|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail. Surveillance for Waterborne-Disease Outbreaks Associated with Drinking Water --- United States, 2001--2002Brian G. Blackburn, M.D.,1,2 Gunther F. Craun, M.P.H.,3 Jonathan S. Yoder, M.P.H., M.S.W.,1,4 Vincent Hill,
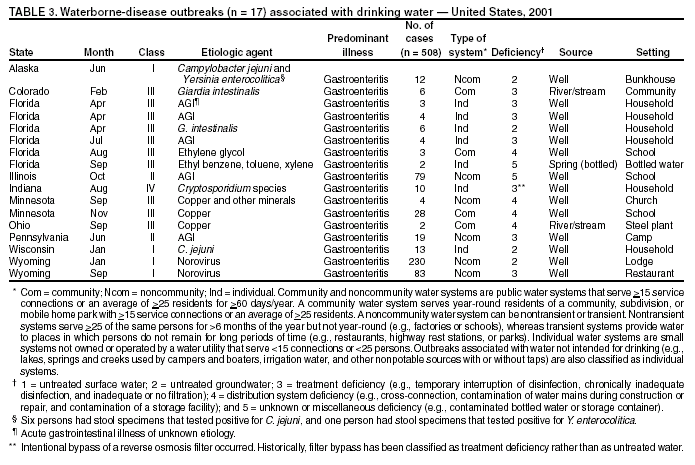
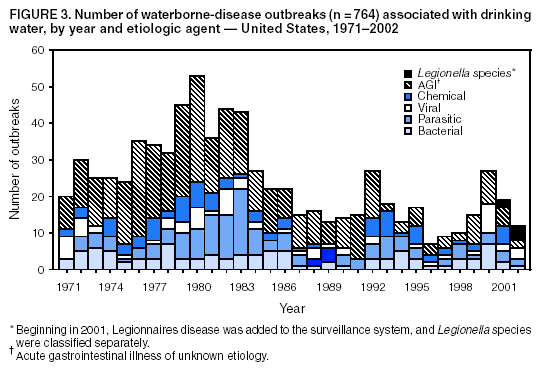
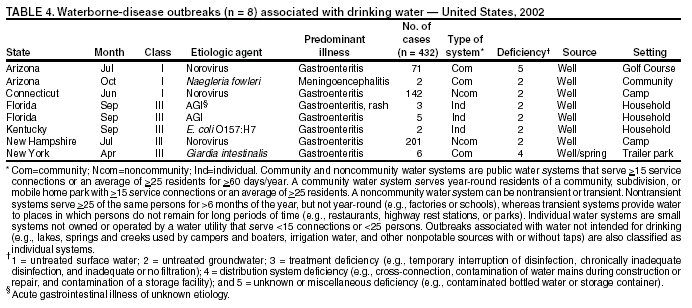
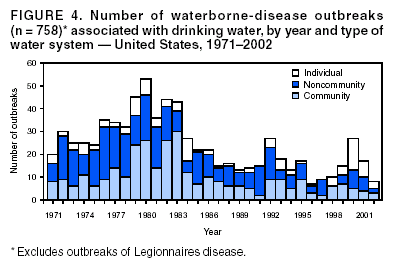
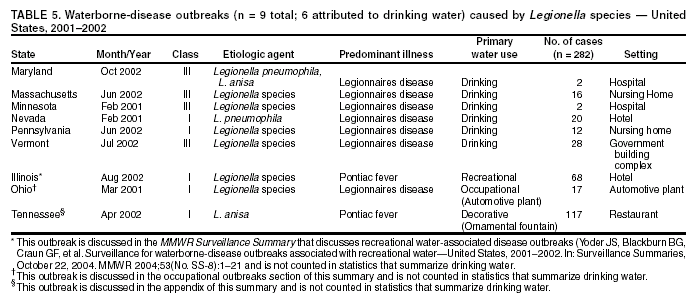
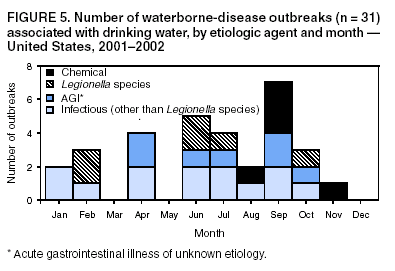
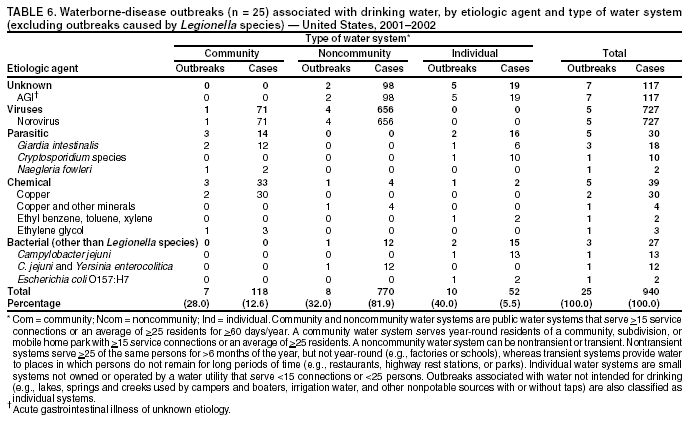
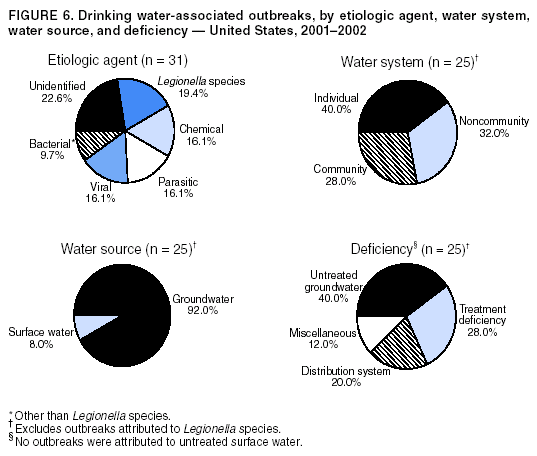
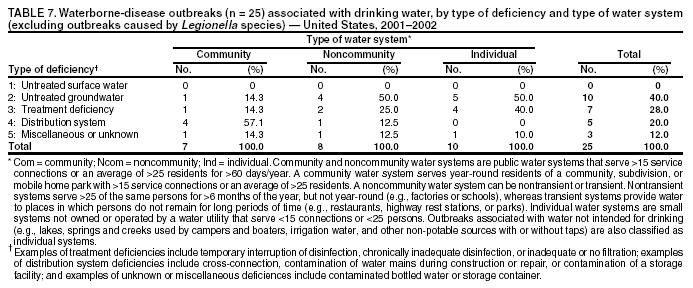
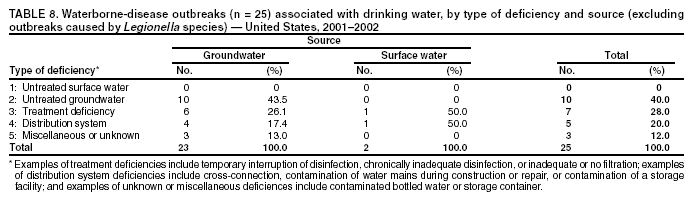
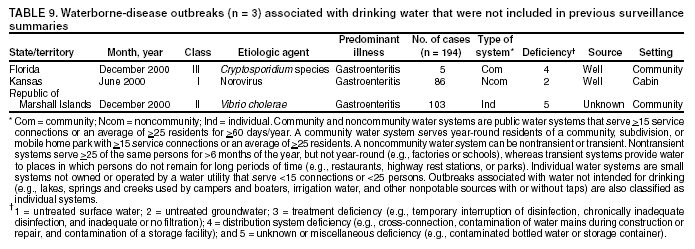
Ph.D.,1 Corresponding author: Brian G. Blackburn, M.D., EIS Officer, CDC/NCID/DPD, 1600 Clifton Rd., NE, MS F-22, Atlanta, GA 30341; Fax: 770-488-7761; E-mail: [email protected]. Abstract Problem/Condition: Since 1971, CDC, the U.S. Environmental Protection Agency, and the Council of State and Territorial Epidemiologists have maintained a collaborative surveillance system for collecting and periodically reporting data related to occurrences and causes of waterborne-disease outbreaks (WBDOs). This surveillance system is the primary source of data concerning the scope and effects of waterborne disease outbreaks on persons in the United States. Reporting Period Covered: This summary includes data on WBDOs associated with drinking water that occurred during January 2001--December 2002 and on three previously unreported outbreaks that occurred during 2000. Description of the System: Public health departments in the states, territories, localities, and the Freely Associated States are primarily responsible for detecting and investigating WBDOs and voluntarily reporting them to CDC on a standard form. The surveillance system includes data for outbreaks associated with both drinking water and recreational water; only outbreaks associated with drinking water are reported in this summary. Results: During 2001--2002, a total of 31 WBDOs associated with drinking water were reported by 19 states. These 31 outbreaks caused illness among an estimated 1,020 persons and were linked to seven deaths. The microbe or chemical that caused the outbreak was identified for 24 (77.4%) of the 31 outbreaks. Of the 24 identified outbreaks, 19 (79.2%) were associated with pathogens, and five (20.8%) were associated with acute chemical poisonings. Five outbreaks were caused by norovirus, five by parasites, and three by non-Legionella bacteria. All seven outbreaks involving acute gastrointestinal illness of unknown etiology were suspected of having an infectious cause. For the first time, this MMWR Surveillance Summary includes drinking water-associated outbreaks of Legionnaires disease (LD); six outbreaks of LD occurred during 2001--2002. Of the 25 non-Legionella associated outbreaks, 23 (92.0%) were reported in systems that used groundwater sources; nine (39.1%) of these 23 groundwater outbreaks were associated with private noncommunity wells that were not regulated by EPA. Interpretation: The number of drinking water-associated outbreaks decreased from 39 during 1999--2000 to 31 during 2001--2002. Two (8.0%) outbreaks associated with surface water occurred during 2001--2002; neither was associated with consumption of untreated water. The number of outbreaks associated with groundwater sources decreased from 28 during 1999--2000 to 23 during 2001--2002; however, the proportion of such outbreaks increased from 73.7% to 92.0%. The number of outbreaks associated with untreated groundwater decreased from 17 (44.7%) during 1999--2000 to 10 (40.0%) during 2001--2002. Outbreaks associated with private, unregulated wells remained relatively stable, although more outbreaks involving private, treated wells were reported during 2001--2002. Because the only groundwater systems that are required to disinfect their water supplies are public systems under the influence of surface water, these findings support EPA's development of a groundwater rule that specifies when corrective action (including disinfection) is required. Public Health Action: CDC and EPA use surveillance data 1) to identify the types of water systems, their deficiencies, and the etiologic agents associated with outbreaks and 2) to evaluate the adequacy of technologies for providing safe drinking water. Surveillance data are used also to establish research priorities, which can lead to improved water-quality regulations. CDC and EPA recently completed epidemiologic studies that assess the level of waterborne illness attributable to municipal drinking water in nonoutbreak conditions. The decrease in outbreaks in surface water systems is attributable primarily to implementation of provisions of EPA rules enacted since the late 1980s. Rules under development by EPA are expected to protect the public further from microbial contaminants while addressing risk tradeoffs of disinfection byproducts in drinking water. IntroductionDuring 1920--1970, statistical data regarding U.S. waterborne-disease outbreaks (WBDOs) were collected by different researchers and federal agencies (1). Since 1971, CDC, the U.S. Environmental Protection Agency (EPA), and the Council of State and Territorial Epidemiologists (CSTE) have maintained a collaborative surveillance system that tracks the occurrences and causes of WBDOs associated with drinking water; tabulation of recreational water-associated outbreaks was added to the surveillance system in 1978 (2--7). The surveillance system includes data regarding outbreaks associated with drinking water, recreational water, and other types of water exposures. This MMWR Surveillance Summary includes data for drinking water-associated outbreaks that occurred during 2001--2002 and for three previously unreported outbreaks that occurred in 2000. Recreational water-associated outbreaks are presented in a separate MMWR Surveillance Summary (8). These surveillance activities are intended to 1) characterize the epidemiology of WBDOs; 2) identify changing trends in the etiologic agents that caused WBDOs and determine why the outbreaks occurred; 3) encourage public health personnel to detect and investigate WBDOs; and 4) foster collaboration among local, state, federal, and international agencies on initiatives to prevent waterborne disease transmission. Data obtained through this surveillance system are useful for identifying major deficiencies in providing safe drinking water. Surveillance information can influence research priorities and lead to improved water-quality regulations. However, the statistics reported in this surveillance summary represent only a portion of the burden of illness associated with drinking water exposure. The surveillance information does not include endemic waterborne disease risks, nor are reliable estimates available of the number of unrecognized WBDOs and associated cases of illness. BackgroundEPA Drinking Water RegulationsPublic water systems are regulated