 |
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
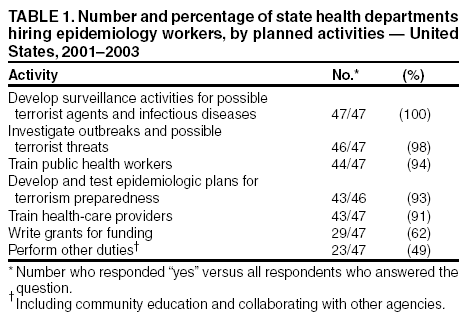
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail. Terrorism Preparedness in State Health Departments --- United States, 2001--2003The anthrax attacks in fall 2001 highlighted the role of infectious disease (ID) epidemiologists in terrorism preparedness and response. Beginning in 2002, state health departments (SHDs) received approximately $1 billion in new federal funding to prepare for and respond to terrorism, infectious disease outbreaks, and other public health threats and emergencies (1). This funding is being used in part to improve epidemiologic and surveillance capabilities. To determine how states have used a portion of their new funding to increase ID epidemiology capacity, the Iowa Department of Public Health's Center for Acute Disease Epidemiology and the Iowa State University Department of Microbiology conducted two surveys of U.S. state epidemiologists during September 2000--August 2001 and October 2002--June 2003. This report summarizes the results of these surveys, which determined that although the number of SHD epidemiology workers assigned to ID and terrorism preparedness increased by 132%, concerns remained regarding the ability of SHDs to hire qualified personnel. These findings underscore the need to develop additional and more diverse training venues for current and future ID epidemiologists. All 50 SHDs responded to both surveys. A total of 47 SHDs reported adding or expecting to add ID epidemiologists, who were assigned various responsibilities (e.g., terrorism preparedness, ID and terrorist agent surveillance, outbreak and possible terrorist threat investigation, public health worker and health-care provider training, and grant writing) (Table 1). Overall, during 2001--2003, the number of epidemiology workers employed in ID and terrorism preparedness increased by 132%, from 366 to 848 (Table 2). Despite these hiring increases, the surveys identified multiple challenges, including problems 1) allocating time for planning (66% of responding SHDs), 2) establishing disease surveillance systems (55%), and 3) hiring qualified ID epidemiologists (57%). Other challenges to preparedness included the complexity of food-security issues, state hiring freezes and budget deficits, political and public policy considerations, and difficulty allocating the necessary time and resources for the pre-event smallpox vaccination program. Reported by: G Shipp, MPA, J Dickson, PhD, Iowa State Univ, Ames; P Quinlisk, MD, C Lohff, MD, Iowa Dept of Public Health, Des Moines, Iowa. N Franklin, 2002 Knight Public Health Journalism Fellowship Program, CDC Foundation, CDC. Editorial Note:Long before the terrorist attacks of September 11, 2001, and the subsequent anthrax attacks, public health officials recognized that the U.S. public health infrastructure was not equipped to respond adequately to events of biologic terrorism and other national public health emergencies (2). In 2003, the number of qualified persons employed in microbial threat preparedness remains dangerously low (3). Since 2001, Congress has appropriated increased amounts of funding to improve the overall capacity of state public health departments for terrorism preparedness (1). This funding was key to increasing the number of ID epidemiologists and the surveillance and response capabilities of SHDs. However, barriers to preparedness remain, and continued public, political, and financial support are essential to removing these barriers. The findings in this report are subject to at least two limitations. First, the surveys were conducted during a period when the responsibilities of ID epidemiologists were in rapid transition, making consistent categorizing by utilization difficult. Second, although all SHD workers described in the surveys performed duties related to epidemiology, because of broad differences in academic background and experience, the nature of their roles and abilities were highly variable. The findings in this report reflect concerns expressed by respondents to the national Epidemiology Capacity Assessment (ECA) regarding inadequate epidemiology staff and resources to conduct the 10 essential public health services (4). In the ECA survey, as of November 2001, approximately 42% of epidemiology workers were reported to have had no formal training in epidemiology, underscoring the need for increased curricula and training programs to improve the capabilities of current and future state and locally based ID epidemiologists. References
 Return to top. Table 2  Return to top.
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to [email protected].Page converted: 10/30/2003 |
|||||||||
This page last reviewed 10/30/2003
|