|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
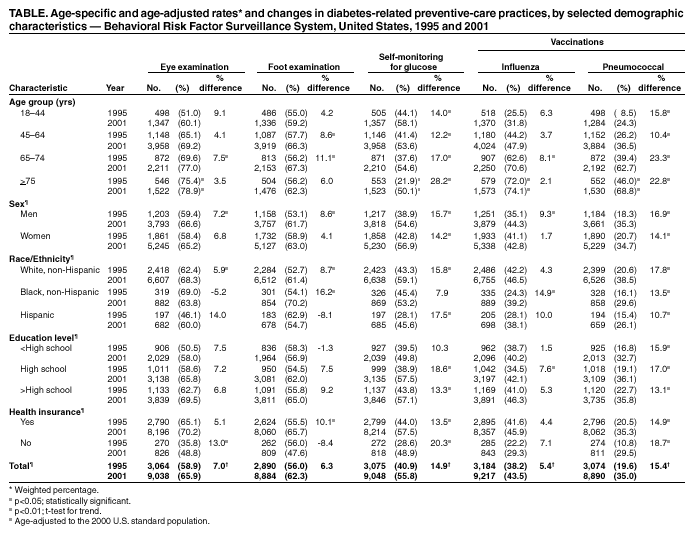
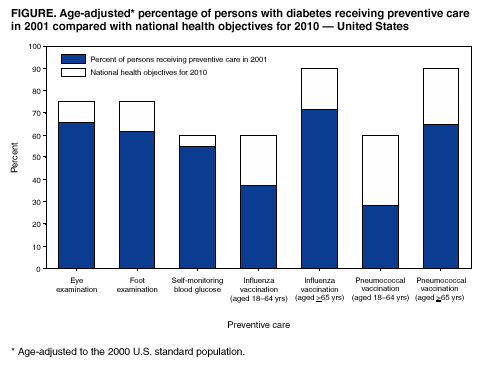
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail. Preventive-Care Practices Among Persons with Diabetes ---United States, 1995 and 2001Effective interventions are available to persons with diabetes that can prevent or delay the development of serious health complications such as lower limb amputation, blindness, kidney failure, and cardiovascular disease (1--4). However, the use of preventive-care practices is lower than recommended (5,6), and the national health objectives for 2010 aim to improve care for all persons with diabetes (7). To assess progress toward meeting these goals, CDC analyzed data on selected diabetes-related preventive-care practices, including influenza and pneumococcal vaccination coverage, from the Behavioral Risk Factor Surveillance System (BRFSS) from 1995 and 2001. This report presents the findings of these analyses, which indicate that levels of preventive-care practices among persons with diabetes in the United States increased from 1995 to 2001. Further efforts are needed to improve care among persons with diabetes, reduce the burden of diabetes-related complications, and achieve the national health objectives, including continued surveillance of diabetes-related preventive-care practices and collaboration with community-based organizations, health-care providers, public health officials, and persons with diabetes. BRFSS is a state-based, random-digit--dialed telephone survey of the noninstitutionalized U.S. population aged >18 years. The surveys are conducted in all 50 states, the District of Columbia, and three U.S. territories. Persons with diabetes were defined as respondents who answered "yes" to the question, "Has a doctor ever told you that you have diabetes?" Women who were told that they had diabetes only during pregnancy were not included. Persons who reported that they had diabetes were asked questions from the diabetes module on preventive-care practices, including: "When was the last time you had an eye exam in which the pupils were dilated?" (eye examination); "About how many times in the last year has a health professional checked your feet for any sores or irritations?" (foot examination); and "About how often do you check your blood for glucose or sugar?" (self-monitoring of blood glucose at least once daily [SMBG]). All BRFSS respondents were asked two additional questions: "During the past 12 months, have you had a flu shot?" (influenza vaccination) and "Have you ever had a pneumonia shot?" (pneumococcal vaccination). A total of 35 states had information from the diabetes module for both 1995 and 2001 and were included in these analyses. The median response rate was 68.7% for 1995 (range: 48.6%--84.5%) and 52.1% for 2001 (range: 33.3%--70.8%). Data were weighted to reflect the age, sex, and racial/ethnic distribution in each of the 35 states. The percentage of persons with diabetes who received each of the preventive-care services and vaccinations was assessed by year, selected sociodemographic characteristics, and health insurance status. Age-specific rates are presented, and rates for selected characteristics are age-adjusted to the 2000 U.S. standard population. All analyses were conducted by using SAS v8 software with SUDAAN to estimate standard errors and test for significant differences in rates between 1995 and 2001. The age-adjusted rates of all preventive-care practices increased from 1995 to 2001. The increases for rates of eye examinations and SMBG were statistically significant (Table). Rates of eye examinations increased with age for both 1995 and 2001, and in each age group rates increased from 1995 to 2001. Among persons aged 65--74 years, the increase was statistically significant. In addition, men, non-Hispanic whites, and persons without health insurance had statistically significant increases in the age-adjusted rate of eye examinations. Rates of annual foot examinations increased significantly from 1995 to 2001 among those aged 45--64 and 65--74 years. Statistically significant increases also were shown among men, non-Hispanic whites, non-Hispanic blacks, and persons with health insurance. The overall rate of SMBG was lower in the older age groups in both 1995 and 2001. However, the rate of SMBG increased significantly in all age groups. In addition, the age-adjusted rate of SMBG increased significantly among both sexes, non-Hispanic whites, Hispanics, persons with an education level of high school or greater, and persons with and without health insurance. From 1995 to 2001, the age-adjusted rate increased significantly for both influenza and pneumococcal vaccinations. However, in 2001, the age-adjusted rate of influenza vaccination among persons with diabetes was higher than that for pneumococcal vaccination (43.5% versus 35.0%). The rates of influenza vaccination increased with age for both 1995 and 2001, and rates in each age group increased from 1995 to 2001; however, the increase was statistically significant only among those aged 65--74 years. In addition, the age-adjusted rate of influenza vaccination increased significantly