 |
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail. Transmission of Hepatitis B and C Viruses in Outpatient Settings --- New York, Oklahoma, and Nebraska, 2000--2002Transmission of hepatitis B virus (HBV) and hepatitis C virus (HCV) can occur in health-care settings from percutaneous or mucosal exposures to blood or other body fluids from an infected patient or health-care worker. This report summarizes the investigation of four outbreaks of HBV and HCV infections that occurred in outpatient health-care settings. The investigation of each outbreak suggested that unsafe injection practices, primarily reuse of syringes and needles or contamination of multiple-dose medication vials, led to patient-to-patient transmission. To prevent transmission of bloodborne pathogens, all health-care workers should adhere to recommended standard precautions and fundamental infection-control principles, including safe injection practices and appropriate aseptic techniques. In the four investigations, a case of acute HBV infection was defined on the basis of a positive test for IgM antibody to hepatitis B core antigen. A case of past or current HCV infection was defined on the basis of a confirmed positive test for HCV RNA or for antibody to HCV; patients known to have been infected before visiting the health-care facility were excluded. Patients with chronic or acute infection were considered to be potential sources for transmission to susceptible patients. Patients were categorized as having clinic-acquired infection on the basis of evidence that included epidemiologic findings, temporal associations between patients and procedures, documented seroconversion, signs and symptoms of acute viral hepatitis, traditional risk factors for HBV or HCV infection, or genetic relatedness among viral isolates. HCV Transmission in a Private Physician's Office --- New York City In May 2001, a physician notified the New York City Department of Health (NYCDOH) of seven patients who had acute HCV infections after undergoing endoscopic procedures at the same office in March 2001. The office voluntarily ceased performing such procedures in late April 2001. During the 9-day period encompassing the procedure dates of these seven patients, 68 patients underwent procedures in this practice. Among 61 (90%) patients who were tested, five additional acute HCV infections were identified, and a chronic infection in a patient whose procedure preceded the 12 acute HCV cases was identified. All 12 patients had a procedure performed within 3 days after the chronically infected patient. This chronically infected patient and six of the acutely infected patients had HCV genotype information available; all were genotype 2c, which is rare in the United States (1). On the basis of these results, patients who underwent endoscopic procedures since the office opened in January 2000 were notified and offered testing for HCV, HBV, and human immunodeficiency virus (HIV). Results were available for 1,315 (60%) of 2,192 eligible patients; seven additional patients were identified as having HCV infections that probably were acquired in the office. No evidence of HIV transmission was observed; HBV infection was noted among some patients, but epidemiologic links among such office patients could not be established. A retrospective case-control study indicated that clinic-acquired HCV infection was not associated with type of endoscopic procedure, specific endoscope used, whether a biopsy was performed, type of biopsy, or anesthesia type or dose. However, the investigation revealed inappropriate infection-control and injection practices, which indicated that the probable route of transmission was contamination of multiple-dose anesthesia medication vials. In April 2002, after corrections to infection-control practices were made by the office, the New York State Department of Health allowed the office to resume gastrointestinal procedures. HBV Transmission in a Private Physician's Office --- New York CityIn December 2001, NYCDOH was informed of two elderly patients (aged >75 years) who had acute HBV infection diagnosed and who had visited the office of the same physician (physician A) during their incubation periods. A preliminary investigation by NYCDOH identified 19 additional cases of acute HBV infection. On the basis of these results, NYCDOH offered testing for HBV, HCV, and HIV infection to 1,042 patients of physician A; 38 patients, including the 19 previously identified, had acute HBV infection during February 2000--February 