Corresponding author: Deborah Lee, MPH, Division of Global Migration and Quarantine, National Center for Emerging and Zoonotic Infectious Diseases. Telephone: 404-639-0439; E-mail: [email protected].
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail.
Disease Surveillance Among Newly Arriving Refugees and Immigrants — Electronic Disease Notification System, United States, 2009
Abstract
Problem/Condition: Approximately 450,000 legal permanent immigrants and 75,000 refugees enter the United States annually after receiving required medical examinations by overseas panel physicians (physicians who follow the CDC medical screening guidelines provided to the U.S. Department of State). CDC has the regulatory responsibility for preventing the introduction, transmission, and spread of communicable diseases into the United States as well as for developing the guidelines, known as technical instructions, for the overseas medical examinations. Other conditions that are not infectious might preclude an immigrant or refugee from entering the United States and also are reported as part of the medical examination. After arrival in the United States, all refugees are recommended to obtain a medical assessment by a health-care provider or a health department within 30 days. In addition, immigrants with certain medical conditions such as noninfectious tuberculosis at the time of the original medical examination are recommended to be evaluated after arrival to ensure that appropriate prevention or treatment measures are instituted. Health departments need timely and accurate notifications of newly arriving immigrants, refugees, and persons with other visa types to facilitate these evaluations. Notifications for all newly arriving refugees (with or without medical conditions) and immigrants with medical conditions are provided by CDC's Electronic Disease Notification (EDN) system. This is the first report describing EDN.
Reporting Period: This report summarizes notifications by the EDN system during January–December 2009.
Description of System: The EDN system is a centralized electronic reporting system that collects health information on newly arriving refugees and immigrants with Class A and Class B medical conditions. Class A conditions render applicants inadmissible and require a waiver for entry; Class B conditions are admissible but might require treatment or follow-up. Information in the EDN system is used to notify state health departments in all 50 states and the District of Columbia about the arrival of these persons in the United States.
Results: In 2009, the EDN system notified U.S. state and local health departments of 104,954 newly arriving refugees and immigrants, of whom 78,899 (75.2%) were refugees (with or without medical conditions), 19,358 (18.4%) were immigrants with medical conditions, and 6,697 (6.4%) were persons with other visa types. Of the 78,899 refugees, 21,319 (27%) had a medical condition. The majority (93.4%) of immigrants with medical conditions had tuberculosis classifications (i.e., either had evidence of latent tuberculosis infection or chest radiograph findings interpreted by the overseas panel physician as consistent with tuberculosis). Of the 41,415 refugees and immigrants with Class A or Class B medical conditions, 405 (1%) had Class A conditions, and 40,994 (99%) had Class B conditions. The majority of refugees and immigrants with suspected Class B tuberculosis were born in the Philippines (41.3%), Mexico (12.1%), Burma (8.7%), Vietnam (7.8%), and the Dominican Republic (5.8%). The majority of refugee notifications were for persons born in Iraq (23.9%), Burma (18.9%), and Bhutan (15.1%). Approximately one third of the tuberculosis notifications were sent to health departments in California (20.5%), Texas (9.8%), and New York (6.3%), and the national reporting rate for tuberculosis follow-up was 75.4% within 30 days of arrival.
Interpretation: The findings in this report suggest that 1) overseas medical screening results in a low frequency (0.4%) of inadmissible medical conditions in the United States, 2) the EDN system provides more direct notifications to health departments than the previous paper-based system about newly arriving immigrants and refugees who need medical follow-up, and 3) approximately 75% of follow-up occurs among persons with suspected tuberculosis who are reported to EDN by states receiving newly arriving refugees and immigrants.
Public Health Actions: The data in this report can be used to help state and local health departments provide prompt and effective follow-up, evaluation, and treatment to newly arriving immigrants and refugees. Timely follow-up might prevent additional spread of tuberculosis or other communicable diseases of public health significance into their communities. In addition, information from the EDN system allows health departments to use their resources as effectively as possible by providing clinical information that identifies the refugees and immigrants who should be prioritized for evaluation and treatment.
Background
Approximately 75,000 refugees and 450,000 legal permanent immigrants enter the United States annually (1). Immigrants and refugees coming to the United States are required to have a medical examination by the U.S. Department of State (DOS) and the U.S. Department of Homeland Security (DHS) to identify applicants with health conditions that render them inadmissible. The Secretary of the U.S. Department of Health and Human Services (HHS) has the statutory responsibility for preventing the introduction, transmission, and spread of communicable diseases into the United States (42 U.S. Code 264). Under the authority of the Immigration and Nationality Act (8 U.S. Code 1182 and 1222) and the Public Health Service Act (U.S. Code 252), CDC outlines the requirements for the overseas medical examination of immigrants and refugees seeking admission into the United States. CDC provides DOS and DHS with the medical screening guidelines used by approximately 700 overseas examining physicians (2), who are referred to as panel physicians (42 CFR Part 34). The medical examination determines whether the applicant has a Class A condition (inadmissible condition) or Class B condition (admissible condition). Class A conditions include 1) a communicable disease of public health significance, 2) lack of documentation for certain vaccinations, 3) a physical or mental disorder with associated harmful behavior, or 4) drug abuse or addiction. Class B conditions are health-related conditions that are admissible but that might require extensive medical treatment or follow-up. Applicants with a Class A condition can enter the United States only if they are granted a waiver. The guidelines that outline the overseas screening requirements for these communicable diseases are provided by CDC in documents called technical instructions (3,4). (Information on medical examination requirements for various types of immigrant visas is available at http://travel.state.gov/visa/immigrants/immigrants_1340.html.)
Under the authority of the Immigration and Nationality Act (8 U.S. Code 1522), CDC has the regulatory responsibility to ensure that state or local health officials at the U.S. resettlement destination of each refugee are notified promptly of the refugee arrivals and provided all applicable medical records. After entry into the United States, all refugees are recommended to undergo a medical assessment by a U.S. health department or a health-care provider within 30 days of arrival (Immigration and Nationality Act, Sect. 412, or Refugee Act of 1980, 8 U.S. Code 1522[b]). Immigrants with medical conditions that require follow-up, such as noninfectious tuberculosis and other conditions specified by the panel physician, are recommended to be evaluated after arrival to ensure appropriate follow-up and prevention measures.
In the United States, the incidence of tuberculosis is 12 times greater among foreign-born persons than among U.S.-born persons (5). Tuberculosis is challenging to diagnose, treat, and control; the medical screening for tuberculosis among immigrants and refugees who apply for entry to the United States is an essential component of the overseas medical evaluation. The identification of and follow-up for immigrants and refugees with noninfectious tuberculosis is an important public health control measure to prevent the spread of tuberculosis in the United States.