under the Safe Drinking Water Act (SDWA) of 1974 and its subsequent 1986 and 1996 amendments (Table 1) (9--11). SDWA authorizes EPA to set national standards to protect drinking water and its sources against naturally occurring or human-made contaminants. Microbial contamination is regulated under the Total Coliform Rule (TCR), Surface Water Treatment Rule (SWTR), Interim Enhanced SWTR (IESWTR), and Long Term 1 Enhanced SWTR (LT1ESWTR). In addition, EPA's lead, copper, and arsenic rules prescribe action levels at which a system must take corrective steps (12,13). These rules have been described previously (2). All public water systems are required by TCR to monitor for total coliforms at a prescribed frequency (14,15). SWTR (16) and IESWTR (17) apply to public systems that serve >10,000 persons and that use surface water or groundwater under the direct influence of surface water and are intended to protect the public against exposure to Giardia intestinalis, Cryptosporidium, viruses, Legionella, and selected other pathogens. LT1ESWTR applies to public systems that serve <10,000 persons and is intended to improve the control of microbial pathogens, especially Cryptosporidium (18,19). An additional regulation, the Filter Backwash Recycling Rule, requires the return of recycle flows to the water treatment process so microbial contaminant removal is not compromised (19,20). Recently proposed microbial and disinfection byproducts regulations include the Long Term 2 Enhanced Surface Water Treatment Rule (LT2ESWTR) and the Stage 2 Disinfectants and Disinfection Byproducts Rule (DBPR). These regulations were developed simultaneously to address risk tradeoffs between control of pathogens and limiting exposure to disinfection byproducts (DBPs) that can form in water from the disinfection process used to control microbial pathogens (21). LT2ESWTR (22,23) mandates source-water monitoring for Cryptosporidium and additional treatment for filtered systems on the basis of source-water concentrations; inactivation of Cryptosporidium by all unfiltered systems; disinfection profiling and benchmarking to ensure continued levels of microbial protection while system operators take steps to comply with new DBP limits; and covering, treating, or implementing a risk-management plan for uncovered finished water-storage facilities. DBPR applies to all community and nontransient, noncommunity water systems that add a disinfectant other than ultraviolet light (24). DBPR requires systems to meet maximum contaminant levels at each monitoring site in the distribution system, determine if they are experiencing short-term peaks in DBP levels, and better identify monitoring sites at which consumers are exposed to high DBP levels. The 1996 amendments require EPA to develop regulations that mandate disinfection of groundwater systems as necessary to protect the public health. The proposed Ground Water Rule (GWR) (information available at http://www.epa.gov/safewater/gwr.html) will specify when corrective action, including disinfection, is required to protect consumers from bacteria and viruses (25). Proposed requirements include periodic sanitary surveys to identify deficiencies, hydrogeologic sensitivity assessments for undisinfected systems, source-water microbial monitoring from certain systems, and compliance monitoring for systems that disinfect to ensure adequate inactivation or removal of viruses. SDWA's Wellhead Protection Program requires every state to develop a program to delineate wellhead protection areas in which sources of contamination are managed to minimize groundwater contamination (25). Additional protection of groundwater sources, especially from contamination by shallow wells and cesspools, is provided by the Underground Injection Control Regulations (26). Every 5 years, EPA is also required to publish a list of contaminants that are known or anticipated to occur in public water systems and that might need to be regulated. The first drinking water Contaminant Candidate List (CCL) was issued in 1998 and included 50 chemical and 10 microbial contaminants (27); however, EPA decided not to regulate any of the waterborne pathogens included in CCL. EPA also must establish criteria for a program to monitor unregulated contaminants and publish a list of contaminants to be monitored (28--30). Microorganisms were included among the contaminants for which analytical methods are available (Aeromonas) and contaminants for which analytical methods are being developed (Helicobacter pylori, cyanobacteria, coxsackieviruses, microsporidia, adenoviruses, and caliciviruses). An ongoing screening survey for Aeromonas, and selected chemical contaminants will help determine whether these should be considered or excluded for regulation. MethodsData SourcesPublic health departments in the states, territories, localities, and the Freely Associated States* (FAS) have primary responsibility for detecting and investigating WBDOs, which they report voluntarily to CDC by using a standard form (CDC form 52.12, available at http://www.cdc.gov/healthyswimming/downloads/cdc_5212_waterborne.pdf). The form solicits data on characteristics of the outbreak, including person, place, time, and location; results from epidemiologic studies conducted; specimen and water sample testing; and other factors potentially contributing to the outbreak (e.g., environmental concerns, disinfection, and filtration [Glossary]). CDC annually requests reports from state, territorial, and FAS epidemiologists or persons designated as WBDO surveillance coordinators and obtains additional information regarding water quality and treatment as needed. Numeric and text data are abstracted from the outbreak form and supporting documents and entered into a database for analysis. Definitions†The unit of analysis for the WBDO surveillance system is an outbreak, not an individual case of a waterborne disease. Two criteria must be met for an event to be defined as a drinking water-associated disease outbreak. First, >2 persons must have experienced a similar illness after exposure to water. This criterion is waived for single cases of laboratory-confirmed primary amebic meningoencephalitis (PAM) and for single cases of chemical poisoning if water-quality data indicate contamination by the chemical. Second, epidemiologic evidence must implicate drinking water as the probable source of the illness. Reported outbreaks caused by contaminated water or ice at the point of use (e.g., a contaminated water faucet or serving container) are not classified as drinking water-associated outbreaks, and WBDOs associated with cruise ships are not summarized in this report. Different types of drinking water systems are used for outbreak classification (Figure 1). Public water systems, which are classified as either community or noncommunity systems (Glossary), are regulated under SDWA. Of the approximately 161,000 public water systems in the United States, 108,000 (67.1%) are noncommunity systems, including 88,000 transient systems