|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
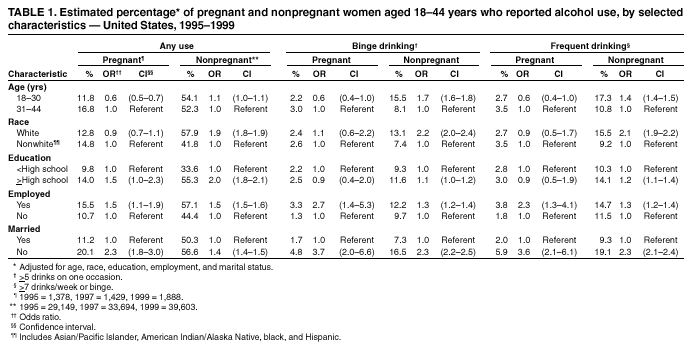
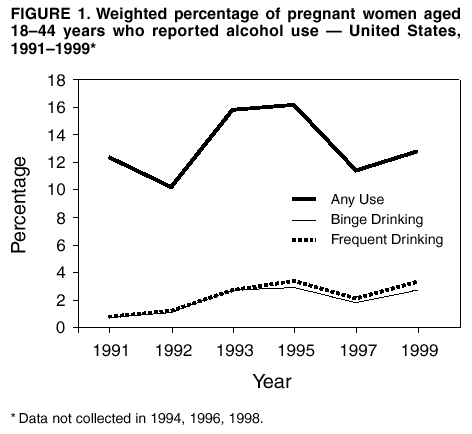
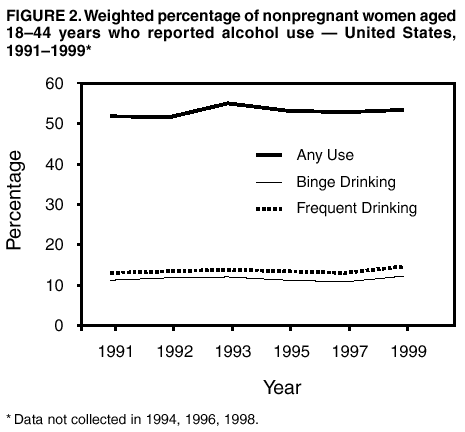
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail. Alcohol Use Among Women of Childbearing Age --- United States, 1991--1999Please note: An erratum has been published for this article. To view the erratum, please click here. Prenatal exposure to alcohol is one of the leading preventable causes of birth defects, mental retardation, and neurodevelopmental disorders in the United States (1). One of the national health objectives for 2010 is to decrease alcohol use among pregnant women to 94% (2). During 1991--1995, alcohol use by pregnant women increased substantially, and alcohol use by nonpregnant women of childbearing age increased slightly (3). To characterize trends in alcohol use among women of childbearing age, CDC analyzed representative survey data from the Behavioral Risk Factor Surveillance System (BRFSS) during 1991--1999. This report summarizes the results of the analysis, which indicate that the rate of any alcohol use (i.e., at least one drink) during pregnancy has declined since 1995. However, rates of binge drinking (i.e., >5 drinks on any one occasion) and frequent drinking (i.e., >7 drinks per week or >5 drinks on any one occasion) during pregnancy have not declined among nonpregnant women of childbearing age. Health-care providers should routinely screen women of childbearing age for alcohol use and counsel them about the adverse effects of alcohol use during pregnancy. BRFSS is an ongoing, state-based, random-digit--dialed telephone survey of the noninstitutionalized U.S. civilian population aged >18 years. Data were analyzed for women aged 18--44 years in all 50 states. Women were asked about their use of alcohol during the 30 days preceding the survey. Three alcohol drinking patterns were examined: any use, binge drinking, and frequent drinking. Information on alcohol use was obtained every year through 1993 and every other year thereafter. Sample data were weighted to reflect general population estimates, and standard errors were calculated by using SUDAAN. Linear regression models were used to examine temporal trends. To determine statistical significance, the inverse of the variance estimates was used for weights. Multivariate logistic analysis was conducted to examine the age, race, education level, employment, and marital status of pregnant and nonpregnant women by patterns of alcohol use. Because of the limited number of pregnant women surveyed, data were combined for 1995--1999 for the analysis of the characteristics of pregnant women who engaged in these risk behaviors. During 1995--1999, a total of 4,695 (4.3%) of the 107,141 women aged 18--44 years who were interviewed about their alcohol use during the month preceding the survey reported that they were pregnant at the time of the interview. The prevalence of any alcohol use among pregnant women increased from 12.4% in 1991 to 16.3 % in 1995 (Figure 1) (3). Compared with 1995 data, prevalence was lower in 1997 (11.4%) and 1999 (12.8%). In contrast, the rates of binge drinking and frequent drinking reported by pregnant women in 1995 remained substantially unchanged in 1997 and 1999: binge drinking rates were 2.9% in 1995, 1.8% in 1997, and 2.7% in 1999, and frequent alcohol use rates were 3.5% in 1995, 2.1% in 1997, and 3.3% in 1999. Among nonpregnant women who reported any alcohol use (Figure 2), rates remained stable: 53.2% in 1995, 52.8% in 1997, and 53.3% in 1999. Binge drinking rates among this population were 11.2% in 1995, 10.8% in 1997, and 12.3% in 1999. In comparison with other pregnant women, pregnant women who reported any alcohol use, binge drinking, and frequent drinking were more likely to be aged >30 years, employed, and unmarried (Table 1). Nonpregnant women who reported any alcohol use, binge drinking, and frequent drinking had similar employment and marital status as pregnant women. In addition, nonpregnant women reporting any alcohol use were more likely to be white and to have higher education levels than women who did not engage in this behavior; nonpregnant women who reported binge drinking and frequent drinking