CDC sends notifications to state and local public health authorities when all refugees and immigrants with conditions of public health significance enter the United States and arrive in their jurisdiction. In March 2006, CDC established the Electronic Disease Notification (EDN) system to facilitate these notifications, which are used to identify new arrivals who require follow-up. This is the first report describing the EDN system, including its methods and results during January–December 2009, the first year with enough data to conduct a meaningful analysis. The findings in this report are intended to provide guidance for the medical examination of immigrants and refugees, create evidence-based recommendations that can protect the health of newly arriving immigrants and refugees, and prevent the spread of disease in U.S. communities.
Methods
Definitions of Immigrants, Refugees, and Persons with Other Visa Types
- Immigrants. Immigrants, also described as legal permanent immigrants or lawful permanent residents, are persons who are not citizens of the United States but who live in the United States under a legally recognized and lawfully recorded permanent residence as an immigrant.
- Refugees. Refugees are persons who are unable or unwilling to return to their country of nationality because of persecution or a well-founded fear of persecution due to race, religion, nationality, membership in a particular social group, or political opinion (Immigration and Nationality Act, Sect. 101[a][42]). Each fiscal year, the U.S. government sets an overall refugee admissions limit based on regional allocations. The limit for refugee admissions in 2009 was 80,000 (1). In 2009, Iraqis and Afghans with special immigrant visas who were eligible for refugee benefits (6,7) were classified under the refugee visa type in the EDN system. During that year, 78,899 persons were admitted as refugees, primarily from Iraq (18,838), Burma (18,202), and Bhutan (13,452) (1).
- Asylees. Asylees are foreign persons who are unable or unwilling to return to their country of nationality or who seek protection in the United States because of persecution or a well-founded fear of persecution. Available asylee records were classified as other visa types. In addition, asylees are already in the United States or are seeking admission at a port of entry. (Additional informatation available at http://www.uscis.gov.)
- Parolees. Parolees are foreign persons allowed into the United States for urgent humanitarian reasons or when that person's entry is determined to be for significant public benefit. Available parole records were classified as other visa types.
Overseas Medical Examination
Each refugee or immigrant who enters the United States must undergo a medical examination in their country of origin. These legally required medical examinations identify persons with inadmissible conditions of public health significance before they enter the United States. The examinations are conducted by panel physicians, who are medically trained, licensed, and experienced physicians practicing overseas who are appointed by the local U.S. embassy or consulate and who follow the CDC medical screening guidelines provided to DOS and HHS. Certain panel physicians who examine U.S.-bound refugees work within the International Organization for Migration (IOM), which assists with refugee-related responsibilities such as migration management and movement (8). The panel physicians record the results of the medical examination on DOS forms that document the health information obtained during the medical examination of immigrants and refugees bound for the United States. The forms include the following:
- Medical Examination of Immigrant or Refugee Applicant (DS-2053 or DS-2054),
- Chest X-Ray Classification Worksheet (DS-3024 or DS-3030),
- Vaccination Documentation Worksheet (DS-3025), and
- Medical History and Physical Examination Worksheet (DS-3026).
(Information about obtaining these forms is available from DOS at http://www.travel.state.gov/visa/visa_1750.html.) Data from the Vaccination Documentation (DS-3025) and Medical Health and Physical Examination Worksheet (DS-3026) are not included in this report because they were incomplete in 2009.
Class A and Class B Conditions
The medical examination determines whether the applicant has an inadmissible condition of public health significance (a Class A condition) or has a health-related condition that is admissible but that might require extensive medical treatment or follow-up (a Class B condition) (Box). Applicants with Class A (inadmissible) conditions can only enter the United States if they are granted a waiver. Applicants who have Class A conditions include those who 1) have a communicable disease of public health significance, 2) do not have documentation of having received vaccinations against vaccine-preventable diseases, 3) have a physical or mental disorder with associated harmful behavior, or 4) abuse or are addicted to drugs. (42 USC 252, 8 USC 1182, and 8 USC 1222 provide for the physical and mental examination of applicants in accordance with regulations prescribed by the HHS Secretary.) The communicable diseases of public health significance include tuberculosis, syphilis, chancroid, gonorrhea, granuloma inguinale, lymphogranuloma venereum, Hansen disease (leprosy), and the following two disease categories: 1) quarantinable diseases designated by a presidential executive order (as provided under Sect. 361[b] of the Public Service Health Act), which include cholera, diphtheria, infectious tuberculosis, plague, smallpox, yellow fever, viral hemorrhagic fevers, severe acute respiratory syndrome (SARS), and influenza caused by novel or reemergent influenza viruses, and 2) events or conditions that are reportable as a public health emergency of international concern to the World Health Organization under the International Health Regulations of 2005 (polio, smallpox, SARS, influenza, and other public health emergencies of international concern) (9).
A Class B condition (Box) is a physical or mental disorder that, although not precluding persons from entering the United States, represents a departure from normal health or well-being that is significant enough to possibly interfere with the ability to care for oneself or to attend school or work or that might require extensive medical treatment or institutionalization in the future. These significant health problems must be brought to the attention of U.S. consular officials in the country where the applicant resides; persons with a Class B condition are recommended for medical follow-up when they arrive in the United States.
Screening for Tuberculosis
According to an agreement with the consular section of the embassy or consulate in the originating country, panel physicians conduct the medical examination for immigrants and refugees bound for the United States using specific criteria outlined by CDC in technical instructions. Two versions of the tuberculosis technical instructions are in use. Immigrants and refugees bound for the United States are examined in accordance with either the 1991 technical instructions (10) or the culture and directly observed therapy (CDOT) version of the tuberculosis technical instructions (which were released in 2007 and are being implemented in a phased approach) (11).
The tuberculosis technical instructions are designed to detect and treat tuberculosis disease among applicants to reduce the risk for spread of tuberculosis among the U.S. population after immigration. Studies found that the 1991 tuberculosis screening requirements lacked the sensitivity to detect persons with tuberculosis who had negative acid-fast bacillus sputum smear results but sputum culture results that were positive for Mycobacteria tuberculosis. In addition, the 1991 tuberculosis technical instructions did not prevent importation of multidrug-resistant tuberculosis into the United States (12,13). In 2007, the tuberculosis technical instructions were updated to require sputum cultures and drug-susceptibility testing for persons with suspected tuberculosis based on WHO data for immigration patterns and countries with a high prevalence of tuberculosis (11) and also to require directly observed therapy for persons found to be infected. As of July 2013, CDOT had been implemented in 117 countries (11). Implementation was prioritized based on the country's number of U.S. immigrants, the number of refugees resettling to the United States, tuberculosis rates, and tuberculosis rates in immigrant groups in the United States (4). By October 1, 2013, all U.S. panel physicians will be required to screen according to the CDOT tuberculosis technical instructions (http://www.cdc.gov/panelphysicians/index.html).