among men, non-Hispanic blacks, and those with a high school education. The age-specific rate of pneumococcal vaccination increased with age in both 1995 and 2001. The rate of pneumococcal vaccination increased significantly in each age group. In addition, the age-adjusted rate increased significantly among men and women, non-Hispanic whites and non-Hispanic blacks, Hispanics, persons at each level of education, and those with and without health insurance. In 2001, the age-adjusted rates of the three preventive-care practices and the two vaccinations were below levels recommended by the national health objectives (Figure). Rates of pneumococcal vaccination among younger persons with diabetes showed the largest difference compared with the 2010 objectives. Reported by: J Lojo, MPH, NR Burrows, MPH, LS Geiss, MA, EF Tierney, MPH, J Wang, MPH, MM Engelgau, MD, Div of Diabetes Translation, National Center for Chronic Disease Prevention and Health Promotion, CDC. Editorial Note:Effective interventions are available that can prevent or delay the development of diabetes complications. The findings in this report indicate that the percentage of persons with diabetes who received preventive-care services increased from 1995 to 2001. Consistent with previous reports (5,6), the rate of the use of preventive-care practices and vaccination coverage among persons with diabetes in 2001 was less than recommended, and improvement is needed in all areas of diabetes care to achieve the national health objectives. Differences observed in the reported use of diabetes-related preventive-care practices among racial/ethnic populations might reflect differences in socioeconomic status, access to care, cultural or language barriers, or other factors. In addition, these analyses identified target groups who are in need of interventions to improve their preventive care, such as younger persons with diabetes who need to receive eye examinations and vaccinations, and older persons who need to practice SMBG. The findings in this report are subject to at least five limitations. First, these analyses included only the noninstitutionalized population and cannot be generalized to persons residing in nursing homes and other institutions. Second, self-reported data are subject to recall bias, and preventive-care practices or vaccination levels might be underreported or overreported. The extent to which reporting bias might affect these results is unknown. Third, BRFSS is a telephone survey, and rates of diabetes-related preventive-care practices presented in this report might be overestimated slightly because persons of low socioeconomic status are less likely to have telephones and less likely to receive preventive care. Fourth, the median response rate was 68.7% for 1995 and 52.1% for 2001; however, compared with census data, BRFSS data have minimal bias (BRFSS data quality report; available at http://www.cdc.gov/brfss). Finally, the analysis included only 35 states and might not be representative of the entire country. However, the rates of both influenza and pneumococcal vaccinations were assessed for all states in 2001 and showed little difference from the results in this report (CDC, unpublished data, 2001). Public and private efforts to improve the level of diabetes care are ongoing (8--10). CDC collaborates with many partners to ensure good care and education for persons with diabetes. CDC and the National Institutes of Health cosponsor the National Diabetes Education Program (available at http://www.ndep.nih.gov), which develops educational tools and community-based interventions and establishes public and private partnerships to address the gap between current and desired levels of diabetes care and practices. CDC also is working with the Bureau of Primary Health Care of the Health Resources and Service Administration on the National Diabetes Collaborative, a partnership of public and private agencies to increase access to and improve the quality of diabetes care within federally funded health centers. As part of its national strategy, CDC provides resources and technical assistance to state diabetes-control programs to improve access to quality diabetes care. CDC also is working with managed-care partners on Project TRIAD (Translating Research into Action for Diabetes), a 5-year prospective study of the quality of diabetes care, costs, and outcomes in managed-care settings. Continued surveillance of diabetes-related preventive-care practices using the BRFSS will be an important tool in monitoring the effectiveness of strategies designed to improve the quality of care among persons with diabetes, identify racial/ethnic health disparities, and focus interventions to eliminate such disparities. References
|
Use of trade names and commercial sources is for identification only and does not imply endorsement by the U.S. Department of
Health and Human Services. |
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices.
**Questions or messages regarding errors in formatting should be addressed to [email protected].Page converted: 10/31/2002
|
|
|||||
|
HOME |
ABOUT MMWR |
MMWR SEARCH |
DOWNLOADS |
RSS
|
CONTACT
|
|||||
|
|
|||||
|
This page last reviewed 10/31/2002