 |
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail. Assisted Reproductive Technology Surveillance --- United States, 2001Victoria Clay Wright, M.P.H.1 AbstractProblem/Condition: In 1996, CDC initiated data collection regarding assisted reproductive technology (ART) procedures performed in the United States to determine medical center-specific pregnancy success rates, as mandated by the Fertility Clinic Success Rate and Certification Act (FCSRCA) (Public Law 102-493, October 24, 1992). ART includes fertility treatments in which both eggs and sperm are handled in the laboratory (i.e., in vitro fertilization and related procedures). Patients who undergo ART treatments are more likely to deliver multiple-birth infants than women who conceive naturally. Multiple births are associated with increased risk for mothers and infants (e.g., pregnancy complications, premature delivery, low-birthweight infants, and long-term disability among infants). Reporting Period Covered: 2001. Description of System: CDC contracts with a professional society, the Society for Assisted Reproductive Technology (SART), to obtain data from fertility medical centers located in the United States. Since 1997, CDC has compiled data related to ART procedures. The Assisted Reproductive Technology Surveillance System was initiated by CDC in collaboration with the American Society for Reproductive Medicine, the Society for Assisted Reproductive Technology, and RESOLVE: The National Infertility Association. Results: In 2001, a total of 29,344 live-birth deliveries and 40,687 infants resulting from 107,587 ART procedures were reported from 384 medical centers in the United States and U.S. territories. Nationally, 80,864 (75%) of ART treatments used freshly fertilized embryos from the patient's eggs; 14,705 (14%) used thawed embryos from the patient's eggs; 8,592 (8%) used freshly fertilized embryos from donor eggs; and 3,426 (3%) used thawed embryos from donor eggs. Overall, 40% of ART procedures that progressed to the transfer stage resulted in a pregnancy; 33% resulted in a live-birth delivery (delivery of >1 infant); and 21% resulted in a singleton live birth. The highest live-birth rates were observed among ART procedures using freshly fertilized embryos from donor eggs (47%). The greatest numbers of ART procedures were performed among residents of California (13,124), New York (12,379), Massachusetts (8,151), Illinois (7,933), and New Jersey (6,011). These five states also reported the highest number of live-birth deliveries and infants born as a result of ART. The ratio of number of ART procedures per million population ranged from 74 in Idaho to 1,273 in Massachusetts, with a national average of 371 ART procedures started per million persons. Among ART treatments in which freshly fertilized embryos from the patient's eggs were used, substantial variation in live birth rates by patient (e.g., women aged <40 years) and treatment characteristics (e.g., ovulatory dysfunction, endometriosis, or unexplained infertility) was observed. The risk for a multiple-birth delivery was highest for women who underwent ART transfer procedures using freshly fertilized embryos from either donor eggs (42%) or from their own eggs (36%). Among ART transfer procedures in which the patient's own eggs were used, an inverse relation existed between multiple-birth risk and patient age. Number of embryos transferred and embryo availability (an indicator of embryo quality) were also strong predictors of multiple-birth risk. Of the 40,687 infants born, 46% were twins, and 8% were triplet and higher order multiples. The total multiple-infant birth rate was 53%. Approximately 1% of U.S. infants born in 2001 were conceived through ART. Those infants accounted for 16% of multiple births nationally. Interpretation: Whether an ART procedure resulted in a pregnancy and live-birth delivery varied according to different patient and treatment factors. ART poses a major risk for multiple births. This risk varied according to the patient's age, the type of ART procedure performed, the number of embryos transferred, and embryo availability (an indicator of embryo quality). Public Health Actions: ART-related multiple births represent a sizable proportion of all multiple births nationally and in selected states. Efforts should be made to limit the number of embryos transferred for patients undergoing ART. IntroductionFor >2 decades, assisted reproductive technologies (ARTs) have been used by couples to overcome infertility. ARTs include those infertility treatments in which both eggs and sperm are handled in the laboratory (i.e., in vitro fertilization and related procedures). Since the birth of the first U.S. infant conceived with ART in 1981, use of these treatments has increased dramatically. Each year, both the number of medical centers providing ART services and the total number of procedures performed have increased notably (1). In 1992, Congress passed the Fertility Clinic Success Rate and Certification Act (FCSRCA),* which requires each medical center in the United States that performs ART to report data to CDC annually on every ART procedure initiated. CDC uses the data to report medical center-specific pregnancy success rates. In 1997, CDC published the first surveillance report under this mandate (2). That report was based on ART procedures performed in 1995. Since then, CDC has continued to publish a surveillance report annually that details each medical center's success rates. CDC has also used this surveillance data file to perform more in-depth analyses of infant outcomes (e.g., multiple births) (3,4). Multiple-infant births are associated with greater health problems for both mothers and infants, including higher rates of caesarean deliveries, prematurity, low birthweight, and infant death and disability. This report is based on ART surveillance data provided to CDC's National Center for Chronic Disease Prevention and Health Promotion (NCCDPHP), Division of Reproductive Health, regarding procedures performed in 2001. A report of these data according to the medical center in which the procedure was performed was published separately (1). In this report, emphasis is on presenting state-specific data and presenting more detailed data regarding multiple-birth risk for 2001. MethodsEach year, the Society for Assisted Reproductive