1991 Tuberculosis Technical Instructions for Tuberculosis Screening and Treatment
The 1991 technical instructions (10) require applicants aged ≥15 years to have chest radiography and to provide three sputum smears for acid-fast bacillus microscopy if the chest radiograph findings suggest active tuberculosis. Before traveling to the United States, applicants who have positive sputum smear results must undergo treatment until their sputum smear results are negative or they are granted a Class A waiver; the therapy they should receive is not specified (Table 1).
CDOT Technical Instructions for Tuberculosis Screening and Treatment
In the CDOT tuberculosis technical instructions, which were released in 2007, CDC updated the panel physician screening algorithms to increase sensitivity for active tuberculosis and prevent importation of multidrug-resistant tuberculosis (3). Applicants with chest radiograph findings that are suggestive of tuberculosis are required to submit three sputum specimens to undergo microscopy for acid-fast bacilli and culture for mycobacteria; drug-susceptibility testing is required on positive cultures. Persons with a positive culture or positive smear must complete treatment according to American Thoracic Society/CDC/Infectious Diseases Society of America guidelines, with medications delivered as directly observed therapy (11), before immigrating to the United States.
Medical Waivers
A provision of the Immigration and Nationality Act allows eligible applicants with a Class A (i.e., inadmissible) condition to apply for a waiver. Without this waiver, persons with Class A conditions cannot enter the United States. During 2009, waivers were available for Class A applicants with HIV infection, active pulmonary or laryngeal tuberculosis undergoing treatment, or a physical or mental disorder with associated harmful behavior. According to CDOT technical instructions, all applicants with pulmonary or laryngeal tuberculosis disease who need treatment overseas must complete directly observed therapy (DOT) by a trained health-care worker before immigration to the United States. Health-related waiver applications are submitted by individual applicants to the U.S. Citizenship and Immigration Services (USCIS), a DHS agency. Before USCIS grants a waiver, CDC reviews the health-related waiver applications and supporting medical documentation to ensure that the applicant has been classified properly and that an appropriate U.S. health-care provider has been identified who agrees to evaluate the applicant within 30 days of arrival in the United States. DHS and USCIS make the final approval or denial of the waiver request (14).
The EDN System
The EDN system is a centralized electronic reporting system that collects health information on all newly arriving refugees and newly arriving immigrants with Class A or B medical conditions. Information in the EDN system is used to notify state health departments in all 50 states and the District of Columbia (DC) about these arrivals. The objectives of EDN are to 1) provide timely and accurate medical notifications to U.S. health departments of all newly arriving refugees and immigrants with health conditions that might require follow-up; 2) monitor diseases of public health significance, such as tuberculosis; and 3) provide data for evidence-based recommendations to the U.S. and international public health communities, as well as to federal partners.
Before 2008, using the existing paper-based notification system to conduct surveillance for Class A or Class B conditions adequately was challenging. Notifications of immigrants with medical conditions and all refugee arrivals (regardless of medical status) were sent by CDC through the U.S. Postal Service to state and local health departments. Some notifications were lost, others were not received, and documentation of the overseas medical examinations was not consistently available, leading to the additional expenses of repeated chest radiography and vaccinations. To address these issues, in March 2006, the EDN system pilot programs were implemented at three of the 20 CDC quarantine stations (15) (Atlanta, Miami, and New York City), covering ports of entry in 12 destination states. Documents were entered electronically into the EDN system for some of the arrivals coming through these quarantine stations. Following the successful pilot, EDN became fully functional and completely replaced the paper-based notification system, allowing electronic notification by e-mail of arrivals at all 20 quarantine stations by October 2008. On October 1, 2008, the EDN system was designated as the primary method to notify health officials of all newly arriving refugees and immigrants with Class A and Class B medical conditions or with HIV infection. These notifications were sent through EDN to tuberculosis and refugee health coordinators in U.S. state and local health departments in all 50 states and DC.
To collect the data for EDN, CDC collaborates closely with federal and international partners to compile accurate medical examination data. Medical documents for all refugees and immigrants entering the United States are collected by U.S. Customs and Border Protection (CBP) at U.S. ports of entry. CBP sends the documents to the quarantine station in charge of that port of entry into the United States (information available at http://www.cdc.gov/quarantine/QuarantineStations.html). Each quarantine station obtains the information for all refugees and immigrants with Class A and B medical conditions. Information collected by the CDC quarantine station staff includes health indicators that are derived from DOS medical examination forms. These include Class A and B conditions; current general physical examination; vaccination history; chest radiography results; and past medical history related to cardiology, pulmonology, neurology, psychiatry, endocrinology, and sexually transmitted diseases.
Flow of Information
After the panel physician in the originating country conducts the medical screening examination, all refugees and immigrants with medical conditions are given a copy of the completed medical examination form (Figure 1). Officials from CBP collect these completed forms at the ports of entry and provide a copy to the officials at the CDC quarantine station that has jurisdiction over the port of entry (15). Within 24–48 hours, the officials at the quarantine station send the forms via courier to the CDC EDN data entry center in Atlanta, Georgia (rather than to multiple health departments), where the forms are scanned and entered manually into the EDN system. Once the records are in the EDN system, an electronic notification is sent via e-mail. Health departments can access the scanned forms for clinical use or download electronic data sets for analysis (Figure 1).
Immigrants and other visa groups, such as asylees and parolees, might arrive in any of the approximately 300 official points of entry (16). In contrast, refugees enter the United States through one of five points of entry: 1) John F. Kennedy International Airport (New York City, New York), 2) Newark Liberty International Airport (Newark, New Jersey), 3) Chicago O'Hare International Airport (Chicago, Illinois), 4) Miami International Airport (Miami, Florida), and 5) Los Angeles International Airport (Los Angeles, California). Refugee arrivals are managed by the DOS Bureau of Population and Refugee Migration through the International Organization for Migration (IOM). Within 24 hours of arrival, approximately 65% of all refugee medical records are transmitted to EDN from IOM's Migrant Management and Operational Systems Application (MiMOSA) (17) database using the Public Health Information Network Messaging System (18) interface. Before these electronic refugee records are made available on the EDN system, staff members at the data entry center compare them with the corresponding scanned document for any discrepancies, such as incorrect classifications or incomplete records. All other records are entered manually from the copies received from quarantine stations.
EDN System Data Analysis
To describe the number and type of Class A or B conditions among all newly arriving refugees (with or without Class A or B conditions) and among newly arriving immigrants (with Class A or B conditions), CDC analyzed EDN data for 2009 (the first year with adequate and complete data to allow for meaningful analysis). The analysis was stratified by type of visa (refugees, immigrants with medical conditions, and other, which included asylees, parolees, and unknown). Because overseas medical records for immigrants without Class A or B medical conditions are not collected in the EDN system, analysis of the total population of immigrant arrivals (i.e., approximately 400,000 immigrant records) is not possible. In contrast, the EDN system collects overseas medical records for refugees both with and without Class A or B medical conditions. Variables analyzed included birth country, sex, age group, number of arrivals or medical records received by quarantine stations, destination state or area, number of days until health departments were notified of arrivals, and tuberculosis classification.
