|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
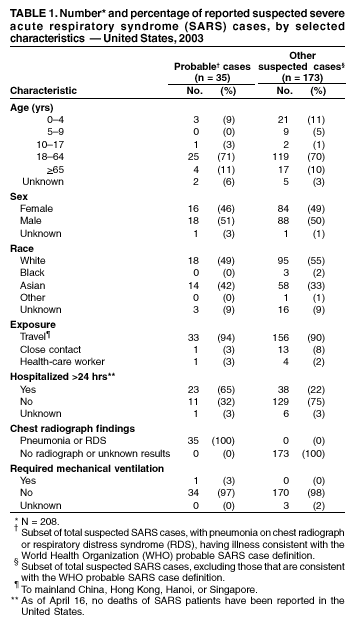
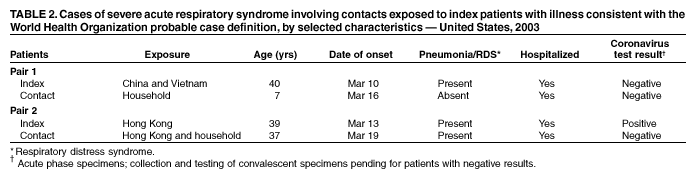
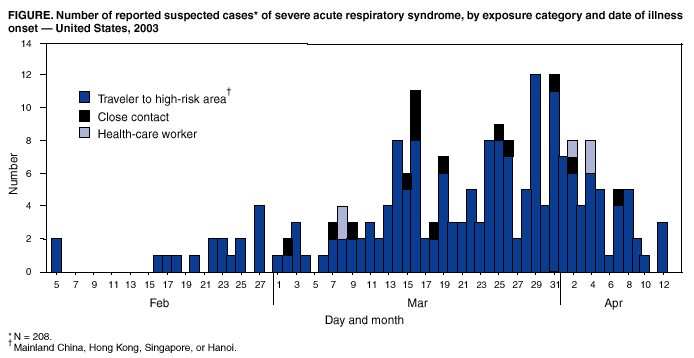
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail. Update: Severe Acute Respiratory Syndrome --- United States, 2003CDC and the World Health Organization (WHO) are continuing to investigate the multicountry outbreak of severe acute respiratory syndrome (SARS). This report updates information on reported SARS cases among U.S. residents and summarizes information on patients with no recent travel outside the United States. During November 1, 2002--April 16, 2003, a total of 3,293 SARS cases were reported to WHO from 22 countries, including the United States; 159 deaths (case-fatality proportion: 4.8%) have been reported (1). WHO-defined areas where local chains of transmission have been identified include regions of China (Beijing; Hong Kong Special Administrative Region; and Guangdong, Shanxi, and Taiwan provinces), Singapore, Vietnam (Hanoi), Canada (Toronto), United Kingdom (London), and the United States (2). Taiwan province, London, and the United States are considered by WHO to be areas with limited local transmission (i.e., no reported transmission other than close person-to-person contact with a known SARS patient). In the United States, as of April 17, a total of 208 suspected SARS cases were reported to CDC from 34 states (Figure). Of these, 35 (17%) had illness consistent with the WHO case definition for probable SARS which requires the presence of pneumonia or acute respiratory distress syndrome (RDS) (3), and the remaining 173 ( 83%) had fever and milder respiratory symptoms (Table 1). Of the 35 probable patients, 33 (94%) had traveled to mainland China, Hong Kong, Singapore, or Hanoi; one (3%) was a health-care worker (HCW) who provided care to a SARS patient, and one (3%) was a household contact of a SARS patient. As previously reported, five of these 33 patients, all of whom were travelers, had laboratory evidence of recent infection with a novel coronavirus (4). Although no additional coronavirus infections have been documented among other U.S. suspected SARS cases, collection and testing of convalescent sera (i.e., sera obtained >21 days after illness onset) for coronavirus infection is ongoing. SARS Patients with No History of Recent Travel Outside the United StatesA total of 19 U.S. residents reported with SARS have no history of travel to mainland China, Hong Kong, Singapore, or Hanoi. All reported close contact with a SARS patient who had traveled recently to one or more of these areas. Five of these cases occurred among HCWs who were exposed to a suspected SARS patient and either did not use personal protective equipment or removed it while examining the patient; in only one instance was the SARS patient provided a surgical mask. Among the 19 close contacts, two had illness consistent with the WHO case definition for a probable case, four required hospitalization, and none is currently hospitalized. Ten have had acute specimens that tested negative for the novel coronavirus. One patient also has had a negative convalescent serum. These 19 patients were close contacts of 16 index patients. Of the 16 index patients, one (6%) tested positive for coronavirus infection, three (19%) have had a negative serologic test on a convalescent specimen; results from 12 (75%) are pending. Two (11%) index patients had illness consistent with the WHO definition of a probable SARS case; the two instances of local transmission in the United States involving these patients are summarized (Table 2). Local Transmission Pair 1. During February 23--March 9, a U.S. resident aged 40 years traveled to mainland China and Hanoi. On March 10, the traveler had fever, cough, and shortness of breath. A chest radiograph revealed pneumonia, and the patient was hospitalized during March 15--16. On March 16, his child aged 7 years had fever and cough. Although the child's chest radiograph did not show evidence of pneumonia, the child was hospitalized for observation and evaluation. Local Transmission Pair 2. During March 1--6, a man aged 39 years traveled to Hong Kong with his wife and stayed in Hotel M, which has been epidemiologically linked to many of the initial SARS cases (4). On March 13, he had fever and respiratory symptoms and was subsequently hospitalized with pneumonia. He tested positive for the novel coronavirus. On March 19, a total of 13 days after return from Hong Kong, his wife became ill and was subsequently hospitalized with radiographic evidence of pneumonia. Reported by: State and local health departments. SARS Investigative Team, CDC. Editorial Note:The primary focus of SARS surveillance activities in the United States is early identification and isolation of patients who have suspected SARS. Many suspected SARS patients in the United States have had relatively mild illness and have not required hospitalization or chest radiographs. The majority of these reported patients are not likely to have the novel coronavirus infection, as respiratory illness is common in travelers (5,6). A small number of persons reported with SARS in the United States had more severe illness that was consistent with the WHO case definition of probable SARS. Cases reported to WHO from other countries are probable SARS cases, whereas the United States has reported all of its suspected cases (7). In the United States, local transmission of suspected SARS has been limited to HCWs and close contacts of suspected SARS patients who were travelers. Identifying persons who might be at risk for SARS on arrival to a medical facility or office is difficult and requires changes in the way medical evaluations are conducted. Revised interim guidelines for triage recommend that all patients in ambulatory-care settings be screened promptly for fever, respiratory symptoms, recent travel, and close contact with a suspected SARS patient (8). CDC has provided guidance to state and local health departments for conducting surveillance of HCWs following exposure to a SARS patient. To prevent secondary transmission, close contacts of SARS patients should be vigilant for fever or respiratory symptoms. If such symptoms develop, exposed persons should avoid contact with others, seek immediate medical attention, and practice infection-control precautions recommended for SARS patients (9). Household members and other close contacts of SARS patients should be actively monitored by the local health department for illness. CDC continues to develop and refine laboratory testing for the novel coronavirus that has been implicated as the cause of SARS and has recently published the nucleic acid sequence of the genome (10). Incorporating laboratory evidence of coronavirus infection into the case definition will be important to characterize the clinical manifestations of coronavirus infection and understand the relation between infection with this novel coronavirus and SARS. References
Table 1
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to [email protected].Page converted: 4/17/2003 |
|||||||||
This page last reviewed 4/17/2003
|