and 20,000 nontransient systems (Glossary), and 53,000 (32.9%) are community systems. Despite representing a minority of water systems, community systems serve 273 million persons (approximately 93.9% of the U.S. population) (31). Furthermore, a limited number of community systems (3,900 [7.4%]) provide water to 81% of the community system population (31). Noncommunity, nontransient systems provide water to 6.3 million persons, and 23.3 million persons use noncommunity, transient systems (by definition, these populations also use another type of water system at their residences, except for the limited number of permanent residents of nontransient systems) (31). Although the majority of public water systems (90.9%) are supplied by groundwater, more persons (66.2%) drink from public systems served by surface water. Approximately 17 million persons (6.0%) rely on private, individual water systems (31) (Glossary). In this surveillance system, drinking water-associated outbreaks involving water not intended for drinking (e.g., lakes, springs, and creeks used by campers and boaters; irrigation water, and other nonpotable sources with or without taps) are also classified as individual systems (Glossary). Sources used for bottled water are also classified as individual systems; bottled water is not regulated by EPA but is subject to regulation by the Food and Drug Administration (FDA). Each drinking water system associated with a WBDO is classified as having a deficiency. Deficiency classifications are as follows: 1: untreated surface water; Outbreak ClassificationWBDOs reported to the surveillance system are classified according to the strength of the evidence implicating water as the vehicle of transmission (Table 2). The classification scheme (i.e., Classes I--IV) is based on the epidemiologic and water-quality data provided on the outbreak report form. Epidemiologic data are weighted more than water-quality data. Although outbreaks without water-quality data might be included in this summary, reports that lack epidemiologic data were excluded. Single cases of PAM or chemical poisoning are not classified according to this scheme. Weighting of epidemiologic data does not preclude the relative importance of both types of data. The purpose of the outbreak system is not only to implicate water as the vehicle for the outbreak but also to understand the circumstances and system breakdowns that led to the outbreak. A classification of I indicates that adequate epidemiologic and water-quality data were reported (Table 2). However, the classification does not necessarily imply that an investigation was conducted optimally, nor does a classification of II, III, or IV imply that an investigation was inadequate or incomplete. Outbreaks and the resulting investigations occur under different circumstances, and not all outbreaks can or should be rigorously investigated. In addition, outbreaks that affect fewer persons are more likely to receive a classification of III rather than I because of the relatively limited sample size available for analysis. For the reporting period 2001--2002, WBDOs associated with drinking water and with recreational water are reported separately for the first time. The MMWR Surveillance Summary of recreational water-associated outbreaks (8) includes WBDOs related to recreational water as defined in the methods section of that summary. This MMWR Surveillance Summary includes waterborne outbreaks related to drinking water, those occurring in occupational settings, those associated with Legionella species, and other miscellaneous outbreaks. Although outbreaks of Pontiac fever have been included in previous MMWR Surveillance Summaries of WBDOs, this summary is the first to include outbreaks of Legionnaires disease (LD). Because nearly all outbreaks attributed to Legionella species share characteristics that are distinct from other types of WBDOs, all Legionella outbreaks have been compiled into a single table in this report that identifies the primary use of the water implicated in the outbreak. Although all Legionella outbreaks are listed in this table, only those that occurred in association with water primarily intended for drinking or occupational use are discussed in this summary. Outbreaks of LD that occurred in association with water intended primarily for recreational use are discussed in the summary of recreational water-associated outbreaks (8). Because the parameters used in this summary to assess drinking water-associated outbreaks (i.e., water system type, water source, and deficiency) do not permit adequate evaluation of the characteristics associated with Legionella outbreaks, such parameters are not applied to Legionella outbreaks. For this reason, Legionella outbreaks are counted not in tables and statistics that include these parameters, but only in those related to the total number of drinking water outbreaks and the etiologic agent of these outbreaks. ResultsDuring 2001--2002, a total of 31 outbreaks (19 during 2001 and 12 during 2002) associated with drinking water were reported by 19 states (Figure 2) compared with 39 outbreaks during 1999--2000 (Figures 3 and 4). (Selected case descriptions are located in the Appendix). These 31 outbreaks caused illness among an estimated 1,020 persons, resulting in 51 hospitalizations and seven deaths. The median number of persons affected in an outbreak was six (range: 2--230). Outbreaks peaked during June--September (Figure 5). Florida reported the most outbreaks (eight) during this reporting period. On the basis of epidemiologic and water-quality data, nine (29.0%) of the 31 outbreaks were assigned to Class I, two (6.5%) to Class II, 19 (61.3%) to Class III, and one (3.2%) to Class IV. Outbreaks were analyzed by state (Tables 3, 4, and 5) and tabulated by etiologic agent and water system type (Table 6), type of deficiency and water system (Table 7), and type of deficiency and water source (Table 8). Outbreaks attributable to Legionella are excluded from the analysis of outbreaks by etiologic agent, water system, amd type of deficiency. Etiologic AgentsOf the 31 outbreaks, 19 (61.3%) were of known infectious etiology, seven (22.6%) were of unknown etiology, and five (16.1%) were attributed to chemical poisoning. The outbreaks of known infectious etiology included six (19.4%) that were caused by Legionella species, five (16.1%) by viruses, five (16.1%) by parasites, and three (9.7%) by bacteria other than Legionella species (Figure 6). Unidentified Etiologic Agents Seven outbreaks affecting 117 persons were reported that involved acute gastrointestinal illness of unknown etiology (AGI); no hospitalizations or deaths resulted from these illnesses. Stool specimen testing to identify a causative agent was attempted in only one of these outbreaks. In another of these outbreaks, norovirus was suspected on the basis of symptoms and incubation period in an outbreak of gastrointestinal illness at a church camp in Pennsylvania. However, no confirmatory testing was done