|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
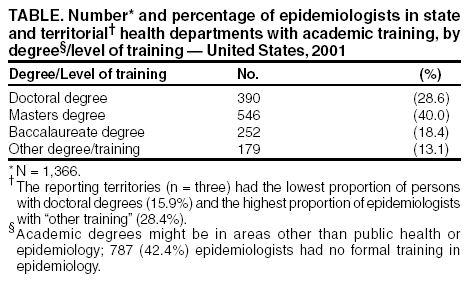
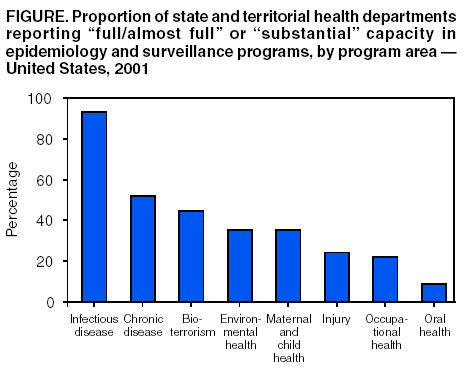
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail. Assessment of the Epidemiologic Capacity in State and Territorial Health Departments --- United States, 2001Epidemiology is essential for the detection, control, and prevention of major health problems. Described as the foundation of all public health functions (1), epidemiology provides information needed to perform the 10 essential public health services (2). One of the national health objectives for 2010 calls for increases in the proportion of tribal, state, and local public health agencies that provide or ensure comprehensive epidemiology services to support essential public health services (objective 23-14) (3). Although national infectious disease capacity has been assessed (4--6), no comprehensive national assessment of epidemiologic capacity has been conducted. To assess core epidemiology and infectious disease capacity of public health departments, the Council of State and Territorial Epidemiologists (CSTE) surveyed state and territorial health departments in November 2001 (7), immediately before the release of approximately $1 billion in federal funding to state health departments for terrorism and public health emergency preparedness. This report summarizes the results of that survey, which indicate that the national epidemiology infrastructure in state and local health departments is far below optimal capacity and that approximately 42% of epidemiologists working in public health have no formal epidemiologic training. Although recent terrorism preparedness initiatives have improved capacity in infectious disease epidemiology, increased resources are needed to build epidemiologic capacity necessary to address the major causes of morbidity and mortality. In October 2001, a draft version of the Epidemiology Capacity Assessment (ECA) was piloted in 10 states. In November, the final version was sent electronically and by mail to the 50 states, the District of Columbia, and the five territories. Responses were received during November 2001--April 2002. ECA included general questions about the epidemiology workforce and specific questions pertaining to the 10 essential public health services. Of the 108 questions, 22 addressed core epidemiologic capacity, and 86 addressed infectious disease capacity. State epidemiologists were identified as key informants, and follow-up was made by telephone and e-mail to nonresponding states. A total of 41 states and three territories (78.6%) responded to the survey. As of November 2001, responding state and territorial health departments employed 1,366 persons as epidemiologists in all program areas; 652 (47.7%) worked in infectious disease programs, and <50 worked in each of the areas of injury epidemiology, occupational epidemiology, or oral health. A total of 77 (5.6%) persons were former CDC Epidemic Intelligence Service (EIS) officers. Among persons employed as epidemiologists in state health departments, the level of training varied substantially (Table); 787 (42.4%) persons had no formal training in epidemiology. Formal training included either academic coursework or other training in epidemiology (e.g., the EIS program). The median total state (n = 26) expenditure for all epidemiology programs was $2.7 million (interquartile range [IQR]: $1.15 million--$6.6 million), with a median per-capita expenditure of $0.70 (IQR: $0.31--$1.73). Federal sources provided 61.3% and state sources 36.6% of funding for all epidemiology programs in the reporting state and territories (n = 42). States were asked to assess core epidemiologic capacity in eight program areas (i.e., infectious disease, chronic disease, maternal/child health, injury, bioterrorism/emergency management, environmental health, oral health, and occupational health) by using a four-point scale* based on the estimated percentage of the activity or resource described in the question that was met (Figure). In addition, states were asked to assess the four essential public health services with a substantial epidemiologic component. "Partial" or "minimal to no" capacity was reported by 24 (54.5%) respondents in monitoring health status to identify and solve community health problems; 17 (39.5%) in diagnosing and investigating health problems and health hazards in the community; 32 (72.7%) in evaluating effectiveness, accessibility, and quality of personal and population-based services; and 41 (93.2%) in conducting research for new