|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
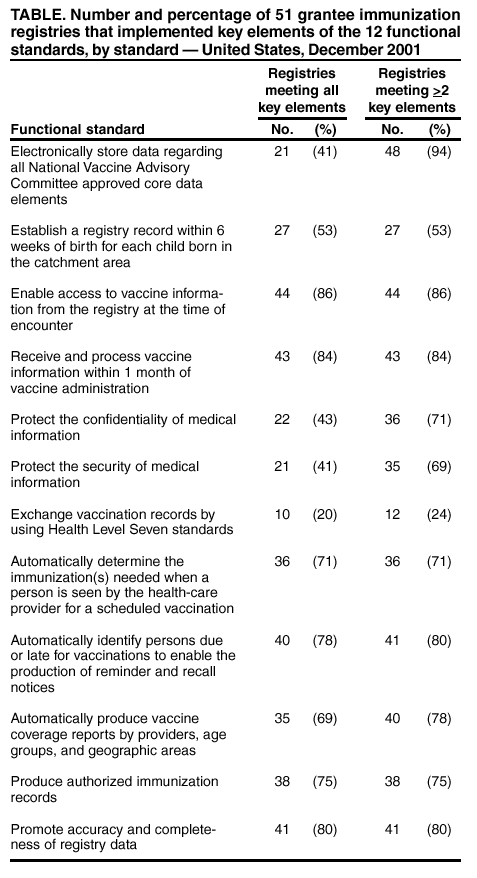
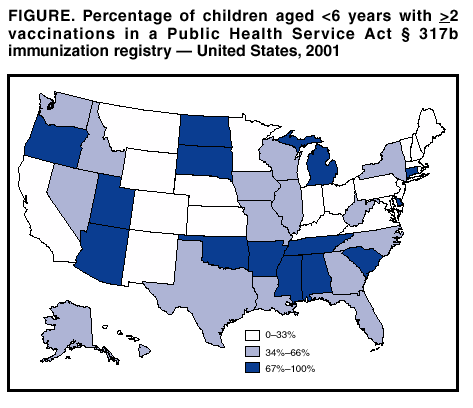
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail. Immunization Registry Progress --- United States, 2002Immunization registries are confidential, population-based, computerized information systems that collect vaccination data about all children within a geographic area (1). By providing complete and accurate information on which to base vaccination decisions, registries are key tools to increase and sustain high vaccination coverage. Registries consolidate vaccination records of children from multiple health-care providers, identify children who are due or late for vaccinations, generate reminder and recall notices to ensure that children are vaccinated appropriately, and identify provider sites and geographic areas with low vaccination coverage. One of the national health objectives for 2010 is to increase to 95% the proportion of children aged <6 years who participate in fully operational, population-based immunization registries (objective 14.26) (2). This report summarizes data from the calendar year 2001 Immunization Registry Annual Report (CY 2001 IRAR), a survey of registry activity among immunization programs in the 50 states and the District of Columbia (DC) that receive grant funding under Public Health Service Act § 317b. Although these data indicate that approximately half of U.S. children aged <6 years are participating in a registry, achieving the national health objective will require increased immunization provider participation. The CY 2001 IRAR, a self-administered questionnaire, was distributed to immunization program managers as part of the annual reporting requirement for grantees. Information included the percentage of children participating in a registry that reside in the catchment area and the progress in implementing the 12 functional standards considered essential for immunization registry operation (3). Responses were received from all 50 states and DC. Of the 51 respondents, 44 (86%) reported operating registries that targeted their entire catchment areas. The remaining seven (14%) respondents (California, Colorado, Georgia, Indiana, Minnesota, New Mexico, and New York) reported operating registries that targeted regions or counties within their catchment areas (Figure). On the basis of 2001 U.S. census estimates, approximately 44% of U.S. children aged <6 years had two or more vaccinations recorded in a grantee registry. All 51 respondents reported efforts to meet the key elements of the 12 functional standards established for immunization registries (Table). A total of seven (14%) registries accept immunization information for children aged <6 years only, 30 (59%) for all ages in their registries, and 14 (27%) for persons in their registry aged 17--25 years. A total of 14 (27%) reported using their registries to identify children eligible for the Vaccines for Children Program (VFC). Reported by: S Jones, MPH, T Boyd, MS, R Linkins, PhD, Data Management Div, National Immunization Program, CDC. Editorial Note:The findings in this report indicate the continuation of a trend identified previously in IRAR surveys (4,5). An increasing percentage of children are participating in registries each year, and registries are increasing their usefulness to public health programs nationwide. Beginning in 2001, diphtheria, tetanus toxoid, and pertussis (DTaP) vaccine; pneumococcal conjugate (PCV7) vaccine; measles, mumps, and rubella (MMR) vaccine; and varicella vaccines were in short supply (6--8). During the shortage, registries were used to track children who missed vaccines because of the shortage and to recall them when vaccines became available. During the 2001--2002 school year, immunization program staff and school nurses used the DC registry to ensure that local schools were in compliance with school entry vaccination requirements. Daily, weekly, and monthly reports were generated to track compliance, monitor vaccine inventory needs, and identify pockets of low vaccination within DC for further outreach efforts. The registry was used to identify approximately 20,000 children who were not vaccinated properly according to school vaccination requirements (CDC, unpublished data, 2002). Although this report indicates a substantial increase in participation rates compared with previous years (4,5), at least part of this improvement can be attributed to differences in how participation was measured. Previous estimates counted only participants from population-based registries. Because CY 2001 IRAR data indicated that some encounter-based registries are approaching or have reached the 95% participation goal, participants from all 51 grantee registries, both population-based and encounter-based, were included in participation rate estimates. The findings in this report are subject to at least three limitations. First, because the CY 2001 IRAR relied on self-reported information, bias in reporting might have occurred. However, onsite verification through record reviews and observation of registry operations during 12 site visits conducted in 2001 indicated that 97% of the CY 2001 IRAR's self-reported answers from these sites were accurate (CDC, unpublished data, 2002). Second, this report includes only information from 51 immunization survey respondents; any registry development performed by other entities (e.g., U.S. commonwealth or territory immunization grantees, hospitals, local health departments, or managed care plans) was not reflected. Finally, the CY 2001 IRAR did not collect information about the completeness or accuracy of immunization data recorded in a registry. CDC is developing tools to assist with registry data quality assessment. As immunization grantees continue to make progress in achieving the national health objectives for 2010, registry target age groups are expanding to include adolescents and adults. Registries also are becoming part of broader child health information systems (e.g., hearing, lead, newborn metabolic, and nutrition screening). In addition, they are being used to improve the efficacy and accountability of vaccine administration in VFC. Additional information about immunization registries is available from CDC at http://www.cdc.gov/nip/registry; telephone, 800-799-7062; or e-mail, [email protected]. References
|
Use of trade names and commercial sources is for identification only and does not imply endorsement by the U.S. Department of
Health and Human Services. |
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices.
**Questions or messages regarding errors in formatting should be addressed to [email protected].Page converted: 8/29/2002
|
|
|||||
|
HOME |
ABOUT MMWR |
MMWR SEARCH |
DOWNLOADS |
RSS
|
CONTACT
|
|||||
|
|
|||||
|
This page last reviewed 8/29/2002