of patient samples or of the implicated water. No suspected etiologic agent was noted for any of the other outbreaks in this category. Legionella Species Six outbreaks were attributed to Legionella species. These are described on page 33 of this report. Viruses Five outbreaks affecting 727 persons were attributed to viral infections, all attributed to norovirus. Of the six outbreaks affecting the most persons reported in this summary, five were caused by norovirus. Illnesses from these five outbreaks resulted in two hospitalizations and one death. Parasites Five outbreaks affecting 30 persons were attributed to parasitic infection: three Giardia intestinalis outbreaks, one Cryptosporidium outbreak, and one Naegleria fowleri outbreak. Illnesses from these outbreaks resulted in five hospitalizations and two deaths; both deaths were caused by N. fowleri infection. Chemicals Five outbreaks affecting 39 persons were attributed to chemical contamination. Two were caused by high levels of copper and a third by high levels of copper and other metals. One outbreak was caused by ethylene glycol contamination of a school's water supply and one by ethyl benzene, toluene, and xylene contamination of bottled water. Illnesses from these five outbreaks resulted in no hospitalizations or deaths. Bacteria (Other Than Legionella Species) Three outbreaks affecting 27 persons were attributed to bacterial infection (other than Legionella species): one Escherichia coli O157: H7 outbreak, one Campylobacter jejuni outbreak, and an outbreak involving infection with two different bacteria (of 12 clinically ill persons, six tested positive for C. jejuni and one tested positive for Yersinia enterocolitica). Illnesses from these three outbreaks resulted in three hospitalizations and no deaths. Water-Quality DataWater-quality data (i.e., information regarding the presence of coliform bacteria, pathogens, or chemical contaminants or data regarding levels of disinfectants such as chlorine) were available for 29 (93.5%) of the 31 outbreaks. Among the 26 outbreaks with a suspected or confirmed infectious etiology, 24 (92.3%) provided bacterial water-quality testing data; a positive total or fecal coliform result from the implicated water was reported for 14 (58.3%) of these 24, including 10 (58.8%) of the 17 outbreaks of confirmed infectious etiology, and four (57.1%) of the seven outbreaks of suspected infectious etiology (i.e., AGI). The etiologic organism that caused the outbreak was recovered from the implicated water in 10 (41.7%) of these 24 outbreaks; however, these were the only 10 outbreaks that were tested specifically for the causative microorganism. Legionella species were detected in the implicated water in all six outbreaks caused by this organism, and etiologic organisms were also recovered from an outbreak of N. fowleri in Arizona (October 2002), from an outbreak of C. jejuni in Wisconsin (January 2001), and from two outbreaks of norovirus in Wyoming (January 2001 and September 2001). All five reports of outbreaks of chemical etiology provided water-quality data. In four of these outbreaks, the contaminant that caused the outbreak was recovered directly from the implicated water, including copper in two outbreaks (Minnesota, November 2001 and Ohio, September 2001), copper and seven other metals in one outbreak (Minnesota, September 2001) and ethyl benzene, toluene, and xylene in one outbreak (Florida, September 2001). The contaminant was not recovered from the tested water in an outbreak (Florida, August 2001) that resulted from ethylene glycol contamination caused by a cross-connection during an improperly performed air-conditioning system repair. However, the sample was collected >24 hours after the contaminating event, and a high degree of clinical suspicion of the contaminating agent existed on the basis of the appearance and smell of the water and on the description of the mechanical error. Water Systems and Water SourcesBecause outbreaks caused by Legionella species are not included in statistics resulting from parameters that describe water systems and water sources, they are excluded from this section. The 25 remaining drinking water outbreaks serve as the focus of these parameters. Seven (28.0%) of these 25 outbreaks were associated with community systems, eight (32.0%) with noncommunity systems, and ten (40.0%) with individual water systems (Tables 6 and 7) (Figure 6). Of the 25 outbreaks, 23 (92.0%) were associated with groundwater sources, including 21 involving wells: one outbreak involved water derived from both a well and spring, and one involved bottled spring water. Two (8.0%) of the 25 outbreaks were associated with surface water that derived from a river or stream. Among the seven outbreaks associated with community water systems, one (14.3%) was caused by contaminated, untreated groundwater; one (14.3%) was related to a treatment deficiency; and four (57.1%) were related to problems in the water distribution system. One (14.3%) community outbreak of an unknown deficiency resulted in 71 cases of illness when participants at a golf tournament consumed contaminated water and ice. The number of illnesses in the other outbreaks varied (range: 2--28). Among the eight outbreaks associated with noncommunity water systems, four (50.0%) were caused by contaminated, untreated groundwater; two (25.0%) were related to treatment deficiencies; one (12.5%) was related to a problem in the water distribution system; and one (12.5%) had an unknown deficiency. Among the 10 outbreaks associated with individual water systems, five (50.0%) were caused by contaminated, untreated groundwater; four (40.0%) were related to treatment deficiencies; and one (10.0%) had an unknown deficiency. These outbreaks affected limited populations (range: 2--13 cases). All three of the bacterial (other than Legionella species) outbreaks occurred in association with groundwater systems (all were untreated wells). Four (80.0%) of the five parasitic outbreaks occurred in association with groundwater systems: two were associated with untreated wells; one occurred after the homeowners intentionally bypassed a reverse osmosis system that had run out of treated water; and one was associated with a distribution deficiency in a treated well/spring combination source. All five viral outbreaks occurred in association with groundwater systems: three were associated with untreated wells; one was related to a treatment deficiency in a chlorinated well; and one had an unknown deficiency. Four (80.0%) of the five chemical outbreaks occurred in association with groundwater systems: three were related to distribution system deficiencies in well water, and one was related to an unknown deficiency in a bottled water product that had a spring as its source. All seven outbreaks of unknown etiology were linked to groundwater systems: four were associated with treatment deficiencies of chlorinated wells, and three were associated with unknown deficiencies in wells (one chlorinated and two