Technology (SART), an organization of ART providers affiliated with the American Society for Reproductive Medicine, collects data regarding ART procedures from medical centers performing ART in the United States and its territories and provides these data to CDC by contract. Data collected include patient demographics, medical history and infertility diagnoses, clinical information pertaining to the ART procedure, and information regarding resultant pregnancies and births. The data file is organized with one record per ART procedure performed. Multiple procedures from a single patient are not linked. Despite the federal mandate, certain centers (<10%/year) have not reported their data; the majority of these are believed to be smaller-than-average practices. For this report, data pertaining to ART procedures initiated January 1--December 31, 2001, are presented. ART data and outcomes from ART procedures are presented by patient's state of residence at time of ART treatment. In cases of missing residency data (<9%), the state of residency was assigned as the state in which the ART procedure was performed. In addition, data regarding the number of ART procedures in relation to the total population for each state are indicated.† Data regarding number of procedures are also presented by treatment type and stage of treatment. ART procedures are usually classified into four groups according to whether a woman used her own eggs or received eggs from a donor and whether or not the embryos transferred were freshly fertilized or previously frozen and thawed. Because both success rates and multiple-birth risk vary substantially among these four treatments groups, data are presented separately for each type. In addition to treatment types, within a given treatment procedure, different stages exist. A typical ART procedure begins when a woman starts taking drugs to stimulate egg production or begins having her ovaries monitored with the intent of having embryos transferred. If eggs are produced, the procedure progresses to the egg-retrieval stage. After the eggs are retrieved, they are combined with sperm in the laboratory, and if fertilization is successful, the resulting embryos are selected for transfer. If the embryo implants in the uterus, the cycle progresses to a clinical pregnancy (i.e., the presence of a gestational sac detectable by ultrasound). The resulting pregnancy might progress to a live-birth delivery. A live-birth delivery is defined as the delivery of >1 live-born infant. Only ART procedures involving freshly fertilized eggs include an egg-retrieval stage; ART procedures using thawed eggs do not include egg retrieval because eggs were fertilized during a previous procedure and the resulting embryos were frozen until the current procedure. An ART procedure can be discontinued at any step for medical reasons or by the patient's choice. Variations in a typical ART procedure are noteworthy. Although a typical ART procedure includes in vitro fertilization (IVF) of gametes, culture for >2 days and embryo transfer into the uterus (i.e., transcervical embryo transfer), in certain cases, unfertilized gametes (eggs and sperm) or zygotes (early embryos [i.e., a cell that results from fertilization of the egg by a sperm]) are transferred into the fallopian tubes within a day or two of retrieval. These are known as gamete and zygote intrafallopian transfer (GIFT and ZIFT). Another adaptation is intracytoplasmic sperm injection (ICSI) in which fertilization is still in vitro but is accomplished by selection of a single sperm that is injected directly into the egg. This technique was originally developed for couples with male factor infertility but is now commonly used for an array of diagnostic groups. Data are presented for each of the four treatment types: freshly fertilized embryos from the patient's eggs, freshly fertilized embryos from donor eggs, thawed embryos from the patient's eggs, and thawed embryos from donor eggs. Detailed data are additionally presented in this report for the most common treatment type, those using freshly fertilized embryos from the patient's eggs. These procedures account for >70% of the total number of ART procedures performed each year. For those procedures that progressed to the embryo-transfer stage, percentage distribution of selected patient and treatment factors were calculated. In addition, success rates, defined as live-birth deliveries per ART-transfer procedure, were calculated according to the same patient and treatment characteristics. Patient factors included the age of the woman undergoing ART, whether she had previously given birth, the number of past ART attempts, and the infertility diagnosis of both the female and male partners. The patient's age at the time of the ART procedure were grouped into five categories: aged <35 years, 35--37 years, 38--40 years, 41--42 years, and >42 years. Diagnoses ranged from one factor in one partner to multiple factors in one or both partners and were categorized as
Treatment factors included
The number of embryos transferred in an ART procedure was categorized as 1, 2, 3, 4, or >5. The number of days of embryo culture was calculated by using dates of egg retrieval and embryo transfer and was categorized as 1--6. However, because of limited sample sizes, live-birth rates are presented only for the two most common days, 3 and 5. For the same reason, live-birth rates are presented for IVF with and without ICSI and not for GIFT and ZIFT. ICSI was subdivided as to whether it was used among couples diagnosed with male factor (the original indication for ICSI treatment) or couples not diagnosed with male factor. Chi-square tests were run separately to evaluate differences in live-birth rates by select patient and treatment factors within each age group. Multivariable logistic regression was also performed to evaluate the independent effects of patient factors --- diagnosis, number of prior ART procedures, and number of previous births --- on chance to have a live birth as a result of an ART treatment. Because age is known to be a strong predictor for live birth, separate models were constructed for each of the five age groups such that these models provide an indication of the variability in live births based on patient factors within each age strata. For these analyses, the referent groups included