|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
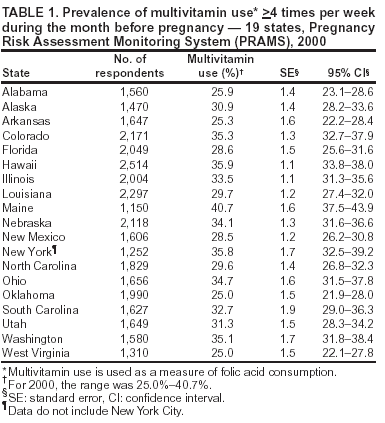
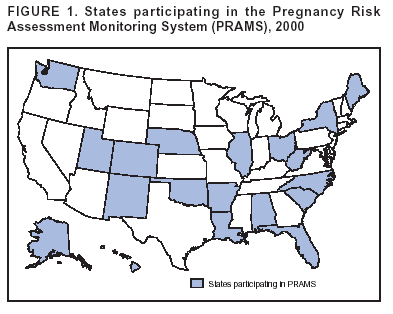
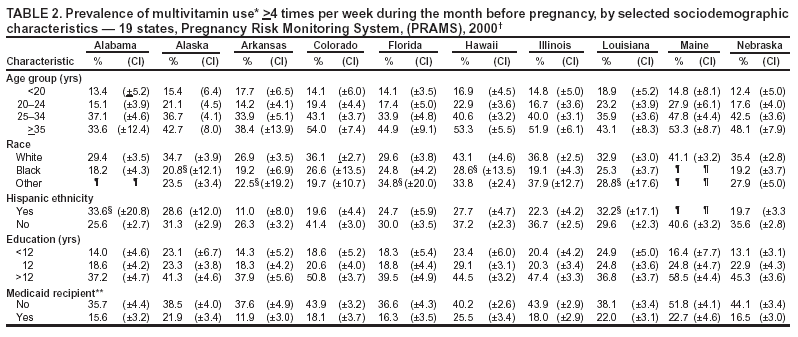
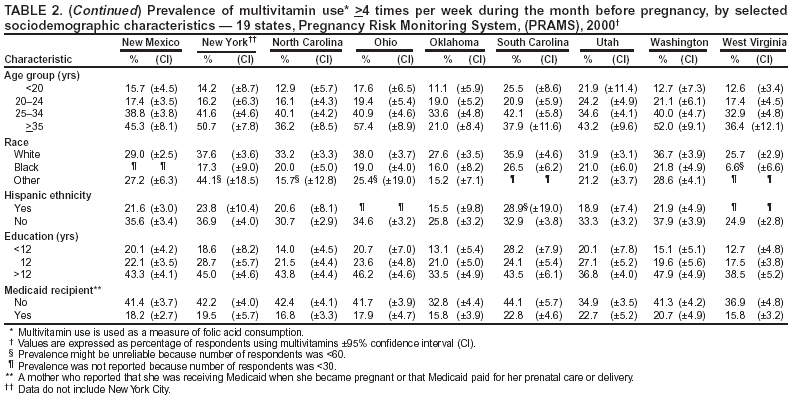
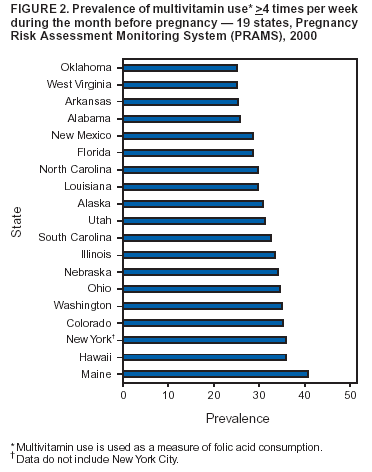
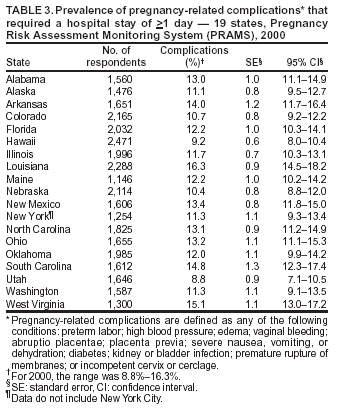
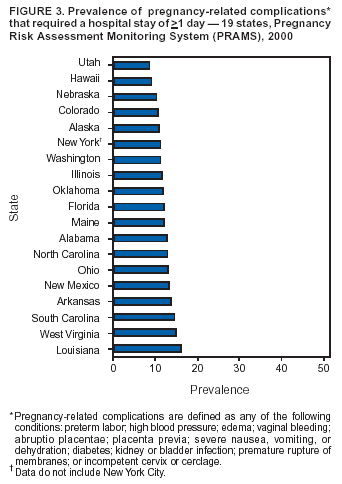
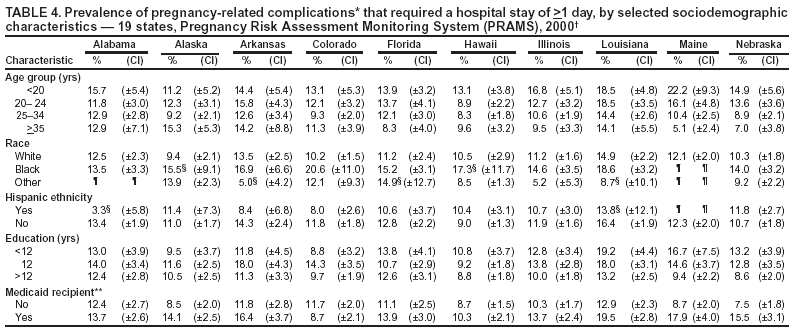
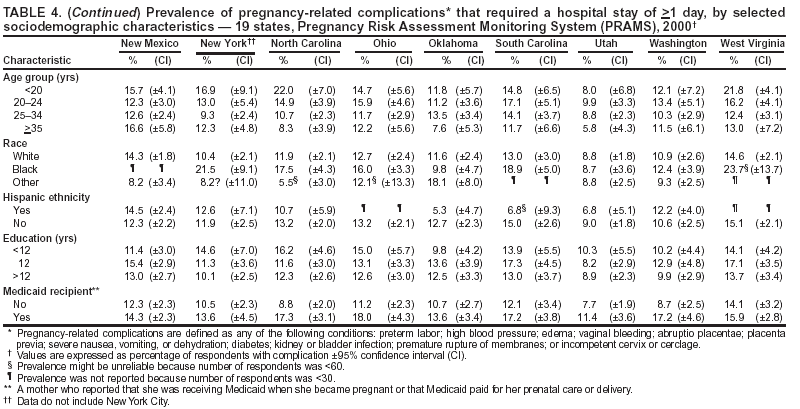
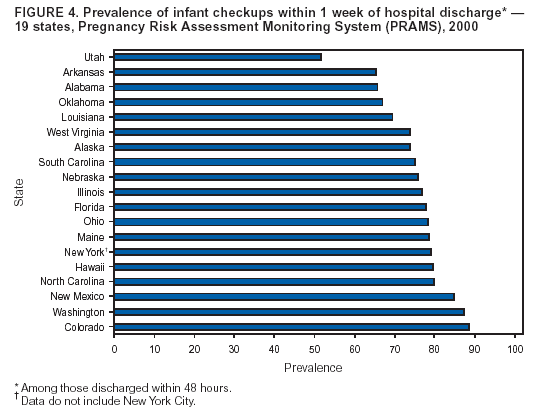
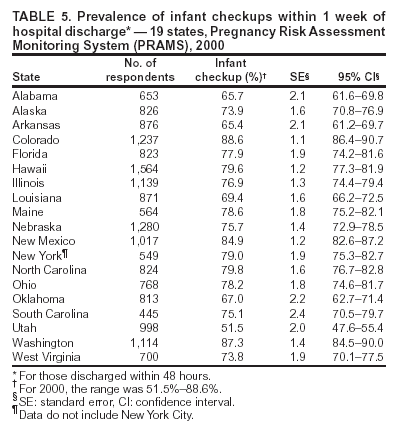
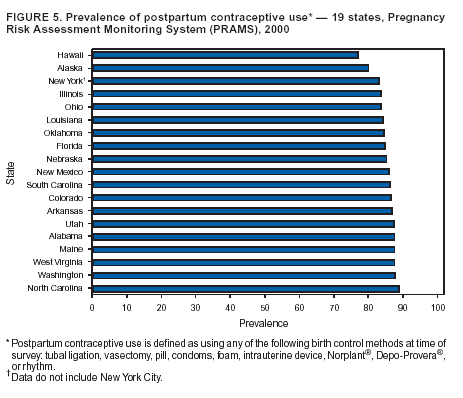
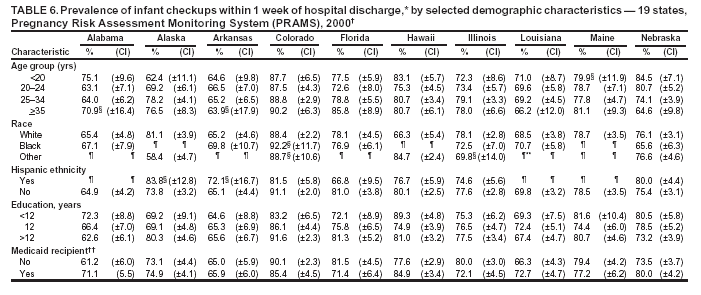
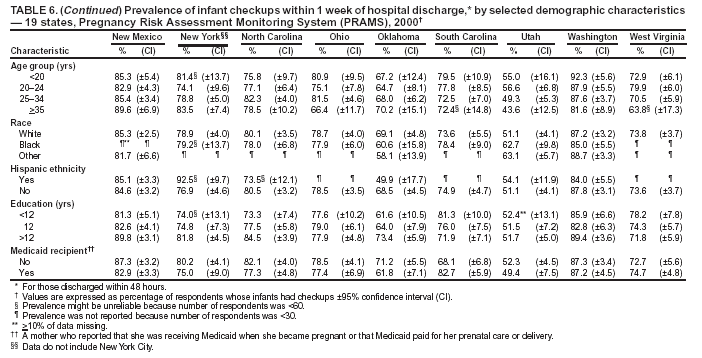
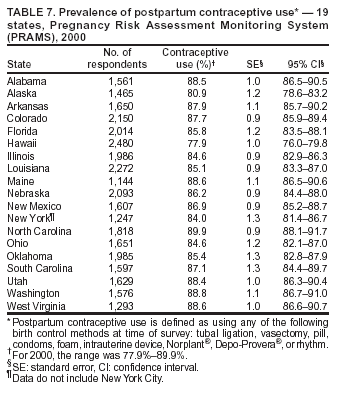
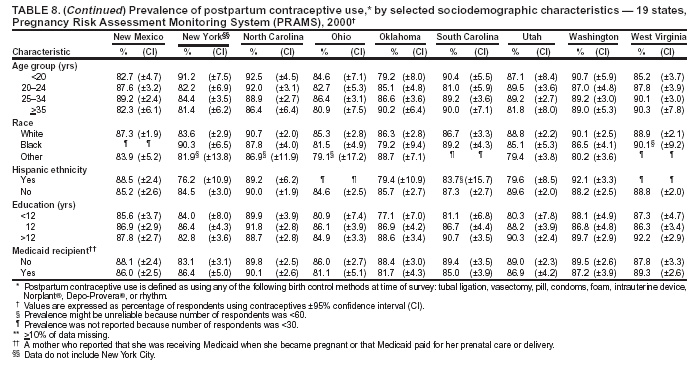
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail. Surveillance for Selected Maternal Behaviors and Experiences Before, During, and After PregnancyPregnancy Risk Assessment Monitoring System (PRAMS), 2000Letitia M. Williams, M.P.H.1 AbstractProblem/Condition: Various maternal behaviors and experiences are associated with adverse health outcomes for both the mother and the infant. These behaviors and experiences can occur before pregnancy (e.g., insufficient intake of folic acid), during pregnancy (e.g., complications requiring hospitalization, such as high blood pressure), and after pregnancy (e.g., inadequate follow-up of infants who were discharged early). Information regarding maternal behaviors and experiences is needed to monitor trends, to enhance the understanding of the relations between behaviors and health outcomes, to plan and evaluate programs, to direct policy decisions, and to monitor progress toward Healthy People 2010 objectives (US Department of Health and Human Services. Healthy People 2010. 2nd. ed. With understanding and improving health and objectives for improving health [2 vols.]. Washington DC: US Department of Health and Human Services, 2000). Reporting Period Covered: This report covers data for 2000. Description of System: The Pregnancy Risk Assessment Monitoring System (PRAMS) is an ongoing, state- and population-based surveillance system designed to monitor selected self-reported maternal behaviors and experiences that occur before, during, and after pregnancy among women who deliver a live-born infant in 31 states and New York City. PRAMS employs a mixed-mode data collection methodology; as many as three self-administered surveys are mailed to a sample of mothers, and nonresponders are followed up with a telephone interview. Self-reported survey data are linked to selected birth certificate data and weighted for sample design, nonresponse, and noncoverage to create annual PRAMS analysis data sets. PRAMS data can be used to produce statewide estimates of various perinatal health behaviors and experiences among women delivering a live infant. Four indicators for the year 2000 (multivitamin use, pregnancy-related complications, infant checkup, and postpartum contraceptive use) from 19 states are examined in this report. Results: In 2000, the prevalence of multivitamin use >4 times per week in the month before pregnancy ranged from 25.0% to 40.7% across the 19 states. Prevalence of pregnancy-related complications requiring hospitalization ranged from 8.8% to 16.3%. Prevalence of infant checkups within 1 week of early (<48 hours) hospital discharge ranged from 51.5% to 88.6%. Prevalence of postpartum contraceptive use ranged from 77.9% to 89.9%. Interpretation: PRAMS data indicate that 19 states are well below the Healthy People 2010 objective for folic acid consumption, as measured by multivitamin use. Data for infant checkups indicate that guidelines for care are not being followed for as many as half of those discharged early. However, data for additional years are needed to assess trends in