untreated). Among the 23 outbreaks related to groundwater systems, 10 (43.5%) were linked to consumption of untreated groundwater, six (26.1%) were associated with treatment deficiencies; four (17.4%) were linked to deficiencies in the distribution system; and three (13.0%) had unknown deficiencies (Table 8). Among the two outbreaks related to surface water systems, one (50.0%) was caused by a treatment deficiency and one (50.0%) by a distribution system deficiency. Outbreaks Caused by Legionella speciesDrinking Water Legionella Outbreaks During 2001--2002, six Legionella outbreaks were related to water systems in which the primary water use at the outbreak site was for drinking (Table 5). These outbreaks caused illness in 80 persons and resulted in 41 hospitalizations and four deaths. The predominant clinical syndrome in all six outbreaks was Legionnaires disease, although in one outbreak involving a government building complex in Vermont (July 2002), six (21.4%) of the 28 ill persons had symptoms consistent with the case definition for Pontiac fever. All of these outbreaks occurred in large buildings or institutional settings and were related to multiplication of Legionella species in the respective distribution systems. Other Legionella Outbreaks One Legionella outbreak was related to a water system in which the primary water use at the outbreak site was recreational (Table 5); this outbreak is discussed elsewhere (8). One Legionella outbreak occurred in an occupational setting and is discussed in the following section. Another Legionella outbreak occurred in Tennessee in April 2002 (32) (Appendix) when patrons of a restaurant experienced Pontiac fever in association with sitting near a particular fountain in the restaurant. Cultures from the fountain were positive for L. anisa. No foods or other exposures were associated with illness, and the restaurant's air conditioning system was negative for Legionella species on laboratory testing. This outbreak caused illness in 117 persons and led to one hospitalization. Outbreaks Associated with Occupational Exposure to WaterTwo outbreaks associated with exposure to water in an occupational setting were reported during 2001--2002. In November 2002, a worker at a wastewater treatment plant in California fell into an equalization basin containing untreated wastewater and subsequently contracted giardiasis. A coworker subsequently experienced gastrointestinal symptoms, although his illness went undiagnosed. In March 2001, an outbreak of Legionnaires disease occurred at an automotive plant in Ohio (33) in which contact with the cleaning area of the plant (particularly one cleaning line) was associated with disease. As a result of this outbreak, 17 persons became ill, two of whom died. Previously Unreported OutbreaksReports of three previously unreported drinking water outbreaks that occurred during 2000 were received during this reporting period (Table 9). An outbreak of cryptosporidiosis occurred in Florida in December 2000 when a groundwater system experienced a main break days before the first of a cluster of five cases of gastrointestinal illness. Cryptosporidium was subsequently identified in a stool specimen from one of these patients. Reports of outbreaks of norovirus (Kansas, June 2000) and cholera (Marshall Islands, December 2000) were also received during this reporting period (Appendix). Outbreaks Not Classified as WBDOsEpidemiologic evidence from four additional outbreaks that were reported as potentially associated with drinking water during 2001--2002 was insufficient to warrant counting these outbreaks as WBDOs. However, because of their potential links to drinking water, a brief description of these outbreaks follows. In June 2002, an outbreak of diarrheal illness occurred among 38 climbers of Mt. Denali in Alaska; illness lasted a mean of 2 days (range: 1--5 days), and the attack rate of climbers was 27% during the 3-day study period. The hypothesized cause was use of fecally contaminated snow as a drinking water source, but this was not associated with illness in a cohort study that was performed during the outbreak. In June 2002, two persons in a Florida household supplied by an untreated well experienced recurring oral lesions and pharyngitis. A third person in the household who did not drink from this water source remained asymptomatic. Although the well water was positive for fecal coliforms, no other epidemiologic evidence linked the drinking water to illness. In June 2002, >77 rafters on the Colorado River in Grand Canyon National Park in Arizona became ill with diarrhea and other gastrointestinal symptoms. Norovirus was isolated from stool specimens of seven (53.8%) of the 13 persons tested. Although norovirus was identified in samples of river water and water from a sewage treatment plant that emptied into the river, these were not the same strains identified in the stool samples. However, a weak association was identified between drinking river water and illness, and no other exposures (e.g., food contamination or asymptomatic carriers) were associated with illness. In April 2000, an outbreak of cholera that sickened approximately 3,500 persons and caused 20 deaths began on Pohnpei Island in the Federated States of Micronesia. No information is available as to the cause of the outbreak or the risk factors for illness. DiscussionConsiderations Regarding Reported ResultsThe WBDO surveillance system provides information concerning epidemiologic and etiologic trends in outbreaks related to drinking water. However, not all outbreaks are recognized, investigated, or reported to CDC or EPA, and studies have not been performed that assess the sensitivity of this system. Furthermore, outbreaks occurring in national parks, tribal lands, or military bases might not be reported to state or local authorities. For these reasons, the true incidence of WBDOs is probably greater than is reflected in surveillance system data. Multiple factors influence whether WBDOs are recognized and investigated by local or state public health agencies, including public awareness of the outbreak, availability of laboratory testing, requirements for reporting diseases, and resources available to local health departments for surveillance and investigation of probable outbreaks. In addition, because changes in the capacity of local and state public health agencies and laboratories to detect an outbreak might result in reporting and surveillance bias, the states with the majority of outbreaks reported during this period might not be the states in which the majority of outbreaks actually occurred. An increase or a decrease in the number of outbreaks reported might reflect either an actual increase or decrease in outbreaks or a change in sensitivity of surveillance practices. As with any passive surveillance system, accuracy of the data depends greatly on the reporting agencies (i.e., state, local, and territorial health departments). Thus, independent of the recognition or investigation of a given