patients with a tubal factor diagnosis, no previous ART procedures, and no previous births. Multivariable models did not include treatment factors because of multicolinearity between certain treatment factors and multiple potential effect modifications. Rather, detailed stratified analyses were performed to elucidate additional detail related to associations between different treatment factors and live birth. In addition to presenting live-birth rates as a measure of success, success rates based on singleton live births according to treatment group and patient age are also presented. Singleton live births are a key measure of ART success because they have a much lower risk than multiple-infant births for adverse health outcomes, including prematurity, low birthweight, disability, and death. Multiple birth as a separate outcome measure was also assessed. Multiple birth was assessed in two ways. First, each multiple-birth delivery was defined as a single event. A multiple-birth delivery was defined as the delivery of >2 infants in which at least one was live-born. The multiple-birth risk was thus calculated as the proportion of multiple-birth deliveries among total live-birth deliveries. Multiple birth was also assessed according to the proportion of infants from multiple deliveries among total infants (i.e., each infant was considered separately in this calculation). The proportion of live-born infants who were multiples (twins and triplets or more) was then calculated.§ Each of these measures represents a different focus. The multiple-birth risk, based on number of deliveries (or infant sets), provides an estimate of the individual risk posed by ART to the woman for multiple birth. The proportion of infants born in a multiple-birth delivery provides a measure of the effect of ART treatments on children in the population. Both measures are presented by type of ART treatment and by maternal age for births conceived with the patient's eggs. Multiple-birth risk is further presented by number of embryos transferred and whether additional embryos were available and cryopreserved for future use. Embryo availability (an indicator of embryo quality) has been demonstrated to have added predictive value independent of the number of embryos transferred (3,5). Proportion of infants born in a multiple-birth delivery is presented separately by patient's state of residency at time of ART treatment. To assess the impact of ART on total births in the United States in 2001, additional analyses including all ART infants born in 2001 are presented. Because the goal of the analysis was to assess the effect of ART on the 2001 U.S. birth cohort and the Assisted Reproductive Technology Surveillance System is organized according to the date of the ART procedure rather than the infant's date of birth, a separate ART data file was created for these analyses. This data file was drawn from two different ART reporting years and was composed of 1) infants conceived from ART procedures performed in 2000 and born in 2001 (approximately 2/3 of live-birth deliveries reported to the ART Surveillance System for 2000); and 2) infants conceived from ART procedures performed in 2001 and born in 2001 (approximately 1/3 of live-birth deliveries reported to the ART Surveillance System for 2001). Data regarding the total number of live births and multiple births in the United States in 2001 were obtained from birth certificate data (U.S. natality files) from CDC's National Center for Heath Statistics (6). These data represent 100% of births registered in the United States in 2001. Data are presented in relation to the total number of infants born in the United States in 2001 by plurality of births. All analyses were performed by using the SAS® software system (7). ResultsOf 421 medical centers in the United States and surrounding territories that performed ART in 2001, a total of 384 (91%) provided data to CDC (Figure 1). The majority of medical centers that provided ART services were located in the eastern United States, in or near major cities. Within states, the number of medical centers performing ART was variable. States with the largest number of ART centers that reported data in 2001 were California (56), New York (29), Florida (28), Texas (25), and Illinois (23). Four states had no ART medical centers (Alaska, Maine, Montana, and Wyoming). Success of ARTA total of 107,587 ART procedures performed in 2001 were reported to CDC (Table 1). The largest number of ART procedures occurred among patients who used their own freshly fertilized embryos (80,864; 75%). Of the 107,587 procedures started, 89,239 (83%) progressed to embryo transfer. Overall, 40% of ART procedures that progressed to the transfer stage resulted in a pregnancy; 33% resulted in a live-birth delivery; and 21% resulted in a singleton live birth. Pregnancy rates, live-birth rates, and singleton live-birth rates varied according to type of ART. The highest success rates were observed among ART procedures using donor eggs and freshly fertilized embryos (56% pregnancy rate, 47% live-birth rate, and 27% singleton live-birth rate). The lowest rates were observed among procedures using the patient's eggs and thawed embryos (29% pregnancy rate, 23% live-birth rate, and 17% singleton live-birth rate). In all, the 29,344 live-birth deliveries from ART procedures resulted in 40,687 infants (Table 1); the number of infants born was higher than the number of live-birth deliveries because of multiple-infant births. A total of 18,967 singleton infants were born as a result of ART. The largest proportion of infants born (75%; n = 30,383) were from ART procedures in which patients used freshly fertilized embryos from their own eggs. Number and Type of ART ProceduresThe number of ART procedures performed among residents of each state approximately paralleled the data by medical center location (Table 2). The greatest numbers of ART procedures reported in 2001 were performed among residents of California (13,124), New York (12,379), Massachusetts (8,151), Illinois (7,933), and New Jersey (6,011). The five states with the largest number of ART procedures performed also ranked highest in terms of numbers of live-birth deliveries and infants born. ART was used by residents of certain states and territories without an ART medical center (Alaska, Guam, Maine, Montana, Virgin