 |
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail. Lyme Disease --- United States, 1999Lyme disease (LD) is caused by the tickborne spirochete Borrelia burgdorferi sensu lato and is the most common vectorborne disease in the United States. Surveillance for LD was initiated by CDC in 1982, and the Council of State and Territorial Epidemiologists designated it a nationally notifiable disease in January 1991. This report summarizes the number of LD cases reported to CDC during 1999. Although the number of cases decreased from 1998, the number of cases in 1999 was higher than the number reported during the early 1990s. LD can be prevented by avoiding tick-infested habitats, by using personal protective measures, by vaccination, by checking for and removing ticks attached to the body and clothes, and by reducing tick populations. For surveillance purposes, LD is defined as the presence of an erythema migrans rash >5 cm (>2 inches) in diameter or at least one late manifestation of musculoskeletal, neurologic, or cardiovascular disease with laboratory confirmation of B. burgdorferi infection (1). Incidence rates for states and the District of Columbia (DC) were calculated using U.S. Census Bureau 1999 population estimates; county rates were based on 1995 population estimates. During 1990--1996, the number of reported LD cases was 7943, 9470, 9908, 8257, 13,043, 11,700, and 16,455, respectively. In 1999, 16,273 LD cases were reported (overall incidence: 6.0 per 100,000 population), a 3% decrease from 16,801 cases reported in 1998 and a 21% increase from 12,801 cases reported in 1997 (Figure 1). Most cases were reported in northeastern, mid-Atlantic, and north central states (Table 1). Nine states reported LD incidences higher than the national rate (i.e., Connecticut, 98.0; Rhode Island, 55.1; New York, 24.2; Pennsylvania, 23.2; Delaware, 22.2; New Jersey, 21.1; Maryland, 17.4; Massachusetts, 12.7; and Wisconsin, 9.3). These states accounted for 92.0% of the nationally reported cases. Alaska, Georgia, Hawaii, Montana, and South Dakota reported no cases during 1999. From 1998 to 1999, 22 states had increases in the number of cases, 24 states and DC had decreases, and four states had no change. County of residence was available for 16,214 (99.6%) LD patients. Among the 3143 U.S. counties, 713 (22.7%) had at least one case during 1999; 90% of the cases were from 109 (15.3%) reporting counties (Figure 2). Incidence exceeded 100 cases per 100,000 population in 24 counties in Connecticut, Maryland, Massachusetts, Minnesota, New Jersey, New York, Pennsylvania, Rhode Island, and Wisconsin; the highest county-specific incidence (950.7) occurred in Nantucket County, Massachusetts. Among the 16,145 (99.2%) patients for whom age was reported, 4061 (25.0%) were aged <15 years; 2005 (12.3%) were 15--29 years, 3528 (21.7%) were 30--44 years, 3694 (22.7%) were 45--59 years, 2051 (12.6%) were 60--74 years, and 806 (5.0%) were >75 years. Among the 16,226 patients for whom sex was reported, 8511 (52.5%) were male. Of patients <15 years, 2338 (57.8%) were male; of patients 15--29 years, 1139 (56.9%) were male; of patients >75 years, 360 (44.6%) were male. Among 12,479 (76.7%) patients for whom month of illness onset was reported, 7161 (57.4%) had illness onset during June (28.5%) and July (28.9%); <5.8% reported illness onset during January, February, and December 1999. Reported by: State health depts. Bacterial Zoonoses Br, Div of Vector-borne Infectious Diseases, National Center for Infectious Diseases, CDC. Editorial Note:From 1991 to 1999, the incidence of LD increased 1.7-fold. The geographic distribution expanded early in the epidemic, then stabilized (2). Most cases continue to occur in northeastern, mid-Atlantic, and north central states. The large proportion of patients aged <15 years and 45--59 years may be the result of greater exposure than other groups to infected ticks, to less use of personal protective measures, to differential use of health-care services, or to reporting bias. The large number of reported LD cases during June and July reflects the seasonal peak of host-seeking activities of infective nymphal-stage vector ticks in areas where LD is endemic (3). The findings in this report are subject to at least three limitations. First, distribution of reported cases could be distorted by reporting bias. Second, LD is underreported in areas where it is endemic and may be overreported where it is not endemic. Third, the LD case definition is limited in sensitivity and specificity, not all LD cases present with typical manifestations and other conditions may be confused with LD, and laboratory testing may be inaccurate. LD can be prevented by avoiding tick-infested areas, using repellents, and promptly removing ticks that become attached to clothing or the body. A vaccine for persons aged 15--70 years, approved by the Food and Drug Administration in 1998, is 76% effective in preventing LD after three doses (4). New methods of reducing tick vectors are being developed (e.g., baited devices that passively apply acaricides to deer and rodents) (5; CDC, unpublished data, 2001). In addition, early diagnosis and treatment of LD can reduce morbidity. Updated guidelines for LD treatment were published in 2000 (6,7). CDC supports collaborative efforts with health departments and academic and nonprofit organizations to prevent LD. During 2001, community-based projects are being initiated with the goal of reducing incidence to 9.7 per 100,000 population by 2010 in states where LD is endemic (8). Additional information about LD is available at http://www.cdc.gov/ncidod/dvbid/lymeinfo.htm. References
Table 1  Return to top. Figure 1 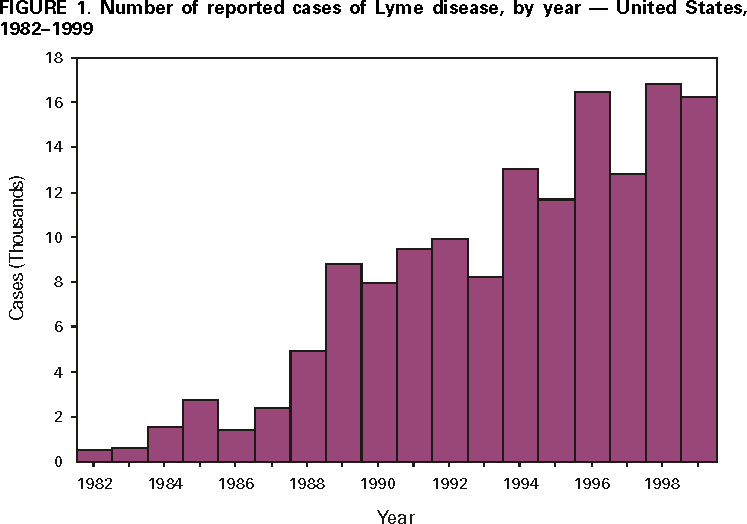 Return to top. Figure 2  Return to top. Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to [email protected].Page converted: 3/15/2001 |
|||||||||
This page last reviewed 5/2/01
|