these four indicators. Public Health Action: State maternal and child health programs can use these population-based data to monitor progress toward Healthy People 2010 objectives, evaluate adherence to guidelines for care, and assess changes in prevalence of other health behaviors. The data can be shared with policy makers to direct policy decisions that might affect the health of mothers and infants. By providing data on maternal behaviors and experiences that are associated with adverse outcomes, PRAMS supports the activities of two CDC initiatives---to promote safe motherhood and to reduce infant mortality and low birthweight. IntroductionVarious behaviors and experiences are associated with adverse health outcomes for both the mother and infant. These experiences can occur before, during, and after pregnancy. For example, insufficient folic acid consumption before conception and in early pregnancy can increase the incidence of neural tube defects (1). Severe complications during pregnancy contribute to maternal and infant morbidity and mortality (2). Because serious medical conditions, such as sepsis, congenital heart disease, and jaundice, become apparent 24--72 hours after birth, infants who are discharged early (<48 hours) from the hospital should receive a medical visit within 1 week of discharge (3--5). Postpartum contraceptive use is a key factor in spacing births for maximum health benefits. The Pregnancy Risk Assessment Monitoring System (PRAMS) was initiated in 1987 and is administered by CDC's National Center for Chronic Disease Prevention and Health Promotion, Division of Reproductive Health, in collaboration with state health departments. PRAMS is an ongoing, state- and population-based surveillance system designed to monitor selected self-reported maternal behaviors and experiences that occur before, during, and after pregnancy among women who deliver a live-born infant. The PRAMS questionnaire is revised periodically to reflect changing priorities and emerging issues. Each revision is referred to as a phase. The data highlighted in this report were collected with the Phase Four version of the questionnaire, which was implemented with the 2000 birth cohort. The four topics presented in this report represent three new indicators and one revised indicator from the PRAMS survey. The new indicators are multivitamin use, infant checkups within 1 week of hospital discharge among those discharged within 48 hours, and postpartum contraceptive use. The revised indicator is pregnancy-related complications requiring hospitalization. Prevalence estimates are presented by state and by selected demographic characteristics (age, race, Hispanic ethnicity, education, and Medicaid status). Annual reports that highlight key PRAMS findings from previous years are also available (6--11). The data presented in this report can be used to assist in program planning and evaluation, to inform policy decisions, and to monitor progress toward Healthy People 2010 objectives (12). By providing data concerning maternal behaviors and experiences that are associated with adverse outcomes, PRAMS supports the activities of two CDC initiatives --- to promote safe motherhood and to reduce infant mortality and low birthweight. MethodsProject DescriptionPRAMS was originally implemented in 1987 to help state health departments establish and maintain an epidemiologic surveillance system of selected maternal behaviors and experiences to supplement data from vital records. In the health departments, PRAMS program structures cross several existing organizational units, including maternal and child health and vital statistics. Since its inception, the program has expanded from six to 32 participating health departments in 2003. This number includes 29 