Islands, and Wyoming); however, each accounted for a limited percentage of total ART usage in the United States. Non-U.S. residents accounted for <2% of ART procedures, live-birth deliveries, and infants born. The ratio of number of ART procedures per million population ranged from 74 in Idaho to 1,273 in Massachusetts, with a national average of 371 ART procedures started per million persons. Forty-seven percent of ART-transfer procedures using freshly fertilized embryos from the patient's eggs were performed on women aged <35 years; 22% on women aged 35--37 years; 19% on women aged 38--40 years; 8% on women aged 41--42 years; and 4% on women aged >42 years. Patient and treatment characteristics of these women varied by age (Table 3). The most common infertility diagnoses reported among couples in which the woman was aged <41 years were male factor and tubal factor; however, diagnoses varied overall. Tubal factor, male factor, and endometriosis were more commonly reported among younger women than women in older age categories. In contrast, diminished ovarian reserve was reported for only 1% of women aged <35 years; it was reported for 14% of women aged 41--42 years, and 20% of women aged >42 years. Among all women, 10%--13% were reported as having unexplained infertility; 10%--17% were reported as having multiple female factors; and 17%--21% were reported as having both male and female factors. Approximately 60% of women aged <35 years were undergoing their first ART procedure. The percentage of women who had undergone at least one previous ART procedure increased with age: only 41% of women aged >42 years were undergoing their first ART procedure. The percentage of women who had had a previous birth followed similar patterns. Although 20% of women aged <35 years reported at least one previous birth, this increased steadily with age: 36% of women in the oldest age group had had a previous birth.¶ The majority of ART procedures used IVF with or without ICSI. Less than 2% of ART procedures used GIFT or ZIFT. Although use of ICSI among couples diagnosed with male factor infertility declined with the patient's age, ICSI use among those not diagnosed with male factor infertility increased with patient's age. Despite variation among all age groups, the total proportion of ICSI use (i.e., combined ICSI for male factor and ICSI for other diagnoses) was greater than the proportion of in vitro fertilization with transcervical embryo transfer (IVF-ET) without ICSI. Among all age groups, the majority of procedures included embryo culture for 3 days; the next most common procedure involved embryo culture to day 5. Culture to day 5 coincides with development of the embryo to the blastocyst stage, which was used more frequently among younger women. Although limited variation existed by age, the majority of ART procedures involved transfer of >1 embryo. Among women aged <35 years, 96% of procedures involved transfer of >2 embryos, and 59% involved transfer of >3 embryos. For women aged >42 years, 87% involved transfer of >2 embryos, and 70% involved transfer of >3 embryos. The availability of extra embryos (an indicator of overall embryo quality) decreased with age. Extra embryos were available and cryopreserved for >40% of women aged <35 years, whereas only 5% of women aged >42 years had extra embryos available and cryopreserved (data were not available regarding extra embryos that were not cryopreserved for future use). Overall, 0.8% of ART transfer procedures used a gestational carrier or surrogate. Limited variation existed by patient age. Live Birth RatesLive-birth rates for women who underwent ART procedures using freshly fertilized embryos from their own eggs also varied by patient age and selected patient and treatment factors (Table 4). Although the average live-birth rate for ART-transfer procedures performed among women who used their own freshly fertilized eggs was 33%, live-birth rates ranged from 41% among women aged <35 years to 7% among women aged >42 years. Women aged <40 years who had an infertility diagnosis of ovulatory dysfunction, endometriosis, male factor, or had unexplained infertility tended to have higher live-birth rates. Women aged <40 years with an infertility diagnosis of diminished ovarian reserve or with multiple infertility diagnoses tended to have lower live-birth rates. Although women aged 41--42 years with a diagnosis of uterine factor appear to have had above average live-birth rates (21%), the variation in success rates across diagnostic categories was not statistically significant for this age group, nor for the oldest age group (women aged >42 years). Across all age groups, women who had undergone a previous ART procedure had lower live-birth rates than women undergoing their first ART procedure. However, the number of previous ART procedures cannot be subdivided by whether they were successful or not. Women in all age groups who had had >1 previous birth had higher live-birth rates than those with no previous births. However, the difference in live-birth rates for both the number of previous ART procedures and the number of previous births did not reach statistical significance for the two oldest age groups (women aged 41--42 years and women aged >42 years). Multivariable adjustment for patient factors within each age strata demonstrated similar patterns (Table 4) (data not indicated). Within all age groups, live-birth rates were higher among ART procedures that used IVF-ET without ICSI, in comparison to procedures that used ICSI, whether or not male factor was reported (Table 4). Live-birth rates were particularly low among couples who used ICSI in the absences of male factor infertility. Within all age groups, live-birth rates were increased among women who had extended embryo culture to day 5, transferred >2 embryos, and had extra embryos available and cryopreserved for future use. Variations in live-birth rates were statistically significant for all treatment factors within all age groups with the exception of number of days of embryo culture for women aged 41--42 years. Although live-birth rates also appeared to increase when a gestational carrier was used, these results reached statistical significance in only one age group (women aged 35--37 years). All of the results for treatment factors need to be considered cautiously because