Notifying Health Departments of Arriving Immigrants with Class A and B Medical Conditions and of All Refugees
Within approximately 2 weeks of arrival, all state health departments and CDC are notified about all refugee arrivals and of immigrants with Class A or B conditions (primarily tuberculosis and HIV) by an e-mail from EDN indicating that new or changed information is available. Notification of arrivals with tuberculosis classifications to U.S. territories such as Puerto Rico, the U.S. Virgin Islands, and the U.S. Pacific Islands is coordinated by CDC quarantine stations and local health departments. EDN, which is accessed through a secure website, allows permitted users to see a list of specific new arrivals, including those who have been classified with suspected tuberculosis and recommended follow-up. Before January 2010, refugees and immigrants with HIV infection were classified as having a Class A condition; medical information for refugees and immigrants with Class A HIV and the required waiver were mailed via courier to the listed primary health-care provider. Class A HIV notifications are included in this report. On January 4, 2010, HIV infection was removed from the list of inadmissible conditions for immigration purposes, and HIV testing is no longer required as part of the immigrant medical examination (19).
Contact information for refugees who might have been exposed (during the incubation period) to a communicable disease such as measles or varicella is compiled from the EDN system and provided to state and local health departments via Epi-X, a CDC-managed secure communication system for public health professionals (20).
Tuberculosis Follow-Up Reporting by States
State and local health departments are asked to complete tuberculosis follow-up evaluations of persons with tuberculosis classification in the EDN system. The tuberculosis follow-up evaluation form was expanded from the CDC form 75.17 (2) to include additional testing conducted during the U.S. medical evaluation, such as a skin test, radiology, microscopy, and bacteriology, as well as treatment.
State health departments can access the health information from overseas medical examinations in an electronic analyzable format and as a scanned copy of the paperwork for all refugee arrivals and immigrants with tuberculosis through the secure EDN website. When an immigrant or refugee moves to another state, records are reassigned to the new state, and a notification is sent to the state tuberculosis coordinator so that follow-up activities can be completed.
Analysis
This report includes a summary of the first report from the EDN system, including the number of newly arriving refugees, immigrants with medical conditions, and persons of other visa types whose information was collected at CDC quarantine stations, and the number of notifications by birth country, U.S. local health departments by birth country, (Class A or B medical condition), and suspected tuberculosis classification. Also provided is the number of persons who received follow-up because of a suspected tuberculosis classification that was reported into the EDN system by U.S. health departments. Other notifications of communicable diseases that occurred in 2009 are summarized. This report does not include overseas vaccination and medical history information because this information was incomplete for 2009.
Results
EDN System Data
EDN provided access to overseas medical examinations that were reported to CDC quarantine stations (Table 2). During 2009, the CDC EDN system notified 438 tuberculosis controllers and refugee health coordinators in 223 U.S. state and local health departments (Figure 2) in all 50 states and DC of 104,954 arrivals, including 19,358 (18.4%) immigrants with medical conditions of public health significance, 78,899 refugees with or without medical conditions (75.2%), and 6,697 (6.4%) applicants with other visa types (with or without medical conditions). Of the 78,899 total refugees arrivals, 21,319 (27%) had a medical condition. The New York John F. Kennedy International Airport was the entry point for the largest proportion (39%) of refugees. Medical examinations of immigrants with medical conditions were collected at all 20 quarantine stations, of which Los Angeles, California, collected the most (21.6%).
At the start of January 2009, the median number of days from arrival to notification was 39 days, with a high of 81 days in March 2009 (Figure 3). During October–December 2009, after full EDN implementation, the median number of days from arrival to notification decreased to 14 days.
Notifications by Birth Country
In 2009, the EDN system generated notifications for arrivals from 174 birth countries (Table 3). The three most common countries of birth for refugees were Iraq (18,897 [23.9%]), Burma (14,951 [18.9%]), and Bhutan (11,898 [15.1%]). The majority of refugees and immigrants with suspected Class B tuberculosis were born in the Philippines (9,642 [41.3%]), Mexico (2,828 [12.1%]), Burma (2,033) [8.7%]), Vietnam (1,830 [7.8%]), and the Dominican Republic (1,352 [5.8%]) (Table 4). The proportion of female arrivals overall was 49.5% and was not significantly different within age groups (<15 years, 49.2%; 15–44 years, 48.3%; and ≥45 years, 52.3%). Overall, the percentage of notifications received was highest among persons aged 15–44 years.
Notifications to U.S. Health Departments
California's 58 county health departments received notifications for 36.1% of all immigrants with medical conditions of public health significance and 14.3% of all refugees, for a total of approximately 20% of EDN notifications during 2009 (Table 5). Texas and New York received the second- and third-highest proportion of notifications both for immigrants with medical conditions (6.7% and 7.8%, respectively) and all refugee arrivals (11.1% and 6.2%, respectively). Montana and Wyoming received no notifications of refugee arrivals.
Notifications of Class A and B Medical Conditions
Of 41,415 notifications of Class A and B medical conditions, 405 (1%) were for Class A and 40,994 (99%) were for Class B medical conditions (Table 6). Of the 405 Class A medical conditions, approximately 90% were for arrivals with waivers who tested positive for HIV infection during the medical examination; the U.S. health-care provider who agreed to care for the HIV-positive person was notified by mail. Of the 40,994 Class B medical conditions, 56.8% were from persons classified with noninfectious tuberculosis. Other than tuberculosis, the two most frequently identified Class B medical conditions were any physical or mental disorder (unlikely to recur) (1.9%) and pregnancy (1.8%).
Notifications of Immigrants and Refugees with Tuberculosis Classifications
All 50 states and DC received notifications of arrivals with tuberculosis classifications (Figure 4). California (7,006 [30%]), New York (1,885 [8.1%]), and Texas (1,872 [8%]) received the most tuberculosis notifications (Table 7). Most (84%) of these notifications were for persons born in the 28 countries that had implemented the CDOT tuberculosis technical instructions by the end of 2009 (21). Of these 28 countries, 13 (46.4%) had implemented the CDOT tuberculosis technical instructions for all applicants bound for the United States, and four (14.3%) had implemented them for refugees before 2009. Overall, a median of 75.4% of persons received follow-up for suspected tuberculosis classifications that were reported into the EDN system by the U.S. health departments. Thirty-three states reported following up with 65%–100% of arrivals with a suspected tuberculosis classification. Among the notifications for tuberculosis, only 10 (0.02%) were for persons with Class A tuberculosis who received waivers; these notifications were sent to seven states (Table 6), and all were among immigrants. Among persons classified as having Class B tuberculosis, 6,257 (26.8%) were classified by using 1991 tuberculosis technical instructions, and 16,828 (72.0%) by the 2007 CDOT tuberculosis technical instructions (Table 8).