2002. HBV DNA genetic sequences of 24 patients with acute infection and four patients with chronic infection were identical in the 1,500--base-pair region examined. No evidence of HCV or HIV transmission was observed. A retrospective cohort study was conducted among the 275 patients attending physician A's office during the 10 months preceding outbreak detection. Of 91 patients with serologic results and available medical records that were included in the cohort study, 18 were infected. Among 67 patients who received at least one injection, 18 (27%) had acute HBV infection, compared with none who received no injections (relative risk [RR] = 13.6; 95% confidence interval [CI] = 2.4--undefined). Patients with HBV infection received a median of 14 injections (range: 2--25), compared with susceptible patients, who received a median of two injections (range: 0--17) (p<0.001). Typically, injections included doses of atropine, dexamethasone, and vitamin B12 drawn from multiple-dose vials into one syringe. The same workspace was used to prepare, dismantle, and dispose of injection equipment. In December 2001, NYCDOH ordered physician A to stop administering injections. In April 2002, physician A retired and closed his office permanently. In response to this outbreak and the outbreak described above, NYCDOH sent a letter (available at http://home.nyc.gov/html/doh/pdf/chi/ltr22002.pdf) to all city clinicians outlining the need for all staff to adhere to infection-control and bloodborne pathogen precautions, including single use of needles and syringes and appropriate use of multiple-dose vials to prevent cross contamination. HBV and HCV Transmission in a Pain Remediation Clinic --- OklahomaIn August 2002, the Oklahoma State Department of Health (OSDH) was informed of six patients with suspected acute HCV infection who had received treatment from the same pain remediation clinic. A preliminary investigation by OSDH found that a certified registered nurse anesthetist (CRNA) reused needles and syringes routinely during clinic sessions. A single needle and syringe was used to administer each of three sedation medications (Versed® [midazolam HCl], fentanyl, and propofol) to up to 24 sequentially treated patients at each clinic session. These medications were administered through heparin locks that were connected directly to intravenous cannulas. On the basis of these findings, the clinic was closed, and an investigation was initiated. Serologic testing for HCV, HBV, and HIV infection was completed for 793 (87%) of the 908 patients attending the clinic. A total of 69 HCV and 31 HBV infections were identified that probably were acquired in the clinic; no HIV infections were identified. Receiving treatment during a clinic session after a patient who was anti-HCV--positive was a statistically significant risk factor for acquiring HCV infection (RR = 9.2; 95% CI = 3.7--22.5). Receiving treatment after a patient who was hepatitis B surface antigen--positive was a significant risk factor for acquiring HBV infection (RR = 8.5; 95% CI = 4.2--17.0). In June 2002, before this investigation, the CRNA ceased reuse of needles after a complaint was filed by staff nurses. After June 2002, no evidence of HBV or HCV transmission associated with receiving treatment at the clinic was found. The state board of nursing revoked the CRNA's license and imposed a $99,000 fine. In response to this outbreak, the American Association of Nurse Anesthetists (AANA) sent mailings to all AANA members and students, nurse anesthesia school program directors, and hospital administrators reminding them that needles and syringes are single-use items and should not be reused. HCV Transmission in a Hematology/Oncology Clinic --- NebraskaIn September 2002, a gastroenterologist reported four patients with recently diagnosed HCV infection to the Nebraska Health and Human Services System (NHHSS). All of these patients had received chemotherapy at the same hematology/oncology clinic. A preliminary investigation identified 10 cases of recently diagnosed HCV infection among clinic patients. Of the six patients for whom HCV genotype was available, all were genotype 3a, which is rare in the United States (1). A patient with a previous diagnosis of chronic HCV genotype 3a infection began attending the clinic in March 2000. The investigation revealed that the health-care worker responsible for medication infusions routinely used the same syringe to draw blood from patients' central venous catheters and to draw catheter-flushing