outbreak, reporting bias can also influence the final data. Outbreaks most likely to be recognized and investigated are those involving acute illness characterized by a short incubation period, serious illness or symptoms requiring medical treatment, or recognized etiologies for which laboratory methods have become more sensitive or widely available. Increased reporting often occurs as etiologies become better recognized, water system deficiencies are identified, and state surveillance activities and laboratory capabilities increase (34--36). Recommendations for improving WBDO investigations include increased laboratory support for clinical and water analyses, enhanced surveillance activities, and assessment of sources of potential bias (37--39). The identification of the etiologic agent of a WBDO depends on the timely recognition of the outbreak so appropriate clinical and environmental samples can be collected. Additionally, the laboratory involved must have the capability to test for an organism to detect it. For example, routine testing of stool specimens at laboratories include tests for the presence of enteric bacterial pathogens and might also include an ova and parasite examination. However, Cryptosporidium species, among the most commonly reported waterborne pathogens, are often not included in standard ova and parasite examinations and thus should be specifically requested (40). Additionally, although norovirus testing is being performed more commonly, testing for other viral agents is rarely done. Finally, collection of water-quality data depends primarily on local and state statutory requirements, the availability of investigative personnel, and the technical capacity of the laboratories that test the water. One key limitation of the data collected as part of the WBDO surveillance system is that the information collected pertains only to outbreaks of waterborne illness rather than endemic waterborne illness. The epidemiologic trends and water-quality concerns observed in outbreaks might not necessarily reflect or correspond with trends associated with endemic waterborne illness. CDC and EPA have recently completed a series of epidemiologic studies designed to assess the magnitude of endemic waterborne illness associated with consumption of municipal drinking water. A joint report on the results of these studies is forthcoming. Drinking Water Outbreaks Caused by Legionella speciesOf the 31 drinking water-associated outbreaks that occurred during 2001--2002, six (19.4%) were caused by Legionella species, which was the single most commonly identified etiologic agent. Because this is the first time that LD outbreaks have been included in the MMWR Surveillance Summary of WBDOs, no comparative data are available from previous reporting periods. LD outbreaks tended to result in higher morbidity and mortality than the majority of other outbreaks reported (as evidenced by the hospitalization and case-fatality rates) and differed epidemiologically from other drinking water outbreaks. They fit patterns usually seen with Legionella (i.e., they all occurred in large buildings or institutional settings, were related to amplification of Legionella species in the respective distribution systems, and were most likely spread by aerosolization of water from these systems). Contamination of source water is less likely to lead to outbreaks involving this organism. These outbreaks underscore the importance of remaining vigilant about the possibility of Legionella species in any building complex and the need to take measures that address this threat (e.g., maintaining hot water temperatures of >124ºF [return temperature]/>140ºF [storage temperature] and cold water storage and distribution temperatures <68ºF, testing for this organism when outbreaks of respiratory disease or febrile illness occur in these settings, and maintaining adequate disinfectant levels as appropriate) (41,42). Drinking Water Outbreaks (Excluding Those Caused by Legionella species)Because of the different epidemiology of Legionella outbreaks and because LD outbreaks have not been included in previous summaries, they will not be discussed in the following sections, which address the remaining 25 drinking water outbreaks that occurred during 2001--2002. These 25 outbreaks represent a 35.9% decrease from the 39 outbreaks reported during 1999--2000 (2), which was the highest total reported in 8 years (2--7). Seasonality of drinking water outbreaks remained consistent with previous years, with the highest number of outbreaks reported during June--September. The number of reported outbreaks began to decrease sharply beginning with the 1985--1986 reporting period; this was attributable primarily to fewer community and noncommunity outbreaks. With institution and enforcement of better regulations that chiefly affect these types of water systems (particularly community systems), a marked drop in the number of outbreaks was seen. In contrast, the increase in outbreaks reported during 1999--2000 was attributable primarily to individual water systems, which affect fewer persons, are less regulated, and are more subject to changes in surveillance and reporting. The relative proportion of community, noncommunity, and individual outbreaks during 2001--2002 was more consistent with historic norms, as was the total number of outbreaks. During 2001--2002, Florida reported the highest number of outbreaks (eight), as was the case during 1999--2000, when 15 outbreaks were reported. The only other state to report >2 drinking water-associated outbreaks during 2001--2002 was Minnesota, with three outbreaks. Reports of these outbreaks might reflect enhanced surveillance activities rather than a true increase in WBDO incidence; six outbreaks in Florida during 2001--2002 and 14 during 1999--2000 occurred in a single county and were investigated by the same epidemiologist. Among the five most populous states (California, Florida, Illinois, New York, and Texas), only Florida reported >1 drinking water-associated outbreak; California and Texas reported none, and Illinois and New York each reported one. Similarly, in the 2001--2002 summary of recreational water-associated outbreaks (8), Florida and Minnesota reported more recreational water-associated outbreaks than any other state (seven and nine, respectively). This suggests that reporting and surveillance bias might be influencing the number of reports, resulting in considerable year-to-year and state-to-state variation. Surface Water Two (8.0%) of the 25 drinking water-associated outbreaks during 2001--2002 were associated with systems served by surface water (Figure 6), compared with seven (18.4%) during 1999--2000. Among the two surface water-related outbreaks, one was an outbreak of copper poisoning (Ohio, 2001) related to a distribution system deficiency, and one was an outbreak of giardiasis in a rural Colorado town during 2001 caused by the failure of a bag filtration system. The latter outbreak is the first associated with inadequate