states and one city (New York City) that conduct the traditional PRAMS surveillance and two states that recently completed a point-in-time survey. One state conducts the traditional PRAMS surveillance as well as additional PRAMS activities. Live births in these states and city represent approximately 62% of all live births in the United States. Data CollectionAll participating states use a standardized data collection method developed by CDC. Every month, a stratified sample of 100--300 new mothers is selected from eligible birth certificates in each state. PRAMS employs a mixed-mode data collection methodology; as many as three self-administered surveys are mailed to mothers in the sample, and nonresponders are followed up with a telephone interview. The first survey is typically mailed 2--3 months after delivery to allow for collection of information about postpartum maternal and infant experiences. Self-reported survey data are linked to selected birth certificate data and weighted for sample design, nonresponse, and noncoverage to create the PRAMS analysis data sets. Additional details regarding the PRAMS methodology have been described elsewhere (13). Validity of specific questions is addressed through pretesting. New questions are tested through cognitive interviewing, in which respondents are asked to describe their understanding of the question's meaning and how they arrived at their response. On the basis of the results of the cognitive testing, questions are revised. A second round of testing involves administering the questionnaire to respondents, who are asked to complete it and provide written feedback. Before the next revision cycle, questions are evaluated for item nonresponse, write-in responses, and whether respondents correctly followed skip patterns. Questions that fare poorly in these evaluations are revised accordingly and pretested before being included in the questionnaire. Data AnalysisThis report includes data from 19 states (Alabama, Alaska, Arkansas, Colorado, Florida, Hawaii, Illinois, Louisiana, Maine, Nebraska, New Mexico, New York, North Carolina, Ohio, Oklahoma, South Carolina, Utah, Washington, West Virginia) (Figure 1) that collected data on year 2000 births and achieved weighted response rates of at least 70%. The weighted response rate indicates the proportion of women sampled who completed a survey, adjusted for sample design. For one reporting area, data are not representative of the entire state: New York data are for upstate New York only and exclude New York City, which has an autonomous vital records agency. Each state's stratification variables, annual sample size, and weighted response rate (range: 72%--86%) are listed (Appendix). Data are presented for four maternal behaviors and experiences that were self-reported on the survey. To assess folic acid consumption, multivitamin use (i.e., taking a multivitamin four or more times per week during the month before pregnancy) was measured. Most commonly available multivitamins contain 400 µg of folic acid, the recommended daily dose for women of childbearing age. Pregnancy-related complications were defined as having stayed in the hospital for >1 day for any of the following conditions: preterm labor; high blood pressure; edema; vaginal bleeding; abruptio placentae; placenta previa; severe nausea, vomiting, or dehydration; diabetes; kidney or bladder infection; premature rupture of membranes; or incompetent cervix or cerclage. The definition of these pregnancy complications might include the delivery hospitalization if the medical complication occurred at the time of delivery. Infant checkup was defined as a visit to or by a medical doctor or nurse within 1 week of hospital discharge. This indicator is reported only for infants who were