solution from 500-cc saline bags that were used for multiple patients. The clinic staff reported that by July 2001, this practice was corrected through changes in personnel and infection-control practices. NHHSS conducted an investigation among all living patients examined at the clinic during March 2000--December 2001. Of 613 eligible patients, 486 (79%) underwent HCV testing; 99 patients with clinic-acquired HCV infection were identified. HCV genotype information was available for 95 patients; all isolates were genotype 3a. During March 2000--June 2001, 85 (61%) of 139 patients with an implanted central venous catheter became infected with HCV, compared with 14 (6%) of 228 patients without an implanted catheter (RR = 10.0; 95% CI = 5.9--16.8). No evidence of HBV or HIV transmission or of HCV transmission after June 2001 was found. The clinic closed in October 2002. Reported by: S Balter, M Layton, K Bornschlegel, New York City Dept of Health and Mental Hygiene; PF Smith, New York State Dept of Health. M Crutcher, S Mallonee, J Fox, P Scott, Oklahoma State Dept of Health. T Safranek, D Leschinsky, K White, Nebraska Health and Human Svcs System. JF Perz, IT Williams, BP Bell, Div of Viral Hepatitis; L Chiarello, AL Panlilio, Div of Healthcare Quality Promotion, National Center for Infectious Diseases; M Phillips, M Marx, A Macedo de Oliveira, D Comstock, N Malakmadze, T Samandari, TM Vogt, EIS officers, CDC. Editorial Note:These four outbreaks are among the largest health-care--related viral hepatitis outbreaks reported in the United States and share several common characteristics. All occurred in outpatient settings and were reported to public health authorities by clinicians who suspected these infections might have been health-care--related. The investigations were resource-intensive and involved notification, testing, and counseling of hundreds of patients. Transmission probably occurred indirectly from patient to patient after exposure to injection equipment that was contaminated with the blood of one or more source patients. All of these outbreaks could have been prevented by adherence to basic principles of aseptic technique for the preparation and administration of parenteral medications (2--7) (Box). Health-care--related exposures are a well-recognized but uncommon source of viral hepatitis transmission in the United States (7--10). The majority of outbreaks identified previously have been associated with unsafe injection practices, primarily reuse of syringes and needles or contamination of multiple-dose medication vials. However, because the majority of patients with acute HBV or HCV infection are asymptomatic, clusters of patients infected in the health-care setting might be unrecognized. Health-care--related transmission should be suspected when cases are detected among persons without traditional risk factors for infection. State and local health authorities should consider strategies to improve case identification, such as targeting intensive follow-up for persons who typically are at low risk for infection (e.g., persons aged >60 years). In the outbreaks described in this report, health-care workers did not adhere to fundamental principles related to safe injection practices, suggesting that they failed to understand the potential of their actions to lead to disease transmission. In addition, deficiencies related to oversight of personnel and failures to follow up on reported breaches in infection-control practices resulted in delays in correcting the implicated practices. To prevent health-care--related transmission of bloodborne viruses, certification and training programs need to reinforce infection-control principles and practices, including aseptic techniques and safe injection practices. These principles should be reviewed with frequent in-service education for health-care staff, including those who work in outpatient settings, and practices should be monitored as part of the institutional oversight process. Finally, written policies and procedures to prevent patient-to-patient transmission of bloodborne pathogens should be established and implemented among all staff involved in direct patient care. CDC is working with professional organizations, advisory groups, and state and local health departments to address these issues. References
Box 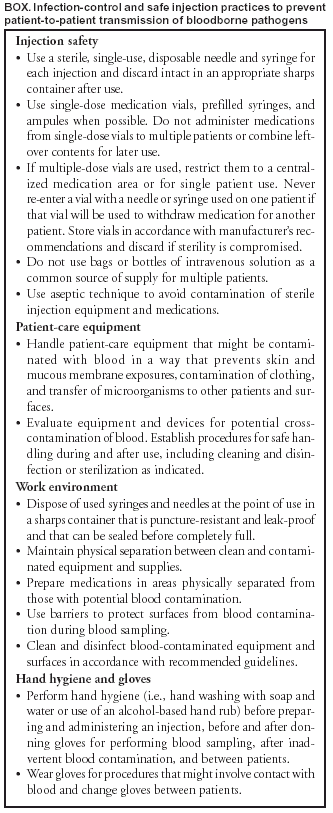 Return to top.
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to [email protected].Page converted: 9/25/2003 |
|||||||||
This page last reviewed 9/25/2003
|