Notifications of Disease Outbreaks
EDN can provide data rapidly that can be used to locate refugees who might have been exposed to a disease outbreak overseas before their arrival at their U.S. destinations. During 2009, state and local health departments were notified of four outbreaks of suspected varicella among refugee children. Before their departure for the United States, some of these children might have been exposed to varicella in transit centers overseas (transit center 1, January 30, 2009; transit center 2, February 2, 2009; transit center 3, March 23, 2009; transit center 4, May 4, 2009), The U.S. contact information of each refugee who might have been exposed during the outbreak was compiled immediately by CDC from the EDN system and provided to state and local health departments for follow-up via Epi-X, a CDC-managed secure communication system for public health professionals (20).
Discussion
The U.S. Public Health Service has provided the guidance for the medical examination of immigrants and refugees since the late 1800s (22), and CDC has maintained a database of selected examinations abroad and domestically since 1996. Before full implementation of EDN in 2009, the notifications provided to state and local health departments of immigrant and refugee arrivals was incomplete or delayed, which did not allow for robust data analysis. The current system, EDN, has multiple functions. First, as a disease notification system, EDN provides systematic collection and electronic transmission of information on communicable diseases of public health significance for newly arriving immigrants with medical conditions and all refugees, facilitating prompt medical care after arrival when needed. Second, EDN can be used as a registry of all refugee arrivals to find specific refugees after disease outbreaks are identified and follow-up investigation is required. Finally, the medical screening data provided by EDN is analyzed and used to develop or enhance evidence-based medical guidance for specific refugee populations (21).
Provision of timely notification to U.S. health departments of refugee and immigrant arrivals is essential for medical and public health follow-up. The HHS Office of Refugee Resettlement, which provides oversight for refugee medical assistance, initial refugee medical screening, and technical assistance and consultation for physical and mental health concerns of refugees, recommends that all refugees undergo medical screening (23) based on CDC domestic screening guidelines (21) when they arrive in the United States. The domestic medical evaluation offers refugees the continuum of health and well-being required for and supportive of successful resettlement. CDC recommends that all those with tuberculosis classifications be contacted to initiate a medical evaluation within 30 days of arrival and that the evaluation be completed within 90 days (24); EDN provides medical and contact information for state and local health officials to facilitate these evaluations.
During 2009, state and local health departments received 104,954 notifications of arrivals of refugees and of immigrants with medical conditions; a low percentage (0.4%) with Class A waivers had inadmissible medical conditions. This information equipped public health officials with timely data to rapidly identify and intervene with persons with active disease, such as HIV infection, and to identify those who needed follow-up to prevent recurrence or development of tuberculosis. During 2009, delays in providing notifications of all newly arriving refugees and immigrants with medical conditions to states occurred, likely because of an unexpected 28% increase in the number of latent tuberculosis infection referrals from the previous year resulting from the implementation of new tuberculosis technical instructions (i.e., CDOT) in originating countries and a 19.4% increase in refugee arrivals (74,062) compared with the previous fiscal year (60,108) (25). These increases in classifications and delays warranted improvements such as additional procedures and staff in the EDN data entry center.
EDN also provides surveillance data that can be used to monitor communicable diseases of public health significance among newly arriving immigrants and refugees. During 2009, most (23,363) Class B notifications were for persons with suspected tuberculosis (noninfectious at the time of the overseas medical examination), such as persons with chest radiograph findings consistent with tuberculosis but with negative sputum smears and cultures for acid-fast bacilli or persons who were a contact of a person with tuberculosis disease. Of these, 75% were reported as having initiated a follow-up examination within 30 days after arriving in the United States. This tuberculosis screening that occurs after arrival (2) provides EDN with results of the tuberculin skin test, interferon-gamma release assay, a comparison of overseas and domestic chest radiographs, sputum microscopy and bacteriology, and tuberculosis treatment. Linking the results of domestic and overseas tuberculosis examinations permits monitoring and evaluation of the overseas screening program to ensure refugees and immigrants are receiving appropriate evaluations and care.
EDN also attempts to obtain a vaccination history (Vaccination Documentation Worksheet, DS-3025) and medical history (Medical History and Physical Examination, DS-3026). These data are not included in this report because they were incomplete for 2009. Beginning in 2010, data on vaccination and medical history were entered into the EDN system. In addition, vaccination for refugees and therefore the vaccination history (DS-3025) is not always completed.
Communicable diseases are a major cause of morbidity and death among refugee populations (26). Before the EDN system was fully functional, contact information for refugees who had recently arrived and potentially been exposed to communicable diseases related to outbreaks in the host country was compiled manually through correspondence with the DOS Bureau of Population and Refugee Migration and IOM. This resulted in less timely notification and the potential for the secondary spread of disease within the United States. During 2004–2007, CDC responded to 19 outbreaks of nine vaccine-preventable diseases such as varicella among refugees bound for the United States (27). Other examples include identification and treatment of intestinal parasites among the Lost Boys of Sudan (28), malaria among refugees from East Africa (29), and increased lead levels among Burmese refugees (30). The EDN system serves as a registry of all refugee arrivals. During 2009, EDN provided public health partners with contact information needed to find and evaluate refugees in the United States who were exposed to three disease outbreaks identified in their country of origin overseas before their departure for the United States.
Findings from domestic screenings have prompted several epidemiologic studies and have enhanced overseas screening recommendations (31,32). Reports of chronic abdominal pain among 462 Sudanese refugees led to a serologic assessment in 2007 that identified active schistosomiasis infections (44%) and strongyloides infections (46%) in these refugees, despite presumptive treatment (28). A study of 39 cases of malaria during May 2007–February 2008 among newly arriving refugees who had received presumptive treatment before leaving their country found that the disease prevalence was significantly higher among those who received sulfadoxine-pyrimethamine than among those who received artemether-lumefantrine (risk ratio: 6.2; 95% confidence interval = 3.1–12.4) (29). In 2008, refugee health coordinators in six states reported increased blood lead levels (i.e., >10 µg/dL) among 13% of Burmese refugee children. An additional investigation confirmed this finding, with the highest prevalence among children aged <2 years (14.5%) (30). Collaboration by CDC program and subject-matter staff and academic partners on evaluating the findings from these studies has led to improved health-care guidance for refugees bound for the United States, such as presumptive treatment for malaria and parasitic diseases.
Limitations
The findings in this report are subject to at least four limitations. First, the majority of immigrant records (approximately 400,000) are not collected; thus, the health status of most newly arriving immigrants cannot be described completely. Second, certain medical documents of immigrants with medical conditions are not collected or are missing at ports of entry, which might result in lower estimates of medical conditions. Third, the medical history is self-reported; thus, follow-up is necessary to identify and verify chronic health conditions. Finally, missing personal information, such as destination location, poses a challenge to timely notification and follow-up.
