylaxis for the region to which they were traveling. Of the 111 persons who reported taking adequate prophylaxis, for 24 cases (i.e., seven P. vivax, 13 P. falciparum, and four P. malariae) sufficient information was not available to determine whether they represented problems with compliance while using proper antimalarial chemoprophylaxis, reporting errors, or emerging drug resistance. However, no conclusive evidence existed to suggest a single national or regional source of infection among this group of patients. Health-care providers are encouraged to contact CDC if they suspect chemoprophylaxis failure, thus enabling measurement of serum drug levels of the antimalarial drug in question. The importance of taking proper precautions and chemoprophylaxis is underscored by the five fatal cases of malaria that occurred in the United States in 1996, including one case in a U.S. civilian who was not on prophylaxis during his exposure in malarious areas. An earlier review of deaths attributed to malaria in the United States identified several risk factors for fatal malaria, including a) failure to take recommended antimalarial chemoprophylaxis, b) refusal to or delay in seeking medical care, and c) misdiagnosis (10). Signs and symptoms of malaria might be vague, but fever is generally present. Other symptoms include headache, chills, increased sweating, back pain, myalgia, diarrhea, nausea, vomiting, and cough. Prompt diagnosis requires that malaria be included in the differential diagnosis of illness in a febrile person with a recent history of travel to a malarious area. Clinicians should ask febrile patients for a travel history, particularly when evaluating febrile illnesses in international visitors, immigrants, refugees, migrant laborers, and international travelers. Treatment for malaria should be initiated immediately after the diagnosis has been confirmed by a positive blood smear. Treatment should be determined on the basis of the infecting Plasmodium species, the probable geographic origin of the parasite, the parasite density, and the patient's clinical status (11). Although non-falciparum malaria rarely causes severe complications, P. falciparum malaria can cause severe, life-threatening complications. Healthcare workers are encouraged to consult appropriate sources for malaria treatment recommendations or to contact CDC's National Center for Infectious Diseases, Division of Parasitic Diseases, Malaria Epidemiology Branch (Box). AcknowledgmentThe authors gratefully acknowledge the state health departments, health-care providers, and laboratories for reporting data to CDC. References
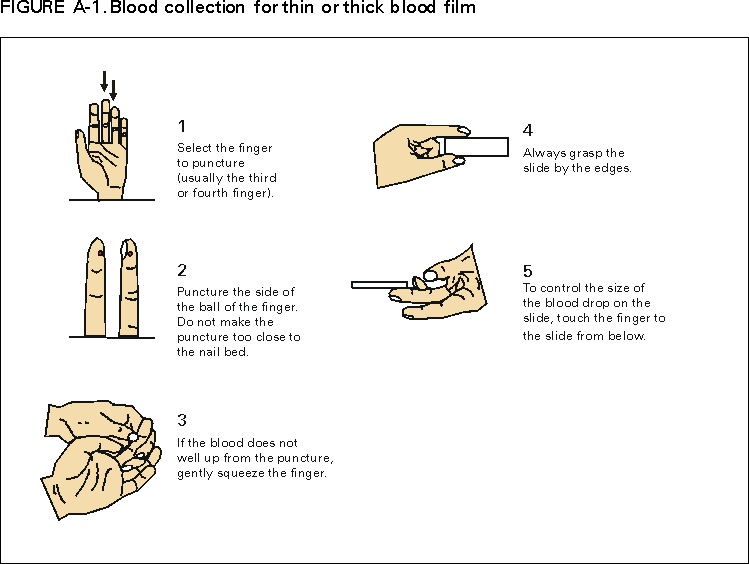
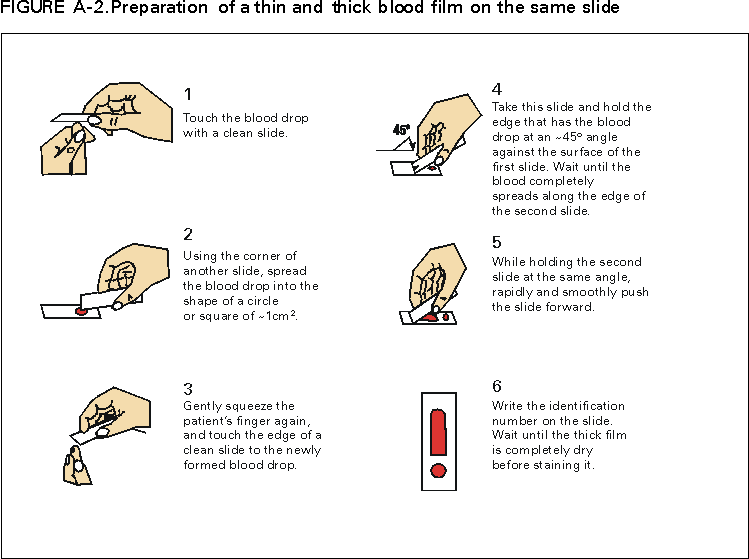
* To obtain confirmation diagnosis of blood smears from questionable cases and to obtain appropriate treatment recommendations, contact either your state or local health department or CDC's National Center for Infectious Diseases, Division of Parasitic Diseases, Malaria Epidemiology Branch; telephone (770) 488-7788. ** Florida, Hawaii, Illinois, Maine, Massachusetts, Missouri, New Jersey, Tennessee, Texas, and Washington. *** To obtain confirmation diagnosis of blood smears from questionable cases and to obtain appropriate treatment recommendations, contact either your state or local health department or CDC's National Center for Infectious Diseases, Division of Parasitic Diseases, Malaria Epidemiology Branch; telephone (770) 488-7788. APPENDIXMicroscopic Procedures for Diagnosing Malaria To establish the diagnosis of malaria, a blood smear must be prepared from fresh blood obtained by pricking the finger (Figures A-1 and A-2).* The thin smear is fixed in methanol before staining; the thick smear is stained unfixed. Many hospitals have a Wright-Giemsa stain available, which is acceptable; however, Wright stain alone will not reliably stain Plasmodium parasites. For best results, the smear should be stained with a 3% Giemsa solution (pH of 7.2) for 30--45 minutes. In P. falciparum infections, the parasite density should be estimated by counting the percentage of red blood cells infected --- not the number of parasites --- under an oil immersion lens on a thin film. Thick blood smears are more sensitive in detecting malaria parasites because the blood is concentrated, allowing a greater volume of blood to be examined. However, thick smears are more difficult to read, and thin smears might be preferred by laboratories that have limited experience. Plasmodium parasites are always intracellular, and they demonstrate, if stained correctly, blue cytoplasm with a red chromatin dot. Common errors in reading malaria smears are caused by platelets overlying a red blood cell, concern about missing a positive slide, and misreading artifacts as parasites. Persons suspected of having malaria but whose blood smears do not show the presence of parasites should have blood smears repeated approximately every 12--24 hours for 3 consecutive days. If smears remain negative, then the diagnosis of malaria is unlikely. For rapid diagnosis, make the thick and thin smears on separate slides. Air dry the thin film, fix it with methyl alcohol, and immediately stain it. If no parasites are found on the thin film, wait until the thick film is dry, and examine it for organisms that might not have been detected on the thin preparation. * In Figures A-1 and A-2, the hands are shown ungloved to better illustrate their placement during the procedures. However, wearing gloves while processing blood specimens is recommended to prevent transmission of bloodborne pathogens (MMWR 1988;37:377--82, 387--8 and MMWR 1987;36[No. S2]). Table 1
All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to [email protected].Page converted: 3/21/2001 |
|||||||||
This page last reviewed 5/2/01
|