treatment of surface water to occur in a community system since 1997, when an outbreak of giardiasis associated with disinfected but unfiltered surface water occurred in New York (3). The last community system-associated outbreak related to inadequate filtration of surface water occurred during 1995, when a large outbreak of giardiasis was reported in New York (4). In contrast, during 1991--1994, eight outbreaks (including a substantial outbreak in Milwaukee) were reported in community systems that used treated surface water (5,6). The decrease in outbreaks associated with inadequate treatment of surface water sources is likely attributable to increasingly stringent regulations for treatment of surface water. However, even with the additional EPA regulations, outbreaks might still occur. For example, in addition to the giardiasis outbreak reported in Colorado during 2001, another limited outbreak of giardiasis was reported in a Colorado resort during 1999--2000 (2); this outbreak was attributed in part to defective cartridge filters. The Colorado outbreaks underscore the need for cartridge, bag, and other package filters to meet design specifications and be properly installed if they are to be effective. All filtered systems, no matter what type of filter is employed, should be adequately operated, maintained, and monitored to ensure reliable performance. During 2001--2002, no outbreaks were associated with the direct ingestion of untreated surface water, compared with three outbreaks during 1999--2000. This is encouraging, because keeping the public aware that surface water, despite its clarity, is prone to contamination by pathogens and should not be directly consumed without being treated at the point of use or boiled, remains a priority. Manufacturers of point-of-use devices and the National Sanitation Foundation provide information (available at http://www.nsf.org) regarding different devices, instructions for use, and their ability to make water safe for human consumption. Groundwater Of the 25 outbreaks related to drinking water, 23 (92.0%) were associated with groundwater sources, compared with 28 (73.7%) during 1999--2000 (2). Of the 25 reported outbreaks, 10 (40.0%) were linked to consumption of contaminated, untreated groundwater. During 1999--2000, a total of 17 (44.7%) of 38 outbreaks were associated with contaminated, untreated groundwater sources. Although outbreaks caused by the use of untreated groundwater decreased during 2001--2002, the largest proportion of groundwater outbreaks during this period remained attributable to untreated water systems, and untreated groundwater remains a primary cause of outbreaks, especially in private, individual water systems that are not regulated by EPA. During both the current and pervious reporting periods, half of the outbreaks attributed to untreated groundwater were reported in individual water systems. Treated groundwater systems can also lead to outbreaks; six (24.0%) of the 25 outbreaks during 2001--2002 were associated with treatment deficiencies of groundwater systems (including one outbreak in which treatment was bypassed), compared with eight (21.1%) during 1999--2000. Four (66.7%) of the six outbreaks associated with treated groundwater during 2001--2002 were reported in individual rather than public systems, compared with one outbreak (14.3%) during 1999--2000. To safeguard the quality of their well water, homeowners should purchase appropriately designed point-of-use devices and follow instructions for operating and maintaining these treatment devices. Public health agencies can help by providing educational materials about effective water treatment devices for private, individual water systems. Although individual groundwater systems are not regulated by EPA, and public groundwater systems (other than systems influenced by surface water) are not required to filter or disinfect drinking water, efforts should continue to identify and remove possible sources of contamination and provide adequate, continuous treatment for those systems that need treatment. Wells and springs must be protected from contamination even if disinfection is provided, as groundwater can become contaminated with pathogens that might overwhelm the disinfection process. EPA's proposed GWR (information available at http://www.epa.gov/safewater/gwr.html) is expected to establish multiple barriers in groundwater systems to protect against pathogens in drinking water from groundwater sources and should establish a targeted strategy to identify groundwater systems at high risk for fecal contamination. The multiple barrier approach should begin with protection of the wellhead, an assessment of potential sources of contamination, and periodic sanitary surveys to ensure that wells remain protected. Periodic monitoring of source water is necessary to identify water-quality deterioration, and adequate, continuous water treatment is needed for wells that are identified as being vulnerable. Of the 22 well-related outbreaks that occurred during 2001--2002, a total of 13 (59.1%) were associated with community or noncommunity wells, compared with nine (40.9%) that were associated with individual wells not covered by EPA regulations. This distribution, similar to previous reporting periods, is notable because only public water systems will be directly affected by GWR, and thus protections offered by GWR might not extend to individual groundwater systems. The quality of water in private wells and springs used by private persons and nonpublic systems thus remains a public health concern; approximately 17 million persons in the United States rely on private household wells for drinking water each year, and >90,000 new wells are drilled annually throughout the United States (43). In addition, contamination of a private well is not only a health concern for the household served by the well but can have an impact on households using other nearby wells that draw from the same aquifer. EPA does not regulate private wells and will not do so as part of the proposed GWR. EPA recommendations for protecting private water supplies are available at http://www.epa.gov/safewater/pwells1.html. Additional efforts should be taken to educate well owners, users, well drillers, and local and state drinking water personnel to encourage practices that best ensure safe drinking water for private well users. Deficiencies During 2001--2002, the number of outbreaks associated with each different type of deficiency (untreated surface water, untreated groundwater, treatment deficiency, distribution system deficiency, and unknown/miscellaneous deficiency) decreased from levels reported during 1999--2000. In addition, each deficiency type represented a similar proportion of the total number of drinking water outbreaks reported during 1999--2000. Water Systems During 2001--2002, the number of outbreaks associated with each of the three different types of water systems also decreased compared with 1999--2000 (Figure 6), whereas the proportion