Conclusion
Since 2009, the EDN system has strived to improve the timeliness, accuracy, accessibility, and comprehensiveness of its data. In collaboration with the DOS Bureau of Population, Refugees, and Migration, the EDN system began acquiring direct data for every newly arriving refugee and notifying health departments of these arrivals within 5–7 days. Also, U.S. destination information is more accurate than it was previously. The EDN system experienced an increase in the number of users from 438 in 2009 to 719 in 2013, and the number of jurisdictions notified increased from 233 in 2009 to 283 in 2013. The EDN system allows a clinic or health-care provider read-only access to overseas medical records of persons arriving in their local community. To ensure that medical information for refugees is as complete as possible during their U.S. medical examination, the EDN system includes information on any vaccinations and predeparture medical interventions such as presumptive treatment for malaria and intestinal parasites provided by IOM.
Fulfilling CDC's mission to protect the public from emerging and reemerging diseases depends, in part, on data obtained from the overseas medical examinations of all newly arriving refugees and immigrants with medical conditions. Public health officials rely on EDN data to track new arrivals who might have been exposed to a disease such as tuberculosis, which allows for interventions to safeguard the public from imported communicable diseases. The overseas medical evaluation is a critical component in reducing the importation of communicable diseases into the United States. Documentation of findings from the medical examination combined with tuberculosis (and other diseases and conditions) follow-up data after arrival in EDN allows for the evaluation of that data, the identification of disease trends among arriving refugee populations, and the provision of evidence-based recommendations to federal, state, and local public health officials, as well as to the international public health community.
Acknowledgments
The findings in this report are based, in part, on contributions by the U.S. Customs and Border Protection and CDC quarantine station personnel, the staff members of the Electronic Disease Notification data entry center, the Division of Global Migration and Quarantine informatics team, the International Organization for Migration and Division of Tuberculosis and Elimination, overseas panel physicians, U.S. health departments staff members, Yoni Haber, Nekeia Gray, Ava Navin, Nicole Cohen, and Martin Cetron.
References
- US Department of Homeland Security. 2009 yearbook of immigration statistics. Washington, DC: US Department of Homeland Security; 2010. Available at http://www.dhs.gov/xlibrary/assets/statistics/yearbook/2009/ois_yb_2009.pdf.
- Liu Y, Weinberg MS, Ortega LS, Painter JA, Maloney SA. Overseas screening for tuberculosis in U.S.-bound immigrants and refugees. N Engl J Med 2009;360:2406–15.
- CDC. 2007 tuberculosis screening and treatment technical instructions for panel physicians. Atlanta, GA: CDC; 2007. Available at http://www.cdc.gov/immigrantrefugeehealth/exams/ti/panel/tuberculosis-panel-technical-instructions.html.
- CDC. Tuberculosis screening and treatment (TB TIs) using cultures and directly observed therapy (DOT): frequently asked questions (FAQ). Atlanta, GA: US Department of Health and Human Services, CDC. Available at http://www.cdc.gov/immigrantrefugeehealth/exams/ti/panel/tuberculosis-panel-technical-instructions-faq.html.
- CDC. Trends in tuberculosis—United States, 2011. MMWR 2012;61:181–5.
- US Department of State. Proposed refugee admission for fiscal year 2009. Washington, DC: US Department of State; 2008. Available at http://2001-2009.state.gov/g/prm/refadm/rls/rpts/52366.htm.
- US Department of State. Special immigrant visas (SIVs) for Iraqi and Afghan translators/interpreters. Washington, DC: US Department of State. Available at http://travel.state.gov/visa/immigrants/info/info_3738.html.
- International Organization for Migration. Geneva, Switzerland. Available at http://www.iom.int/jahia/jsp/index.jsp.
- World Health Organization. International health regulations. Geneva, Switzerland: World Health Organization; 2005. Available at http://www.who.int/ihr/en.
- CDC. Technical instructions for panel physicians. Atlanta, GA: US Department of Health and Human Services, CDC; 1991. Available at http://www.cdc.gov/immigrantrefugeehealth/exams/ti/panel/tuberculosis-panel-technical-instructions.html.
- CDC. Tuberculosis screening and treatment technical instructions (TB TIs) using cultures and directly observed therapy (DOT): implementation. Atlanta, GA: US Department of Health and Human Services, CDC. Available at https://www.cdc.gov/immigrantrefugeehealth/exams/ti/panel/tuberculosis-implememtation.html.
- Maloney SA, Fielding KL, Laserson KF, et al. Assessing the performance of overseas tuberculosis screening programs: a study among US-bound immigrants in Vietnam. Arch Intern Med 2006;166:234–40.
- CDC. Multidrug-resistant tuberculosis in Hmong refugees resettling from Thailand to the United States, 2004–2005. MMWR 2005;54:741–4.
- US Citizenship and Immigration Services. I-601, Application for waiver of grounds of inadmissibility. Washington, DC: US Citizenship and Immigration Services. Available at http://www.uscis.gov/portal/site/uscis.menuitem.5af9bb95919f35e66f614176543f6d1a/?vgnextoid=bb515f56ff55d010VgnVCM10000048f3d6a1RCRD&vgnextchannel=db029c7755cb9010VgnVCM10000045f3d6a1RCRD.
- CDC. Quarantine stations. Atlanta, GA: CDC. Available at http://www.cdc.gov/quarantine/quarantinestations.html.
- US Customs and Border Protection. Locate a port of entry—air, land, or sea. Washington, DC: US Customs and Border Protection. Available at http://www.cbp.gov/xp/cgov/toolbox/contacts/ports.
- International Organization for Migration. Migrant management operational systems application. Geneva, Switzerland: International Organization for Migration. Available at http://www.mimosa.iom.int/confluence/display/MAU1/MiMOSA+Official+Website.
- CDC. Public Health Information Network messaging system. Atlanta, GA: CDC. Available at http://www.cdc.gov/phin/tools/PHINms/index.html.
- CDC. Final rule removing HIV infection from U.S. immigration screening [updated April 2, 2010 and July 20, 2011]. Atlanta, GA: CDC. Available at http://www.cdc.gov/immigrantrefugeehealth/laws-regs/hiv-ban-removal/final-rule.html.
- CDC. Epi-X: the Epidemic Information Exchange. Atlanta, GA: CDC. Available at http://www.cdc.gov/epix.
- CDC. Guidelines for the U.S. domestic medical examination for newly arriving refugees. Atlanta, GA: CDC. http://www.cdc.gov/immigrantrefugeehealth/guidelines/domestic/domestic-guidelines.html.