discharged within 48 hours of delivery. Postpartum contraceptive use was defined as using any of the following birth control methods 2--8 months postpartum at the time of the survey: tubal ligation (tubes tied), vasectomy, pill, condoms, foam, intrauterine device, Norplant®, Depo-Provera®, or rhythm method. The 2000 prevalence estimates are presented by state with associated standard errors and 95% confidence intervals (CI). Graphs accompany the tables. Prevalence estimates for 2000 also are presented by maternal sociodemographic characteristic and state. The sociodemographic characteristics of age, race, Hispanic ethnicity, and education were taken from the birth certificate. Maternal age was grouped into four categories (<20 years, 20--24 years, 25--34 years, >35 years). Race was grouped into three categories (white, black, other). In Alaska, the other race category comprised primarily Alaska Natives. In New Mexico and Oklahoma, the other race category comprised primarily Native Americans. In the remaining 16 states, the other race category was composed primarily of Asians. Ethnicity was defined as Hispanic or not Hispanic. Education was grouped into three categories (less than high school, high school, more than high school). Medicaid status was self-reported on the survey. A Medicaid recipient was defined as someone who was receiving Medicaid just before the pregnancy or who used Medicaid to pay for prenatal care or delivery. All tables in the report were produced by using weighted PRAMS data. Percentages and standard errors were calculated for the characteristic of interest by using PROC CROSSTAB in SUDAAN (14). The 95% confidence intervals were computed by using the formula CI = percentage ± (1.96 ´ standard error). The number of respondents was the number of mothers who answered a particular question. All missing observations were excluded. An estimate is noted in the tables when the percentage of missing values is >10%. Because estimates based on small samples are imprecise and might be biased, estimates for which the number of respondents was <60 are noted in the tables that present data by sociodemographic characteristic. Estimates for which the number of respondents was <30 are not reported. The chi square test was used to identify statistically significant associations between sociodemographic variables and the indicators for each state. For age and education, logistic regression was performed in addition to the chi square test to assess linear relationships with each indicator. In cases in which the chi-square test indicated a significant association for race, an additional chi-square test was performed with race collapsed into two categories (black and white/other). ResultsMultivitamin UseIn 2000, 25.0%--40.7% of women reported taking a multivitamin >4 times per week in the month before pregnancy (Table 1). The prevalence was lowest in Oklahoma and West Virginia and was highest in Maine (Figure 2). In all 19 states, prevalence of multivitamin use increased with increasing maternal age (Table 2). In 14 states, an association was noted between race and the prevalence of multivitamin use (Table 2). In 11 of these states (Alabama, Illinois, Louisiana, Nebraska, New York, North Carolina, Ohio, Oklahoma, Utah, Washington, West Virginia), black women were significantly less likely to report multivitamin use than were women in the white/other category. In 10 of the 16 states where adequate data regarding Hispanic populations were available (Arkansas, Colorado, Hawaii, Illinois, Nebraska, New Mexico, New York, North Carolina, Utah, Washington), non-Hispanic women were more likely than Hispanic women to report multivitamin use. In all states, women with >12 years of education were significantly more likely than women with <12 years to use multivitamins (Table 2). In all states, women receiving Medicaid were significantly less likely than those not receiving Medicaid to report multivitamin use. Pregnancy-Related ComplicationsIn 2000, the prevalence of pregnancy-related complications that required a hospital stay of >1 day ranged from 8.8% to 16.3% across 19 states (Table 3). The prevalence was lowest in Utah and highest in Louisiana (Figure 3). When examined by age group, the prevalence of pregnancy-related complications was significantly higher among younger women than older women in four states (Maine, Nebraska, North Carolina, and West Virginia) (Table 4). Associations between race and pregnancy-related complications were found in six states (Alaska, Arkansas, Illinois, New Mexico, North Carolina, and South Carolina). In two states (North Carolina and South Carolina), black women had a significantly higher prevalence of pregnancy-related complications than women in the white/other race category. Prevalence of pregnancy-related complications was lower among Hispanic women than non-Hispanic women in three (Alabama, Colorado, and Oklahoma) of the 16 states where data were available for Hispanic populations. In three states (Louisiana, Maine, and Nebraska), the prevalence of pregnancy-related complications declined with increasing maternal education (Table 4). In eight of 19 states (Alaska, Illinois, Louisiana, Maine, Nebraska, North Carolina, Ohio, Washington), Medicaid recipients were more likely than women who did not receive Medicaid to have pregnancy-related complications. Infant CheckupIn 2000, the prevalence of infant checkups within 1 week after hospital stay of <48 hours ranged from 51.5% to 88.6% in 19 states (Table 5). The lowest and highest prevalences were in Utah and Colorado, respectively (Figure 4). Significant differences in prevalence of infant checkups by age, race, and ethnicity were seen infrequently. In only two of 19 states (Alaska and Nebraska) was infant checkup associated with maternal age. The direction of the association differed in these two states (Table 6). In four states (Alaska, Hawaii, Nebraska, and Utah), race was significantly associated with infant checkups. In Nebraska, black women had a significantly lower prevalence of infant checkup than women in the white/other race category. However, in Utah, black women were more likely to report infant checkups than were women in the white/other race category (Table 6). Differences in the prevalence of infant checkup differed by Hispanic ethnicity in three states (Colorado, Florida, and New York). In Colorado and Florida, Hispanic women were less likely than non-Hispanic women to report infant checkup. In New York, Hispanic women had a higher prevalence of infant checkups than did non-Hispanic women. In four states (Alaska, Colorado, New Mexico, and North Carolina), the prevalence of infant checkups increased with increasing maternal education (Table 6). In eight states (Alabama, Florida, Hawaii, Illinois, Louisiana, Nebraska, Oklahoma, South Carolina), infant checkup was associated with Medicaid status, although the direction of association differed across states. Postpartum Contraceptive UseIn 2000, the prevalence of postpartum contraceptive use among women in 19 states who delivered a live infant ranged from 77.9% to 89.9% (Table 7). Prevalence was lowest in Hawaii and highest in North Carolina (Figure 5). Use of postpartum contraception decreased significantly with age in only one state, Hawaii (Table 8). In five states (Alaska, Hawaii, Nebraska, Utah, and Washington), postpartum contraceptive use was associated with race (Table 8). In only one state (Alaska), black women were significantly more likely to report postpartum contraceptive use than were women in