treatment was not randomized but rather based on medical center assessment and patient choice. Although variability among patients who used different treatment options cannot be adjusted for completely, stratified analyses were used to examine associations between treatment factors and live-birth rates among more homogenous groups of patients. To address concerns that in the absences of male factor infertility ICSI might be used preferentially for women considered difficult to treat, multiple groups of patients with an indication of being difficult to treat were evaluated separately. These groups included women with previous failed ART cycles, women diagnosed with diminished ovarian reserve, and women with a low number of eggs retrieved (<5). Within each of these groups, age-specific live-birth rates for IVF-ET with and without ICSI were examined. In all analyses, women who used IVF with ICSI had lower success rates compared with women who used IVF without ICSI (data not indicated). Thus, the pattern of results remained consistent with the findings presented (Table 4). To address concerns that extended (i.e., day 5) embryo culture might be used preferentially for women with a presumed better prognosis, data regarding women deemed to have a higher likelihood of success were evaluated separately; these subgroups included women with above average number of eggs retrieved (>10), women with diagnoses other than diminished ovarian reserve, and women with extra embryos cryopreserved for future use. Again, the pattern of results for analyses within each of these subgroups remained consistent with the findings presented (Table 4) (data not indicated). Finally, analyses were conducted in which the data were stratified by patient age, number of embryos transferred, and number of embryos available simultaneously. These results are included with the discussion regarding multiple-birth risk. Total live-birth rates are compared with singleton live-birth rates for women who underwent ART procedures in which freshly fertilized embryos from their own eggs were used (Figure 2). Both live-birth rates and singleton live-birth rates decreased with patient age. Across all age groups, singleton live-birth rates were lower than live-birth rates. However, the magnitude of the difference between these two measures declined with patient age. Total live-birth rates ranged from 41% among women aged <35 years to 7% among women aged >42 years, and singleton live-birth rates ranged from 25% among women aged <35 years to 6% among women age >42 years. Multiple BirthsOf 10,377 multiple-birth deliveries, 7,805 were from pregnancies conceived with freshly fertilized embryos from the patient's eggs; 823 were from thawed embryos from the patient's eggs; 1,514 were from freshly fertilized embryos from a donor's eggs; and 235 were from thawed embryos from a donor's eggs (Table 5). In comparison with ART procedures using the patient's eggs and freshly fertilized embryos, the risks for multiple-birth delivery were increased when eggs from a donor were used and decreased when thawed embryos were used. Among ART procedures in which the patient's own eggs were used, a strong inverse relation existed between multiple-birth risk and patient age. The average multiple-birth risk (i.e., multiple-birth delivery rate) for ART procedure in which freshly fertilized embryos from the patient's eggs were used was 36%. This rate varied from 40% among women aged <35 years to 14% among women aged >42 years. Of 40,687 infants born through ART, 53% (21,720) were born in multiple-birth deliveries (Table 5). The proportion of infants born in a multiple-birth delivery also varied by type of ART procedure and patient age. A more detailed examination of multiple-birth risk for women who underwent ART procedures in which freshly fertilized embryos from their own eggs were used revealed that number of embryos transferred was a risk factor for multiple-birth delivery, but the magnitude of the risk varied according to patient age (Figures 3--7). Among all age groups, transfer of >2 embryos resulted in increased live-birth delivery rates. However, the multiple-birth risk was also substantially increased. Among all age groups, with the exception of women aged >42 years (Figures 3--6), the percentage of multiple-birth deliveries increased with increasing number of embryos transferred from 2 to >5. As a result, if success were evaluated in terms of singleton live-birth deliveries rather than total live-birth deliveries, the two youngest age groups had lower singleton success rates when >3 embryos were transferred than when 2 embryos were transferred (Figures 3 and 4). For women aged 38--40 years (Figure 5), transfer of >3 embryos offered a certain advantage in terms of live-birth delivery rates. However, as among younger age groups, the percentage of twin deliveries and triplet or higher order multiple-birth deliveries were increased with >3 embryos having been transferred compared with two. For women aged 41--42 years (Figure 6), both the live-birth delivery rate and the multiple-birth risk increased steadily with an increased number of embryos having been transferred. The percentage of triplet or higher order multiple-birth deliveries did not demonstrate a trend. For women aged >42 years (Figure 7), the percentage of multiple-birth deliveries did not demonstrate a trend by number of embryos (>2) having been transferred.