insights and innovative solutions to health problems. States' self-assessed capacity for conducting the 10 essential services varied substantially. Although 31 (72.1%) states reported "full/almost full" capacity to monitor all diseases under the Nationally Notifiable Disease Surveillance System, only eight (18.6%) states had "full/almost full" capacity for analysis and reporting of data from the 24 different databases (e.g., emergency rooms, poison control centers, or Medicaid) mentioned in the survey. Few states and territories reported having "full/almost full" capacity to maintain surveillance systems for health outcomes related to emergencies, including four (9.3%) for bioterrorism events, two (4.8%) for radiologic events, and three (7.5%) for environmental or other hazardous substances; no respondents reported "full/almost full" surveillance capacity for incendiary devices or natural disasters. A total of 28 (63.6%) states and territories reported having "full/almost full" or "substantial" capacity to diagnose and investigate infectious disease problems or health hazards. Nine (20.9%) states and territories reported "full/almost full" or "substantial" capacity to evaluate infectious disease public health programs, and nine (20.5%) reported engaging in applied epidemiologic research and publication. Reported by: ML Boulton, RA Malouin, Bur of Epidemiology, Michigan Dept of Community Health. K Hodge, L Robinson, Council of State and Territorial Epidemiologists. Editorial Note:A 1992 CSTE survey of 51 state and territorial epidemiologists indicated that 1,608 full-time epidemiologists were working in infectious disease epidemiology and surveillance (4). Although the methodology and response rate for ECA differed from those used in the 1992 study, results from the 2001 survey suggest that the number of epidemiologists in state and territorial health departments probably had declined. Because of the expansion in the scope of responsibility for epidemiology over this same period, the majority of state and territorial epidemiologists who responded to the survey reported an insufficient number of staff and resources. The finding that approximately 42% of epidemiologists in state health departments lacked any formal training in epidemiology indicates a large training gap in the public health workforce. Professionals (e.g., nurses, sanitarians, health educators, or disease intervention specialists) who might lack training in epidemiology accounted for approximately one third of this workforce. The findings indicate the need to better define what combination of skills, education, and training is sufficient for the designation of epidemiologist. CSTE, in collaboration with CDC and the Association of Schools of Public Health, recently launched an epidemiology fellowship initiative to increase the number of trained public health epidemiologists (8). To enhance state and local health departments' response to public health emergencies, CDC has placed 12 former EIS officers in the newly established Career Epidemiology Field Officer (CEFO) program. Increased continuing education opportunities for the current workforce should be developed. In addition, schools of public health, many of which have a public health practice office, should encourage more epidemiology graduates to apply for positions in state or local health departments. Addressing the scarcity of trained epidemiologists in the area of noninfectious disease is especially critical. States reported their capacities to be inadequate for all epidemiology program areas except infectious disease. Although recent bioterrorism funding initiatives have improved capacity in infectious disease epidemiology (9), other program areas also need support to build infrastructure. Epidemiology capacity remains inadequate for performing the 10 essential public health services. Because of state budget deficits, additional resources for increased epidemiologic capacity must be identified. Although much of the focus of epidemiologists is terrorism preparedness, the goal of the new epidemiology training programs is a larger and better educated workforce prepared to respond to multiple public health problems, including emerging infectious diseases and chronic diseases (10). References
* "Full/almost full": 75%--100% of activity or resource described in the question is met; "substantial": 50%--75%; "partial": 25%--50%; or "minimal to no": <25%.
Table
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to [email protected].Page converted: 10/30/2003 |
|||||||||
This page last reviewed 10/30/2003
|