the white/other race category. Hispanic women in Hawaii were significantly more likely than non-Hispanic women to report postpartum birth control use (Table 8). In Utah, Hispanic women were significantly less likely than non-Hispanic women to report postpartum birth control use. Postpartum contraceptive use increased with increasing maternal education in six states (Arkansas, Louisiana, Nebraska, Oklahoma, South Carolina, and West Virginia). Postpartum contraceptive use was associated with Medicaid status in three states (Arkansas, Louisiana, and Oklahoma). Medicaid recipients were less likely than women who did not receive Medicaid to report postpartum contraceptive use (Table 8). DiscussionPrevalence of the four indicators examined in this report varied among particular subpopulations of women. State-to-state variations also were seen in the prevalence of these indicators. Variations across states may be attributable to population differences in sociodemographic characteristics, differences in state and local policies, and variations in the availability of and access to health-care services. Multivitamin UseIncreased folic acid consumption before conception and in early pregnancy reduces the incidence of neural tube defects and can also reduce the incidence of certain congenital heart defects (1,15--16). Congenital anomalies are the leading cause of infant death, causing 5,743 deaths, or 20.5% of all infant deaths, in 2000 (17). Neural tube defects alone caused 419 deaths (17). In 1992, the U.S. Public Health Service recommended that all women of childbearing age consume 400 µg of folic acid daily (18). In 1998, the Food and Drug Administration required enriched cereal grain products to be fortified with folic acid. The Healthy People 2010 goal is for 80% of nonpregnant women aged 15--44 years to consume at least 400 µg of folic acid each day from fortified foods or dietary supplements (12). Most commonly available multivitamins contain 400 µg of folic acid. In 2000, PRAMS began asking women if they took a multivitamin in the month before they became pregnant. However, PRAMS does not capture folic acid consumption through other means (e.g., fortified foods). Knowledge of these recommendations and of the benefits of folic acid consumption has spread slowly among childbearing women. In 2002, a March of Dimes national survey found that 75% of women had heard of folic acid, and 14% knew that folic acid helps prevent birth defects, but only 34% of women took a vitamin supplement containing folic acid (19). PRAMS data (25.0%--40.7% of women taking multivitamins) are consistent with the March of Dimes findings. PRAMS data indicate that the Healthy People 2010 objective for folic acid consumption, as measured by multivitamin use, is not being met in these states. State health departments can use these data to target campaigns promoting multivitamin use to populations in which folic acid consumption is lower than recommended (e.g., younger women, those with less education, and Medicaid recipients). States can also use PRAMS data as a benchmark for tracking progress toward the Healthy People 2010 goal. Pregnancy-Related ComplicationsPregnancy-related complications contribute to maternal, fetal, and infant mortality and morbidity (2,20). These severe complications continue to be a priority area for Healthy People 2010, which includes objectives that address reducing maternal complications during pregnancy (12). Hospitalization rates for pregnancy-related complications have been the primary means for measuring maternal morbidity (21). Monitoring of severe pregnancy-related complications is crucial in assessing maternal morbidity and mortality. Infant CheckupLength of hospital stay after childbirth has decreased dramatically in the last 