** A further assessment of multiple-birth risk among patients who used freshly fertilized embryos from their own eggs and set aside extra embryos for future use is also presented (Figures 8--11). This group can be thought of as those with elective embryo transfer because they are known to have chosen to transfer fewer embryos than the total number available. For women with elective embryo transfer who were aged <35 years, 35--37 years, and 38--40 years, live-birth rates were highest when only two embryos were transferred (Figures 8--10). In addition, live-birth rates among women in these three youngest age groups were >29% with elective transfer of only one embryo. Thus, singleton live-birth rates did not demonstrate any or much improvement when two embryos were transferred. Rather, the added live-birth rates observed with two embryos transferred incurred a substantial risk of multiple births. The number of cases of elective transfer of one embryo among women aged 41--42 years was too limited to allow adequate evaluation. Live-birth rates with elective transfer of 2-->5 embryos demonstrated limited variation for this age group. Data are not provided for women aged >42 years because in this age group limited sample sizes existed for all numbers of elective embryo transfer. The total number and percentage of infants born in multiple-birth deliveries by maternal state of residence is presented (Table 6). The states with the highest number of ART-associated live-birth deliveries also had the highest number of infants born in multiple-birth deliveries. These include California (2,673), New York (2,353), Massachusetts (1,399), New Jersey (1,358), Texas (1,286), and Illinois (1,278). Nationally, the percentage of infants born in multiple-birth deliveries after ART was used was 53%; the percentage of twins and triplets or more were 46% and 8%, respectively. The percentage of infants born in multiple-birth deliveries was >50% in the majority of states. The states with the highest proportion of infants born in multiple-birth deliveries were Alabama (61%), Colorado (61%), Montana (69%) Rhode Island (61%), and Tennessee (61%). The contribution of ART infants to the total number of U.S. infants born in 2001 is presented (Table 7). Of 4,025,933 total infants born in the U.S. in 2001, a total of 37,087 (1%) were conceived by using ART. Infants conceived with ART accounted for 0.4% of singleton births and 16% of multiple births nationally. Fourteen percent of all twins and 42% of infants born in triplets and higher order multiples were conceived with ART. DiscussionAccording to the latest estimates of infertility in the United States from the 1995 National Survey of Family Growth, 15% of women of reproductive age reported a past infertility-associated health-care visit, and 2% reported a visit in the past year (8). Among married couples in which the woman was of reproductive age, 7% reported they had not conceived after 12 months of unprotected intercourse. With advances in ART, couples are increasingly turning to these treatments to overcome their infertility. Since the birth of the first infant through ART in the United States in 1981, use of ART has grown substantially. Since 1997, CDC has been monitoring ART procedures performed in the United States. During that time, a notable and consistent increase in the use of ART has occurred. The increased use of ART coupled with higher ART success rates has resulted in dramatic increases in the number of children conceived through ART each year. From 1996 (i.e., the first full year for which CDC collected data) through 2001, the number of ART procedures performed increased 66%, from 64,724 to 107,587 (1). Additionally, from 1996 to 2001, live-birth rates for all types of ART procedures increased substantially. For the most common type of ART procedure, using freshly fertilized embryos from the patient's eggs, live birth rates increased from 28% in 1996 to 33% in 2001. The number of infants conceived through ART increased 94%, from 20,921 infants conceived through ART procedures performed in 1996 to 40,687 infants conceived through ART procedures performed in 2001. This report documents that in 2001, ART use varied according to patient's state of residency. Residents of California, New York, Massachusetts, Illinois, and New Jersey reported the highest number of ART procedures. These states also reported the highest number of infants conceived through ART. In 2001, ART use by state of residency was not completely in line with expectations based on the total population within states (9,10). Whereas Massachusetts had the third highest number of ART procedures performed, it ranked thirteenth in terms of total population size.†† Likewise, residents of Rhode Island underwent more ART procedures than would have been expected based on their population size. As a result, state-specific ratios of ART procedures by population varied according to state of residency. States with the highest ratio of number of ART procedures among state residents per million population were Massachusetts (1,273), Maryland (758), New Jersey (706), District of Columbia (695), and Rhode Island (682). This divergence is not unexpected because in 2001 both Massachusetts and Rhode Island had a statewide mandate for insurance coverage for ART procedures. The state variation might also be related to availability of ART services within each state. However, the relation between demand for services and availability cannot be disentangled (i.e., increased availability in certain states might reflect the increased demand for ART among state residents). Patients with different characteristics used ART services. Among ART treatments in which freshly fertilized embryos from the patient's eggs were used (i.e., the most frequent type of ART treatment), substantial variation was observed in patient age, infertility diagnoses, history of past infertility treatment, and past births. Success rates from ART use are affected by numerous patient and treatment factors; hence, considering one single measure of success in evaluating ART efficacy is not informative. At a minimum, ART treatments need to be subdivided into categories on the basis of the source of the egg (patient or donor) and the status of the embryos (freshly fertilized or thawed) because success rates vary substantially across these types. Within the type of ART treatment, further variation exists in success rates by patient and treatment factors, most notably patient age. Other factors to consider when assessing success rates are infertility diagnosis, number of previous ART procedures, number of previous births, type of ART procedures, number of days of embryo culture, number of embryos transferred, availability of extra embryos, and use of a gestational carrier (surrogate). Variation exists in success rates according to each of these factors. CDC's primary focus in collecting ART data has been live-birth deliveries as an indicator of success, because ART surveillance activities were developed in response to a federal mandate to report ART success rate data. This mandate requires that CDC collect data from all ART medical centers and report success rates, defined as all live births per ovarian stimulation procedures or ART procedures, for each ART clinic. Thus, a key role for CDC has been to publish standardized data related to ART success rates, including information regarding factors that affect these rates. With these data, couples can make informed decisions regarding whether to undergo this time-consuming and expensive treatment (11,12).