- Yew E. Medical inspection of immigrants at Ellis Island, 1891–1924. Bull N Y Acad Med 1980;56:488–510.
- US Department of Health and Human Services, Administration for Children and Families, Office of Refugee Resettlement. Washington DC: US Department of Health and Human Services. Available at http://www.acf.hhs.gov/programs/orr.
- CDC. Monitoring tuberculosis programs—National Tuberculosis Indicator Project, United States, 2002–2008. MMWR 2010;59:295–8.
- US Department of Homeland Security. Annual flow report—refugees and asylees: 2009. Washington, DC: US Department of Homeland Security. Available at http://www.dhs.gov/xlibrary/assets/statistics/publications/ois_rfa_fr_2009.pdf.
- World Health Organization. Outbreak surveillance and response in humanitarian emergencies: WHO guidelines for EWARN implementation. Geneva, Switzerland: World Health Organization. Available at http://whqlibdoc.who.int/hq/2012/WHO_HSE_GAR_DCE_2012_1_eng.pdf.
- CDC. Cost of vaccinating refugees overseas versus after arrival in the United States, 2005. MMWR 2008;57:229–32.
- Posey DL, Blackburn BG, Weinberg M, et al. High prevalence and presumptive treatment of schistosomiasis and strongyloidiasis among African refugees. Clin Infect Dis 2007;45:1310–5.
- Phares CRKB, Doney AC, Arguin PM, et al. Presumptive treatment to reduce imported malaria among refugees from east Africa resettling in the United States. Am J Trop Med Hyg 2011;85:612–5.
- Mitchell T, Jentes E, Ortega L, et al. Lead poisoning in United States-bound refugee children: Thailand-Burma border, 2009. Pediatrics 2012;129:e392–9.
- CDC. Overseas refugee health guidelines: malaria. Atlanta, GA: CDC; 2012. Available at http://www.cdc.gov/immigrantrefugeehealth/guidelines/overseas/malaria-guidelines-overseas.html.
- CDC. Overseas refugee health guidelines: intestinal parasites. Atlanta, GA: CDC; 2012. Available at http://www.cdc.gov/immigrantrefugeehealth/guidelines/overseas/intestinal-parasites-overseas.html.
FIGURE 1. CDC Electronic Disease Notification system flow chart
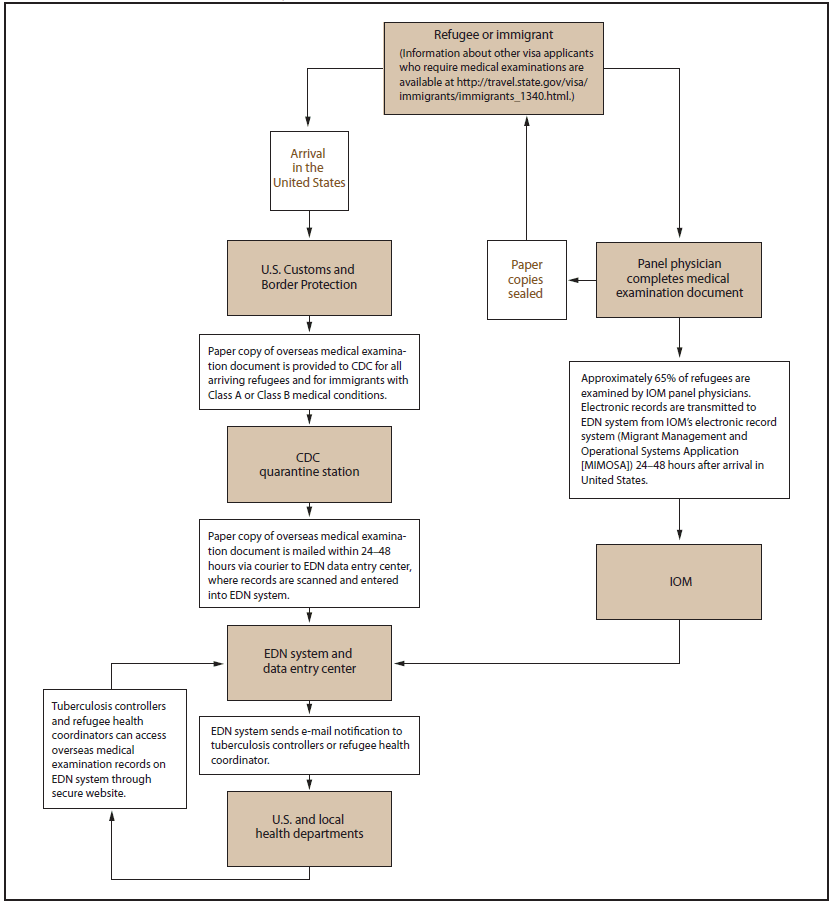
Abbreviation: EDN = Electronic Disease Notification; IOM = International Organization for Migration.
Alternate Text: The figure shows a flow chart for refugees or immigrants entering the United States. After arrival in the United States, all refugees are recommended to obtain a medical assessment by a health-care provider or a health department within 30 days. In addition, immigrants with certain medical conditions such as noninfectious tuberculosis at the time of the original medical examination are recommended to be evaluated after arrival to ensure that appropriate prevention or treatment measures are instituted.
FIGURE 2. CDC U.S. quarantine stations and Electronic Disease Notification system jurisdictions in 2009*
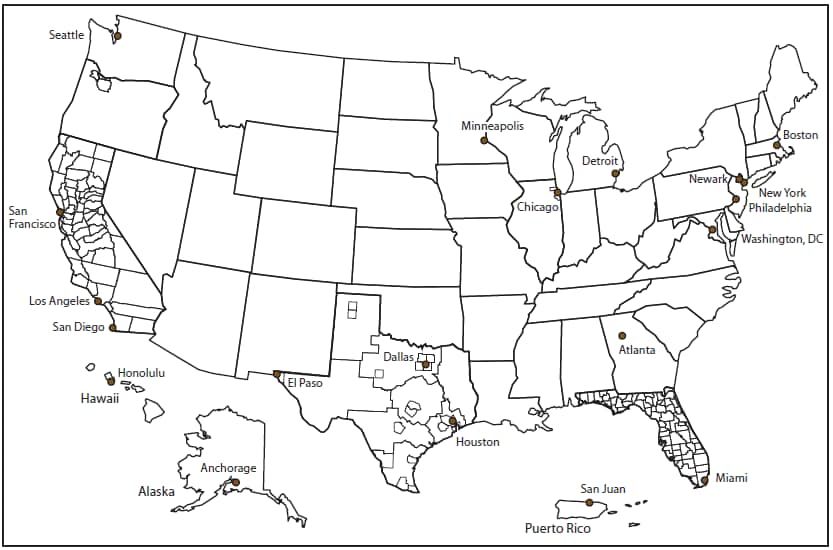
* Quarantine stations are indicated by dots; Electronic Disease Notification jurisdictions (N = 223) are indicated by borders. Jurisdictions include individual states, counties, and cities. Notifications of arrivals in Puerto Rico are coordinated by the quarantine station and local health department.