30 years because of social and financial factors (3--4,22). Since the early 1990s, ongoing debate has occurred regarding the safety of early hospital discharge of mothers and newborns. In the mid-1990s, concern about harm to newborns as a result of early postpartum hospital discharge resulted in laws to establish minimum hospital stay of 48 hours after a vaginal delivery (22). Guidelines of the American Academy of Pediatrics (AAP) and American College of Obstetrics and Gynecology (ACOG) recommend at least 48 hours of postpartum hospitalization (23,24). AAP, ACOG, and other national and international authorities also recommend that newborns are followed up within the first week of birth in cases of early hospital discharge (3,22). Numerous serious medical conditions become apparent 24--72 hours after birth. These include sepsis, congenital heart disease, jaundice, and other problems that may require evaluation and treatment (4,22). Although certain studies demonstrate reductions in hospital and patient costs, improvement in patient satisfaction, and promotion of family bonding when mothers and newborns are discharged earlier (4,22,25), the majority of studies conclude that early hospital discharge can lead to problems if appropriate follow-up is not performed (4,5,22). In 2000, PRAMS began collecting infant follow-up data, which complement the infant early discharge data collected in previous years. These data indicate that as a woman's education increased, so did the likelihood of having her infant followed up within 1 week after being discharged within 48 hours of delivery. PRAMS data can be useful for assessing the proportion of newborns receiving follow-up in the first week after early discharge. This information can be used to conservatively monitor the level of adherence to the AAP and ACOG guidelines, which recommend follow-up within 48 hours after discharge. Postpartum Contraceptive UseInfants born to women who became pregnant 18--59 months after a prior birth have been found to be at lower risk of dying, being born preterm, being small for gestational age, or having low birthweight compared with infants born following an interpregnancy interval of <6 months or >59 months (26--30). Postpartum contraceptive use is critical in preventing pregnancy shortly after childbirth. Studies that have examined the efficacy and appropriateness of various contraceptive methods during the postpartum period have indicated that certain hormonal methods can affect breastfeeding by reducing the production of milk, and other methods should not be initiated until 4--8 weeks after delivery (31). However, safe and effective methods that can be used shortly after delivery have been identified. Recent research has indicated that Depo-Provera® injections are effective in preventing repeat pregnancies among postpartum adolescents (32--34). Other appropriate postpartum methods include vaginal rings, progestin-only pills and Copper T 380-A intrauterine devices (35). PRAMS collects data regarding prevalence of contraceptive use following the birth of a live infant and reasons for not using contraception during the postpartum period (not reported here). Selected states also capture the type of contraceptives that a woman is using. These data can be helpful in informing policy and programs that are working toward the Healthy People 2010 objective of reducing the number of births occurring within 24 months of a previous birth from the baseline measure of 11% to the target of 6%. LimitationsSeveral limitations affect the data presented in this report. Because data are self-reported 2--8 months after delivery, responses might be subject to recall bias, particularly for behaviors and experiences that occurred before the pregnancy (e.g., folic acid