§§ However, success-rate data must also be balanced with consideration of effects on maternal and infant health. Thus, CDC also closely monitors multiple births conceived through ART. Multiple births are associated with an increased health risk for both mothers and infants (13--15). Women with multiple-gestation pregnancies are at increased risk for maternal complications (e.g., hemorrhage and hypertension). Infants born in a multiple-birth delivery are at increased risk for prematurity, low birthweight, infant mortality, and long-term disability. The health risks associated with multiple births have also contributed to rising health-care costs. In 2001, the estimated costs per delivery resulting from ART procedures ranged from $38,345 to $84,819 (12). Hospital charges have been estimated to be four times higher for delivery of twins and 11 times higher for delivery of triplets than for singleton deliveries (16). In the United States, multiple births have increased dramatically during the last 2 decades (6,17). The rise in multiple births has been attributed to an increased use of ART and delayed childbearing (4,18,19). Although infants conceived with ART accounted for 1% of the total births in the U.S. in 2001, the proportion of twins and triplets or more attributed to ART were 14% and 42%, respectively. In certain states, such infertility treatments as ART might not be covered by insurance carriers, and patients might feel pressure to maximize the opportunity for live-birth delivery. Additionally, anecdotal evidence suggests that certain ART providers might feel pressure to maximize their publicly reported success rates, if defined solely as total live-birth delivery, by transferring multiple embryos. Indeed, in the United States, high-order embryo transfer is still common practice. In 2001, approximately 66% of ART cycles that used fresh, nondonor eggs or embryos and progressed to the embryo-transfer stage involved the transfer of >3 embryos; approximately 32% of cycles involved the transfer of >4; and 11% of cycles involved the transfer of >5 embryos. Recent reports published in the scientific literature have advocated for the presentation of singleton live-birth rates as a distinct indicator of ART success (20--24). This report includes this measure and presents it with total live-birth rates. Success rates based on singleton live-birth deliveries will provide patients with a measure that more directly highlights infant outcomes with the optimal short- and long-term prognosis. Data regarding multiple-birth deliveries and proportion of multiple-birth infants as distinct outcomes are provided also. Data in this report indicate that 54% of infants born through ART in 2001 were multiple births; this compares with 3% in the general U.S. population during the same period (6,25). The twin rate was 45%, 15 times higher than in the general U.S. population (3%); the triplet and higher order multiples rate was 8%, a total of 42 times higher than the general U.S. population (0.2%). Regarding the specific type of ART treatment, the rates are even higher for women who underwent ART procedures using freshly fertilized embryos from their own eggs (54% total multiple births) or from donor eggs (60% total multiple births). In the majority of states, >50% of infants conceived through ART were born in multiple-birth deliveries. Alabama, Colorado, Montana, Rhode Island, and Tennessee reported ART-associated multiple-birth rates >60%. Multiple births resulting from ART are an increasing public health problem, nationally and for the majority of states. The findings in this report confirm the need to reduce the occurrence of multiple births resulting from ART. For women who underwent ART procedures using freshly fertilized embryos from their own eggs, the multiple-birth risk increased when multiple embryos were transferred (>2). However, embryo availability (an indicator of embryo quality) was also a strong predictor of multiple-birth risk and had added predictive value beyond the number of embryos transferred. When patient age, number of embryos transferred, and embryo availability were jointly considered, for certain subgroups, high live-birth rates and singleton live-birth rates were achieved with the transfer of one or two embryos. Thus, among certain groups, multiple-birth risk can be minimized by limiting the number of embryos transferred without compromising success rates. This analysis was subject to certain limitations. First, ART surveillance data are reported for each ART procedure performed rather than for each patient who used ART. Linking procedures among patients who underwent >1 ART procedure in a given year is not possible. Because patients undergoing >1 procedure in a given year are most likely to be those who failed >1 treatment, the success rates reported here might underestimate the true per-patient success rate. Additionally, ratios of ART procedures per population might be higher than the unknown ratio of number of persons undergoing ART per population. Second, these data represent couples who sought ART services in 2001; therefore, success rates do not represent all couples with infertility who were potential ART users in 2001. Third, 9% of medical centers that performed ART in 2001 did not report their data to CDC as required. ART data are reported to CDC by the ART medical center where the procedure was performed rather than by the state where the patient resided. In this report, ART data are presented by the female patient's state of residence. In previous reports (18), ART data were not presented by state of residence because of incomplete residency data. In 2001, residency data were missing for <9% of all live-birth deliveries reported to CDC. The range of missing residency data varied by medical center. Medical centers located in 45 states had <5% missing residency data; medical centers located in five states had 5%--9% missing residency data; and medical centers located in four states had >10% missing residency data. These states were Georgia, Massachusetts, Minnesota, and