tended to be aged <30 years. Reported by: JS Sidhu, MD, RL Floyd, DSN, Div of Birth Defects and Developmental Disabilities, National Center on Birth Defects and Developmental Disabilities, CDC. Editorial Note:The findings in this report indicate that overall rates of any alcohol use during pregnancy declined since 1995. However, rates of binge drinking and frequent drinking during pregnancy did not decline and remain higher than the 2010 Healthy People objectives. These findings are consistent with those from the National Household Survey on Drug Abuse (4). Among nonpregnant women in their peak childbearing years, the use of alcohol, including the riskier practices of frequent and binge drinking, has not declined (5,6). Prenatal drinking patterns are highly predictive of alcohol use during pregnancy (4). Pregnant women who are unmarried and older tend to have the highest rates of alcohol use (4). Women who drink alcohol are more likely than other women to be white, unmarried, younger, and working full time outside the home (7). Age is one characteristic that distinguishes heavier drinking patterns among pregnant and nonpregnant women. In this analysis, binge drinking and frequent drinking during pregnancy were more common in women aged 30--44 years, but among nonpregnant women, these drinking patterns were more likely to occur among women <30 years. Women aged <30 years tend to reduce alcohol use when they become aware they are pregnant, but women aged >30 years are less likely to reduce alcohol use after learning they are pregnant (5), indicating greater alcohol dependency and difficulty in reducing or eliminating alcohol use during pregnancy (8). The findings in this report are subject to at least three limitations. First, BRFSS data are self-reported and might be subject to reporting biases, especially among pregnant women who are aware that alcohol use is not advised. Second, because BRFSS is a telephone survey of the noninstitutionalized U.S. population, homeless women, women in homes without telephones, and women who are institutionalized were not surveyed. Both of these limitations could have an impact on prevalence rates. Finally, because the proportion of pregnant women in this sample who were drinkers was limited, these estimated prevalence rates are subject to variability. Heavy alcohol use before pregnancy is highly predictive of continued use, chiefly among older prenatal patients. Because levels of binge and frequent drinking among nonpregnant women have not declined, all women of childbearing age should be warned about the adverse effects of alcohol use, especially high-risk drinking patterns (i.e., binge drinking and frequent drinking), and health-care providers should learn effective techniques for screening for, and intervening with, binge and frequent drinkers. Routine screening can enhance women's present and future health and might avert early prenatal exposure before women become aware of pregnancy. Using brief intervention techniques and encouraging patients to seek social support through friends, family, and community groups might encourage women to abstain from alcohol use during pregnancy (9). Potential disparities in health knowledge of pregnant women might be a contributing factor to sustained levels of binge and frequent drinking. To ensure more uniform dissemination of prenatal alcohol prevention messages, CDC, in collaboration with the Association of Schools of Public Health, will conduct targeted media campaigns to increase public awareness of the adverse effects of alcohol use during pregnancy among diverse geographic and racial/ethnic populations and among younger women. Additional information about CDC's activities to prevent alcohol-exposed pregnancies is available at www.cdc.gov/ncbddd/fas. References
|
Use of trade names and commercial sources is for identification only and does not imply endorsement by the U.S. Department of
Health and Human Services. |
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices.
**Questions or messages regarding errors in formatting should be addressed to [email protected].Page converted: 4/4/2002
|
|
|||||
|
HOME |
ABOUT MMWR |
MMWR SEARCH |
DOWNLOADS |
RSS
|
CONTACT
|
|||||
|
|
|||||
|
This page last reviewed 4/4/2002