consumption). Recall may also differ for the subset of women who experienced pregnancy complications or whose infants experienced health problems. PRAMS provides population-based data for each participating state; results are not generalizable to other states or to the United States as a whole. The associations between the indicators and age, race, ethnicity, education, and Medicaid status could all be a function of socioeconomic status. No controlling for confounding factors was done in this analysis, and additional research is needed to assess the effects of these factors when controlling for socioeconomic status. Finally, the associations between a specific indicator and demographic characteristic do not imply causality. ConclusionThe health of mothers and their infants is affected by behaviors and experiences that occur before, during, and after pregnancy. This is the first report from PRAMS covering four indicators designed to capture these time periods. Certain sociodemographic groups of women (e.g., black women) were less likely to engage in protective behaviors such as multivitamin use, getting a postnatal checkup for their newborn infant, and postpartum contraceptive use. Pregnancy-related complications were experienced by different groups of women in different states. These data can be used to tailor the development of state-based programs, such as education initiatives and services for women at highest risk in each state. A distinct feature of PRAMS is that it allows states to obtain population-based estimates to support their maternal and child health programs. In the past, states have used data from PRAMS to generate legislative support for maternal and child health programs. Legislature appropriation for unintended pregnancy, a 5-year funded state-wide smoking cessation campaign, and increased domestic violence screening for pregnant women are just a few examples of how states interpret and use PRAMS data (36). By obtaining more years of data on the indicators in this report and by continuing monitoring of the prevalence and sociodemographic characteristics of women reporting these behaviors and experiences, states can help clarify patterns and direct appropriate prevention strategies. Acknowledgments The PRAMS Working Group: Alabama: Rhonda Stephens, M.P.H.; Alaska: Kathy Perham-Hester, M.P.H.; Arkansas: Gina Redford, M.A.P.; Colorado: Alyson Shupe, Ph.D.; Florida: Steven Wiersma, M.D.; Georgia: Tonya Johnson; Hawaii: Limin Song, M.P.H.; Illinois: Theresa Sandidge, M.A.; Louisiana: Joan Wightkin; Maine: Martha Henson; Maryland: Diana Cheng, M.D.; Michigan: Yasmina Bouraoui, M.P.H.; Minnesota: Ron Campbell, M.D.; Mississippi: Linda Pendleton, L.M.S.W.; Montana: JoAnn Dotson; Dr. P.H.; Nebraska: Debbi Barnes-Josiah, Ph.D.; New Jersey: Lakota Kruse, M.D.; New Mexico: Ssu Weng, M.D.; New York State: Anne Radigan-Garcia; New York City: Fabienne Laraque, M.D.; North Carolina: Paul Buescher, Ph.D.; North Dakota: Sandra Anseth, R.N.; Ohio: Adriana Pust; Oklahoma: Dick Lorenz, M.S.; Oregon: Ken Rosenberg, M.D.; Rhode Island: Sam Viner-Brown; South Carolina: Mary Kate Powell; Texas: Ramdas Menon, Ph.D.; Utah: Lois Bloebaum; Vermont: Peggy Brozicevic; Washington: Linda Lohdefinck; West Virginia: Melissa Baker, M.A.; CDC PRAMS Team, Applied Sciences Branch, Division of Reproductive Health, National Center for Chronic Disease Prevention and Health Promotion. References
|
Use of trade names and commercial sources is for identification only and does not imply endorsement by the U.S. Department of
Health and Human Services. |
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices.
Page converted: 11/3/2003
|
|
|||||
|
HOME |
ABOUT MMWR |
MMWR SEARCH |
DOWNLOADS |
RSS
|
CONTACT
|
|||||
|
|
|||||
|
This page last reviewed 11/3/2003