New York. In cases of missing residency data, residency was assigned as the state in which the ART procedure was performed. Thus, the number of procedures performed among state residents, number of infants, and number of multiple-birth infants might have been overestimated for these states. Concurrently, the numbers might be underestimated in states bordering states with missing residency data, particularly states in the Northeast region of the United States. Nonetheless, the effects of missing residency data were not substantial. Statistics were evaluated separately according to the state in which the ART medical center was located rather than the patient's state of residence. The rankings of the states in terms of total number of infants and multiple-birth infants were similar to the rankings based on patient's state of residence (data not indicated). A further concern to consider in reviewing the state-based statistics in this report is that the patient's state of residence was reported at the time of ART treatment. The possibility of migration during the interval between ART treatment and birth exists. Data from the U.S. Census Bureau demonstrate that annually, approximately 3% of the U.S. population move between states. This rate is even higher for persons aged 20--35 years (26). One group with a recognized high potential for migration is members of the U.S. armed forces. Therefore, ART procedures performed among patients who attended military medical centers were evaluated separately. In 2001, a total of 771 (0.7%) ART procedures were performed in four military medical centers. These medical centers were located in California, the District of Columbia, Hawaii, and Texas. In certain of these facilities, a substantial number of distinct states were listed for patient's state of residence. States for which >1% of ART procedures among state residents were performed in a military medical center were Alabama, Colorado, Kansas, Louisiana, Maine, Maryland, New Mexico, North Carolina, Oklahoma, South Carolina, and Texas. States for which >5% of ART procedures among state residents were performed in a military medical center were Alaska, the District of Columbia, Hawaii, and Virginia. Despite these limitations, findings from national surveillance of ART procedures performed in the United States provide useful information for patients contemplating ART, ART providers, and health-care policy makers. First, ART surveillance data can be used to monitor trends in ART use and outcomes from ART procedures. Second, data from ART surveillance can be used to assess patient and treatment factors that contribute to higher success rates. Third, ongoing surveillance data can be used to assess the risk of multiple births. Fourth, surveillance data provide information to assess changes in clinical practice related to ART treatment. Multiple births are one of the most important public health concerns associated with using ART. Increased use of ART treatments and the widespread practice of transferring multiple embryos during ART treatments has led to a substantial increase in multiple-birth rates in the United States (4,17). Although balancing the chance of success with ART against the risk of multiple births is difficult in certain cases, efforts should be made to limit the number of embryos transferred for patients undergoing ART. Such efforts will ultimately require ART patients and providers to view treatment success in terms of singleton pregnancies and births. Additionally, continued research is critical to understanding the effect of ART on maternal and child health. CDC will continue to provide updates of ART use in the United States as data become available. AcknowledgmentsThe data used for this study were collected by the Society for Assisted Reproductive Technology (SART). The SART system is jointly supported by CDC, Atlanta, Georgia; SART, Birmingham, Alabama; and the American Society for Reproductive Medicine (ASRM), Birmingham, Alabama. The authors thank SART and ASRM, without whose contributions this work would not have been possible. References
* Fertility Clinic Success Rate and Certification Act of 1992 (FCSRCA), Public Law 102-493, October 24, 1992. † Data regarding population size are based on July 1, 2001, estimates from the U.S. Census Bureau (9,10). § Includes only the number of infants live-born in a multiple-birth delivery. For example, if three infants were born in a live-birth delivery and one of the three infants was stillborn, the total number of live-born infants would be two. However, these two infants would still be counted as triplets. ¶ Data were not available to distinguish whether previous births were conceived naturally or conceived with ART or other infertility treatments. ** Results are based on total multiple-birth risk and thus do not provide an indication of pregnancies that began as twins, triplets, or more, but reduced (either spontaneously or through medical intervention) to singletons or twins (Figures 3--11). †† Data regarding population size are based on July 1, 2001, estimates from the U.S. Census Bureau (9,10). §§ Estimated costs for one cycle of IVF range from $7,854 to $11,000 (12). Table 1 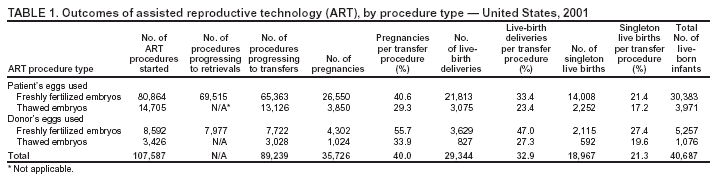 Return to top. Figure 1 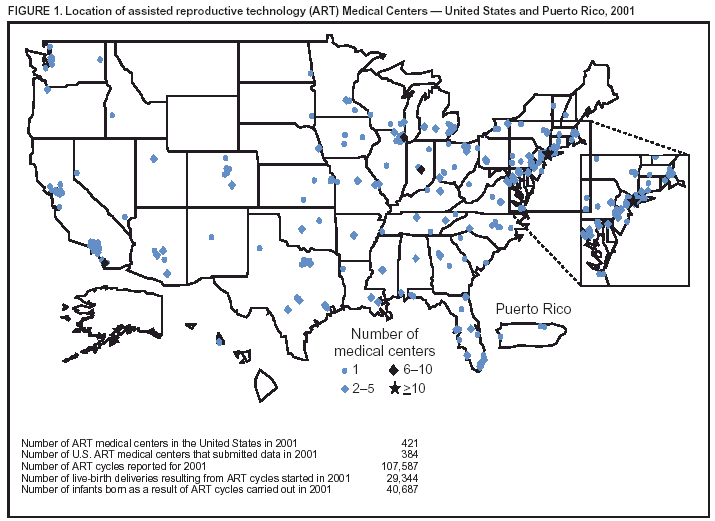 Return to top. Table 2 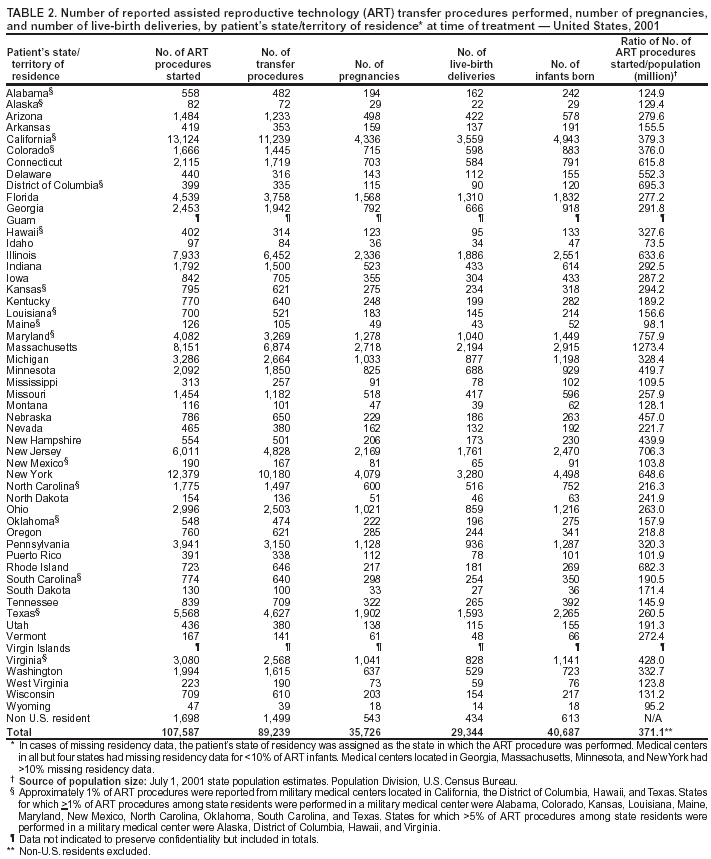 Return to top. Figure 2 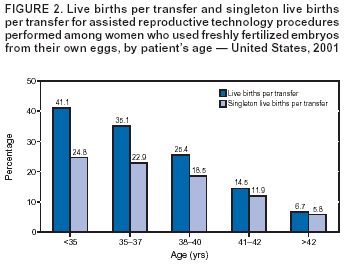 Return to top. Table 3 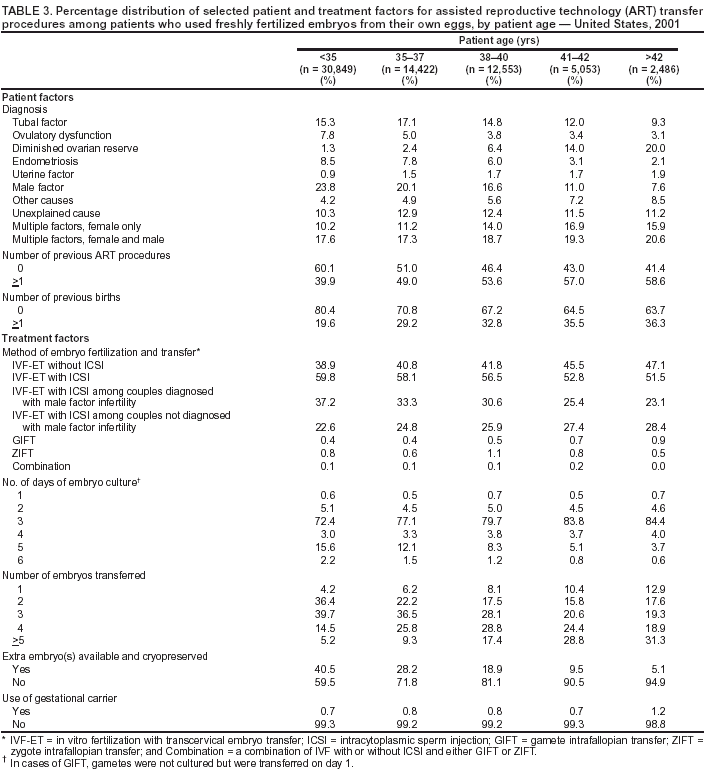 Return to top. Table 4 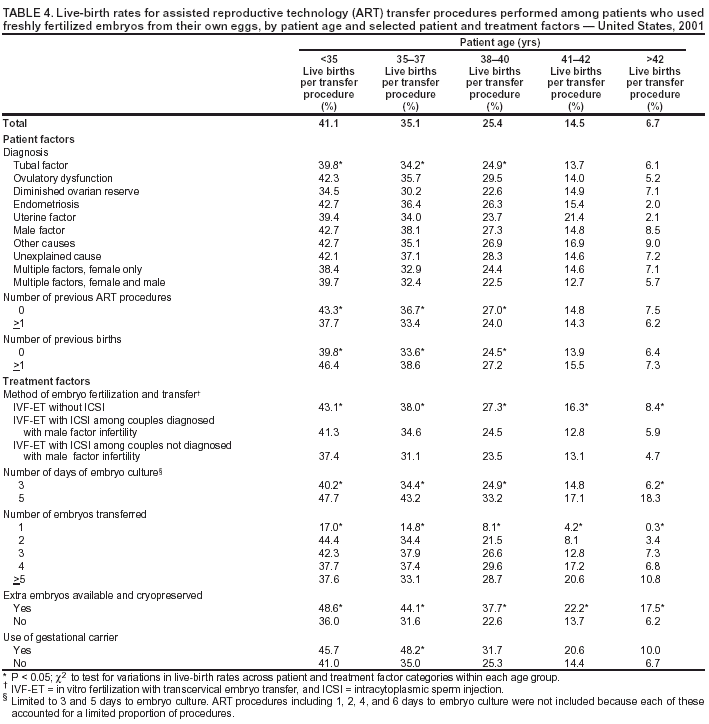 Return to top. Table 5 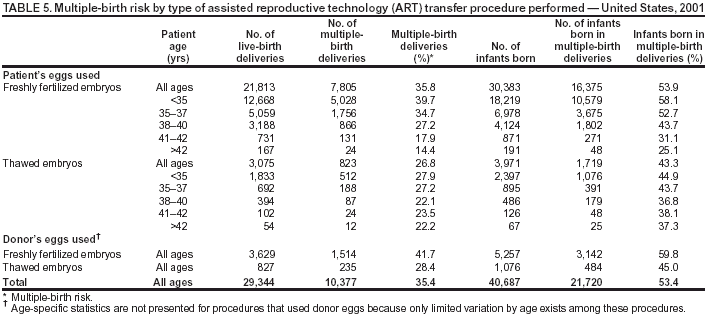 Return to top. Figure 5 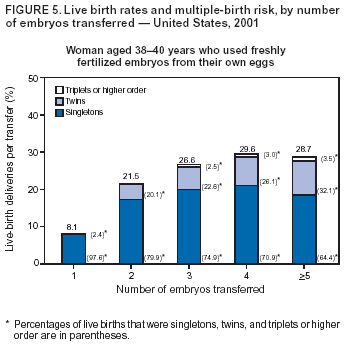 Return to top. Table 6 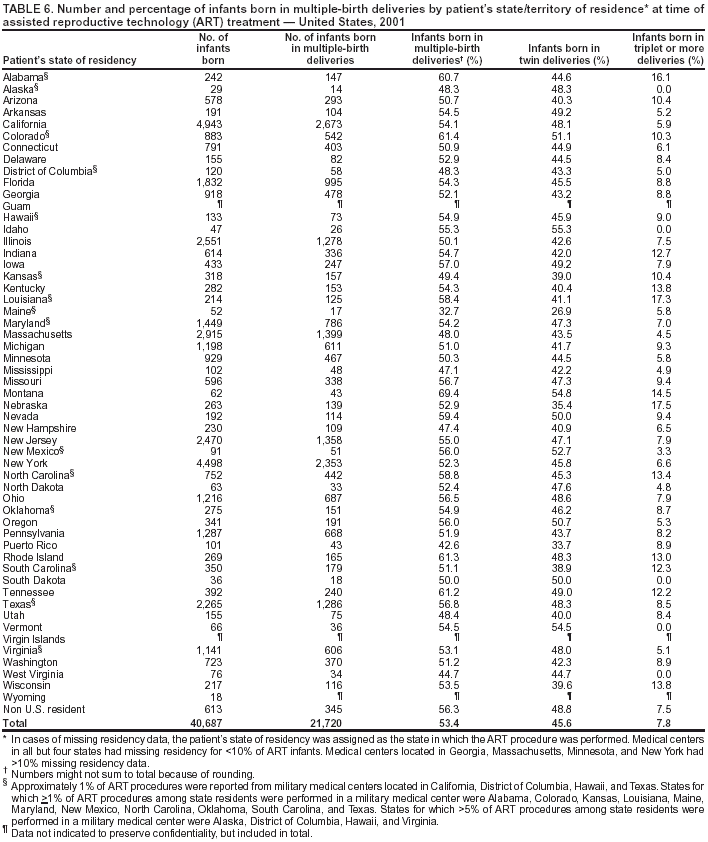 Return to top. Figure 6 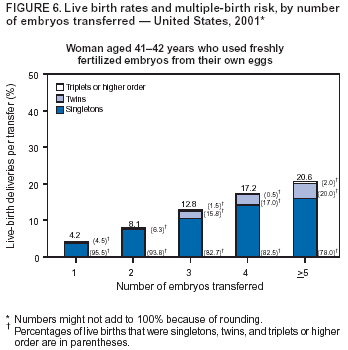 Return to top. Table 7 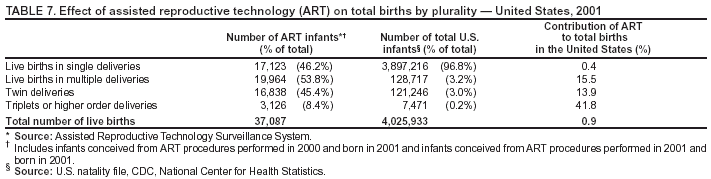 Return to top. Figure 7 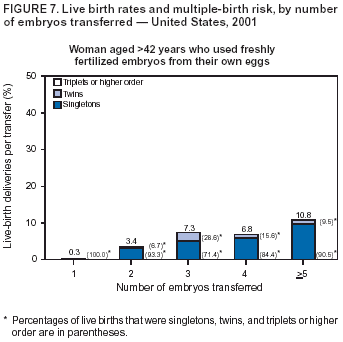 Return to top. Figure 8 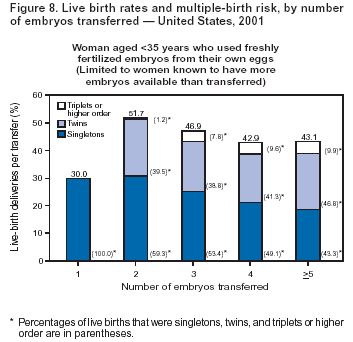 Return to top. Figure 9 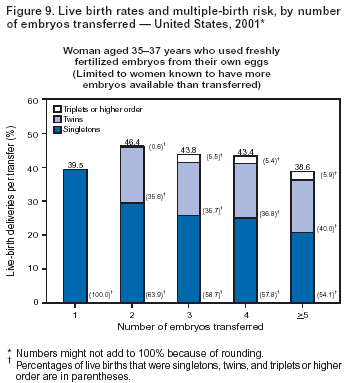 Return to top. Figure 10 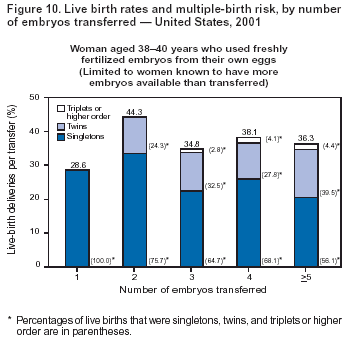 Return to top. Figure 11 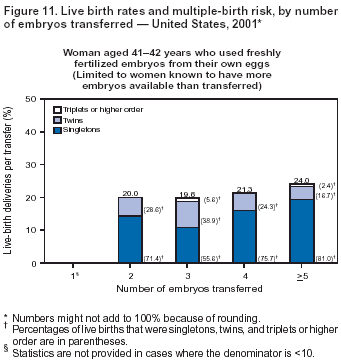 Return to top.
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to [email protected].Page converted: 4/19/2004 |
|||||||||
This page last reviewed 4/19/2004
|