associated with each type remained relatively consistent. The number of outbreaks associated with individual systems decreased from 17 during 1999--2000 to 10 during 2001--2002, but still remained the most common of the three. Of the eight outbreaks reported from Florida (the state with the most reported outbreaks, possibly reflecting enhanced surveillance in that state), seven involved individual groundwater systems (the eighth involved a community well system), which might have biased the results toward more individual (as well as more groundwater) outbreaks; this again potentially demonstrates that outbreaks involving individual water systems are the most susceptible to detection bias, given the limited number of persons involved, the different levels of resources available to investigate these outbreaks, and the limited number of regulations that govern these systems. The number and proportion of outbreaks attributed to individual systems during 1999--2000 was at a 15-year high and accounted for much of the overall increase in the number of outbreaks reported during 1999--2000. The decline in outbreaks attributed to individual systems makes the number and proportion of outbreaks associated with each type of water system more comparable with reporting periods during the 1990s. Etiologic Agent The etiologic agent was not identified in seven (22.6%) of the 31 outbreaks reported during 2001--2002 (Figure 6). Although these seven outbreaks comprised the largest group of outbreaks, this was a marked decrease from the number (17) and percentage (43.6%) of outbreaks of unknown etiology during 1999--2000. This likely reflects both the improved diagnostic capability of laboratories and better outbreak investigations, resulting in more rapid and more appropriate specimen collection. Viral outbreaks (five) comprised 16.1% of the total, an increase from the previous reporting period. This likely reflects rapidly improving diagnostic capability for detecting norovirus in stool samples, a hypothesis supported by the fact that all five viral outbreaks were caused by this agent. The five norovirus outbreaks affected by far the most persons (727) of any single etiologic agent and caused more illness than all other agents combined. Parasitic outbreaks (five) also comprised 16.1% of the total, similar to previous years. Among the parasitic outbreaks, two linked cases of N. fowleri infection occurred in Arizona during October 2002, resulting in two deaths; this was the first report of an outbreak of N. fowleri in the United States related to a drinking water system (Appendix). This outbreak further underscores the need for treatment of groundwater, particularly in geothermal areas in which these thermophilic amebae are likely to be amplified. Chemical outbreaks (five) also comprised 16.1% of the total, an increase from the previous reporting period; these outbreaks highlight the importance of proper maintenance of water systems, because four of the five resulted directly from errors related to either recent maintenance work or to an improperly installed device. Bacterial outbreaks (three) comprised 9.7% of the total, a decrease compared with the previous reporting period and the lowest number reported since 1991--1992. ConclusionData collected as part of the national WBDO surveillance system are used to describe the epidemiology of waterborne diseases in the United States. Trends regarding water systems and deficiencies implicated in these outbreaks are used to assess whether regulations for water treatment and monitoring of water quality are adequate to protect the public's health. Identification of the etiologic agents responsible for these outbreaks is also critical because new trends might necessitate different interventions and changes in policies and resource allotment. Surveillance for waterborne agents and outbreaks occurs primarily at the local and state level. Local and state public health authorities should be able to detect and recognize drinking water-associated outbreaks and implement appropriate prevention and control measures. Improved communication among local and state public health departments, regulatory agencies, water utilities, and recreational water facilities would aide the detection and control of outbreaks. Routine reporting or sharing of water-quality data with the health department is recommended. Other means of improving surveillance at the local, state, and federal level might include the additional review and follow-up of information gathered through other mechanisms (e.g., issuances of boil-water advisories or reports of illness associated with agents thought to be waterborne). State health departments can request epidemiologic assistance and laboratory testing from CDC to investigate WBDOs. CDC and EPA can be consulted regarding engineering and environmental aspects of drinking water and recreational water treatment and regarding collection of large-volume water samples to identify pathogenic viruses and parasites, which require special protocols for their recovery. Requests for tests for viral organisms should be made to CDC's Viral Gastroenteritis Section, Respiratory and Enterovirus Branch, Division of Viral and Rickettsial Diseases, National Center for Infectious Diseases (NCID), at 404-639-3577. Requests for information or testing for Legionella should be made to CDC's Respiratory Diseases Branch, Division of Bacterial and Mycotic Diseases, at 404-639-2215. Requests for tests for parasites should be made to CDC's Division of Parasitic Diseases, NCID, at 770-488-7756. Additional information is available from
AcknowledgmentsThe authors thank the following persons for their contributions to this report: state waterborne-disease surveillance coordinators; state epidemiologists; state drinking water administrators; Robert Tauxe, M.D., Matt Moore, M.D., Barry Fields, Ph.D., Rachel Woodruff, M.P.H., Division of Bacterial and Mycotic Diseases, NCID, CDC; Marc-Alain Widdowson, M.A., Vet.M.B., M.Sc., Division of Viral and Rickettsial Diseases, NCID, CDC; Matthew Arduino, Dr.P.H. Joe Carpenter, Division of Healthcare Quality and Promotion, NCID, CDC; Mark Eberhard, Ph.D., James Maguire, M.D., Adria Prosser, Ph.D., Division of Parasitic Diseases, NCID, CDC; Lorraine Backer, Ph.D., Mark McClanahan, Ph.D., Division of Environmental Hazards and Health Effects, NCEH, CDC. References
* Composed of the Republic of the Marshall Islands, the Federated States of Micronesia, and the Republic of Palau; formerly parts of the U.S.-administered Trust Territory of the Pacific Islands. † Additional terms are defined in the Glossary. Table 1 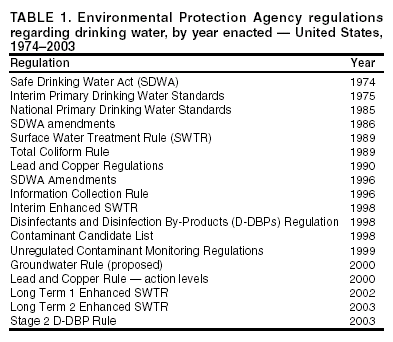 Return to top. Figure 1 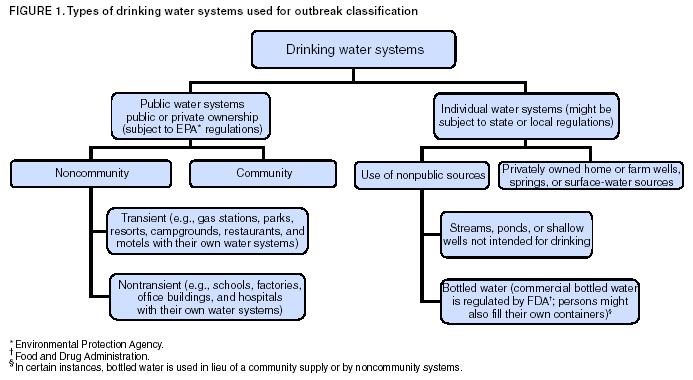 Return to top. Table 2 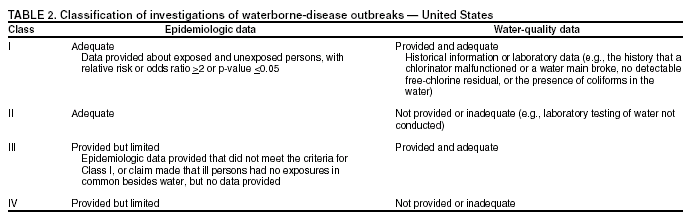 Return to top. Figure 2 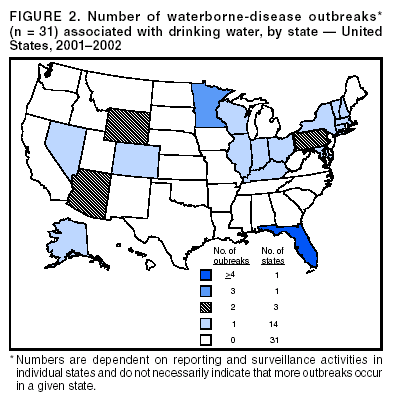 Return to top.
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to [email protected].Page converted: 10/13/2004 |
|||||||||
This page last reviewed 10/13/2004
|