|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
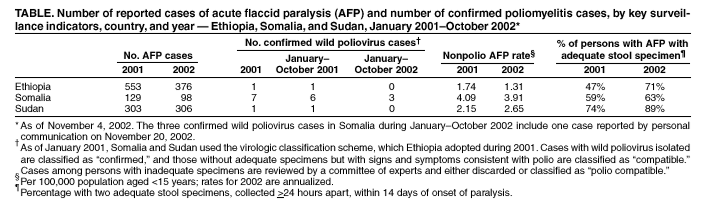
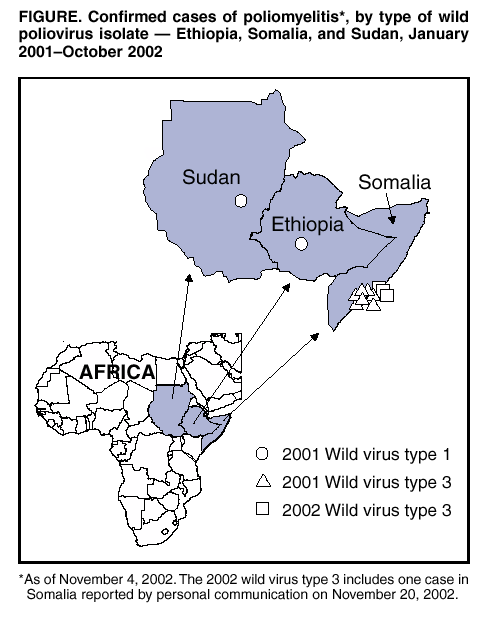
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail. Progress Toward Poliomyelitis Eradication --- Ethiopia, Somalia, and Sudan, January 2001--October 2002Since the World Health Assembly resolved in May 1988 to eradicate poliomyelitis, the estimated number of polio cases globally has declined >99%. The number of countries in which polio was estimated to be endemic decreased from 125 in 1988 to 10 in 2001, and three World Health Organization (WHO) regions (American, European, and Western Pacific) comprising approximately 55% of the world's population have been certified polio-free (1). Ethiopia, Somalia, and Sudan have achieved the lowest levels of poliovirus circulation since the polio eradication initiative began and are approaching interruption of transmission. This report describes intensified polio eradication activities in these countries during January 2001--October 2002, summarizes progress made, and highlights remaining challenges. Continued political commitment and financial support will be required to eradicate polio in these countries. Routine ImmunizationAccording to national estimates, 50% of children in Ethiopia aged <1 year received 3 doses of oral poliovirus vaccine (OPV3) in 2001. In Somalia, where vaccination services are delivered through national and international nongovernment organizations supported by WHO, the United Nations Children's Fund (UNICEF), and other United Nations agencies, OPV3 coverage was an estimated 33% in 2001. In Sudan, officially reported OPV3 coverage increased from 65% in 2000 to 71% in 2001. However, because of the lack of a routine vaccination program in the conflict-affected areas of the southern part of the country, WHO and UNICEF estimate actual total national coverage at 47%. Supplementary Immunization ActivitiesSupplementary immunization activities (SIAs) began in 1994 in Sudan, in 1996 in Ethiopia, and in 1997 in Somalia (2--4). SIAs were intensified through house-to-house vaccination beginning in 1999 in Somalia and Sudan and in 2000 in Ethiopia. During 2001--2002, at least two rounds of National Immunization Days (NIDs)* were conducted in Ethiopia, Somalia, and Sudan among children aged <5 years (total estimated target populations: 13.7 million, 1.3 million, and 7.0 million, respectively). In addition to NIDs, countries conducted additional rounds of subnational immunization days† (SNIDs) targeting high-risk areas and populations. In Ethiopia, SNIDs were conducted in 21 zones and three subzonal areas in five regions of the country. The criteria used to select these areas included previous isolation of wild poliovirus, poor surveillance indicators, poor routine vaccination coverage, below-optimal performance in previous campaigns, difficulty in obtaining access, and shared borders with countries in which polio is endemic. Approximately 3.5 million children were vaccinated in these campaigns. High-quality implementation of SIAs has occurred in Somalia and Sudan despite continuing armed conflict in those countries. In Somalia, during lulls in fighting, a "rapid access" SIA strategy has been implemented in which vaccinators have worked independently to target small populations in a short time. In Sudan, which has experienced civil war for 34 years, SIAs in areas controlled by the government have been coordinated successfully with SIAs in areas in the south not controlled by the central government. During 2000--2001, lulls in fighting allowed implementation of SIAs for the first time in the Nuba Mountains and southern Blue Nile areas of Sudan. Acute Flaccid Paralysis SurveillanceSince 2001, Ethiopia, Somalia, and Sudan have exceeded the WHO-established target for a nonpolio acute flaccid paralysis (AFP) rate indicative of sensitive surveillance (i.e., >1 per 100,000 population aged <15 years) (Table). These countries did not meet the WHO target measure of adequacy of collected stool specimens (i.e., > 80%) in 2001, although Sudan has met this target in 2002. In 2001, the nonpolio enterovirus isolation rate (target: >10%), a marker of laboratory performance and the integrity of the reverse cold chain for specimens, was 25% for Ethiopia, 17% for Sudan, and 16% for Somalia. AFP surveillance in Ethiopia, Somalia, and Sudan is facilitated by staffs comprising trained polio eradication officers. In Ethiopia, 19 staff members are posted throughout the country. In Somalia, which has not had a functioning central government since 1991, UNICEF and WHO have deployed 164 full-time national and international staff in all districts to assist with surveillance and SIAs. In Sudan, 44 persons have been deployed in the north and 230 in the south, a large area lacking infrastructure and experiencing conflict. In addition to polio eradication duties, staff conduct limited activities in the surveillance of other vaccine-preventable diseases (e.g., measles) and participate in the early-warning network for other major infectious diseases. Wild Poliovirus IncidenceThe last reported wild poliovirus--positive cases in Ethiopia and Sudan occurred in January and April of 2001, respectively (Figure). Both polioviruses were type 1. In 2000, Ethiopia reported 155 confirmed polio cases, three of which were confirmed virologically, and Sudan reported 79 cases, four of which were confirmed virologically. In Somalia, 96 cases were reported in 2000; 46 were confirmed virologically, 42 (92%) of which occurred in the capital city, Mogadishu. In 2001, seven virologically confirmed cases were identified in the heavily populated Mogadishu area (Lower Shabelle and Banadir). During 2002, three virologically confirmed cases have been identified in Somalia (most recently in October); all of these cases occurred in the Mogadishu area (Lower Shabelle, Middle Shabelle, and Banadir). Reported by: Country Offices for Ethiopia, Somalia, and Sudan, World Health Organization. Polio Eradication Programme, Regional Office for the Eastern Mediterranean, World Health Organization, Cairo, Egypt. Vaccines and Biologicals Dept, World Health Organization, Geneva, Switzerland. Div of Viral and Rickettsial Diseases, National Center for Infectious Diseases; Global Immunization Div, National Immunization Program, CDC. Editorial Note:Since January 2001, substantial progress has been made toward polio eradication in Ethiopia, Somalia, and Sudan. Ethiopia and Sudan have not reported a polio case in >1 year, and transmission in Somalia appears limited to the Mogadishu area. These achievements have been the result of substantial efforts by the countries with the support of the international public- and private-sector partnership for polio eradication. Progress toward polio eradication in Somalia and Sudan demonstrates that eradication strategies can be implemented successfully even in areas with poor access and ongoing conflict. Cease-fire agreements have allowed access to children previously unreached by health services. National capacity has been strengthened to address other diseases by building disease reporting and surveillance systems and by developing national human resources through training. The program has developed a platform to provide countrywide health services by establishing an extensive system to access children. Key challenges to the eradication programs include improving the quality of SIAs and surveillance. Countries classified as polio-free should maintain high levels of polio vaccination coverage and surveillance to ensure interruption of virus transmission and provide a barrier against virus importation. Program activities should be strengthened in the Somali and Afar regions of Ethiopia bordering Somalia; weak or absent health infrastructures in these regions have resulted in low vaccination coverage and inadequate AFP surveillance. Although reaching children in conflict-affected areas (including the Mogadishu area) is difficult, access must be secured to interrupt wild poliovirus transmission. The close collaboration between WHO and UNICEF, which has been of critical importance in Somalia, should continue. To enhance eradication activities, countries must provide the necessary technical support and maintain political commitment as polio incidence declines and attention turns to other pressing health needs. In April 2002, the Global Technical Consultative Group for Poliomyelitis Eradication identified the greatest challenge to polio eradication as securing the necessary financial resources (5). To support continuing high-quality polio eradication activities in Ethiopia, Somalia, and Sudan, WHO and UNICEF will require an estimated $50 million in 2003. Efforts to support polio eradication programs will continue. Independent technical advisory groups will meet, and managerial reviews will be conducted in each country to monitor progress and provide guidance. Before regional certification of polio eradication, laboratory containment of wild polioviruses must be achieved. WHO is assisting countries in developing and implementing national plans for laboratory containment of poliovirus (6), and the polio-free countries of Ethiopia and Sudan have begun the containment process. Substantial trained personnel and infrastructure have been established in Ethiopia, Somalia, and Sudan through polio eradication programs, particularly in Somalia and Sudan; this infrastructure will be available after polio eradication to address other important health issues, and planning will be needed to ensure optimal use. References
*Nationwide mass campaigns during a short period (days to weeks) in which 2 doses of OPV are administered to all children (usually aged <5 years), regardless of previous vaccination history, with an interval of 4--6 weeks between doses.
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to [email protected].Page converted: 11/27/2002 |
|||||||||
This page last reviewed 11/27/2002
|