Alternate Text: The figure is a map of the United States that indicates the location of quarantine stations and Electronic Disease Notification system jurisdictions.
FIGURE 3. Number of days from arrival until notification of immigrants, refugees,* and persons with other visa types† — Electronic Disease Notification system, United States, 2009
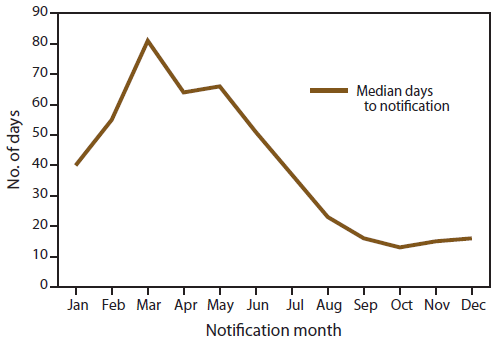
* Refugee arrivals include Iraqis and Afghans with special immigrant visas.
† Asylees, parolees, and unknown.
Alternate Text: The figure shows the median number of days from arrival until notification of immigrants, refugees (including Iraqis and Afghans with special immigrant visas), and persons with other visa types (i.e., asylees, parolees, and unknown) whose records are contained in CDC's Electronic Disease Notification system for 2009, by month.
FIGURE 4. Number of notifications for suspected tuberculosis classifications,* by county — Electronic Disease Notification system, United States, 2009
Abbreviation: CDOT = culture and directly observed therapy.
* Class B tuberculosis was defined as chest radiograph findings consistent with tuberculosis without a positive sputum smear or culture (B1), latent tuberculosis infection (B2), or contact with a person with a case of tuberculosis. Class B1, 1991: chest radiograph findings consistent with active tuberculosis without a positive sputum smear; CDOT: chest radiograph findings consistent with tuberculosis without a positive sputum smear or culture. Class B2, 1991: chest radiograph findings consistent with inactive tuberculosis without a positive smear; 2007: latent tuberculosis infection.
Alternate Text: The figure is a map of the United States by county showing the number of notifications for suspected tuberculosis classifications from CDC's Electronic Disease Notification system for 2009. Class B tuberculosis was defined as chest radiograph findings consistent with tuberculosis without a positive sputum smear or culture (B1), latent tuberculosis infection (B2), or contact with a person with a case of tuberculosis. Class B1, 1991: chest radiograph findings consistent with active tuberculosis without a positive sputum smear; CDOT: chest radiograph findings consistent with tuberculosis without a positive sputum smear or culture. Class B2, 1991: chest radiograph findings consistent with inactive tuberculosis without a positive smear; 2007: latent tuberculosis infection.
|
TABLE 7. (Continued) Number and percentage of immigrants, refugees,* and persons with other visa types† with tuberculosis classifications arriving in the United States, by percentage of follow-up and by Class B classification — Electronic Disease Notification system, United States, 2009 |
|||||||||
|---|---|---|---|---|---|---|---|---|---|
|
Destination state/area |
Ranking, |
Total |
Classification used to assign |
Reported |
|||||
|
1991 tuberculosis technical instructions§ |
CDOT§ |
||||||||
|
B1 |
B2 |
B1 |
B2 |
B3 |
|||||
|
No. |
(%) |
(%) |
(%) |
(%) |
(%) |
(%) |
|||
|
Utah |
27 |
159 |
(0.7) |
(3.1) |
(6.9) |
(46.5) |
(42.1) |
(1.3) |
(95.6) |
|
Vermont |
45 |
32 |
(0.1) |
— |
(3.1) |
(68.8) |
(25.0) |
(3.1) |
(93.8) |
|
Virginia |
10 |
485 |
(2.1) |
(3.5) |
(9.3) |
(51.5) |
(33.8) |
(1.2) |
(25.9) |
|
Washington |
5 |
918 |
(3.9) |
(4.4) |
(10.8) |
(48.3) |
(33.6) |
(2.9) |
(93.1) |
|
West Virginia |
50 |
12 |
(0.1) |
(8.3) |
(8.3) |
(33.3) |
(50.0) |
— |
(58.3) |
|
Wisconsin |
28 |
157 |
(0.7) |
(4.5) |
(9.6) |
(47.1) |
(33.8) |
(5.1) |
(78.5) |
|
Wyoming |
51 |
10 |
(0) |
— |
— |
(70.0) |
(30.0) |
— |
(100.0) |
|
Other** |
— |
404 |
(1.7) |
(1.7) |
(0.7) |
(41.1) |
(55.0) |
(1.5) |
— |
|
Total |
— |
23,341 |
(100.0) |
(3.2) |
(7.5) |
(49.9) |
(38.2) |
(1.1) |
(75.4)†† |
|
Abbreviation: CDOT = culture and directly observed therapy. * Refugee arrivals include Iraqis and Afghans with special immigrant visas. † Asylees, parolees, and unknown. § Class B1, 1991: chest radiograph findings consistent with active tuberculosis without a positive sputum smear; CDOT: chest radiograph findings consistent with tuberculosis without a positive sputum smear or culture. Class B2, 1991: chest radiograph findings consistent with inactive tuberculosis without a positive smear; 2007: latent tuberculosis infection. Class B tuberculosis was defined as chest radiograph findings consistent with tuberculosis without a positive sputum smear or culture (B1), latent tuberculosis infection (B2), or contact with a person with a case of tuberculosis (B3). ¶ Indicates that a worksheet was initiated by the health department. Tuberculosis follow-up data from some states might not have been reported in the system. ** Includes Guam, Puerto Rico, U.S. Marshall Islands, U.S. Virgin Islands, and unknown. †† Median percentage represents instances of tuberculosis follow-up that were reported in the system. |
|||||||||
Use of trade names and commercial sources is for identification only and does not imply endorsement by the U.S. Department of Health and Human Services.
References to non-CDC sites on the Internet are
provided as a service to MMWR readers and do not constitute or imply
endorsement of these organizations or their programs by CDC or the U.S.
Department of Health and Human Services. CDC is not responsible for the content
of pages found at these sites. URL addresses listed in MMWR were current as of
the date of publication.
All MMWR HTML versions of articles are electronic conversions from typeset documents.
This conversion might result in character translation or format errors in the HTML version.
Users are referred to the electronic PDF version (http://www.cdc.gov/mmwr)
and/or the original MMWR paper copy for printable versions of official text, figures, and tables.
An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S.
Government Printing Office (GPO), Washington, DC 20402-9371;
telephone: (202) 512-1800. Contact GPO for current prices.
**Questions or messages regarding errors in formatting should be addressed to
[email protected].
